The Association between State Policy Environments and Self-Rated Health Disparities for Sexual Minorities in the United States


Abstract
:1. Introduction
2. Materials and Methods
3. Results
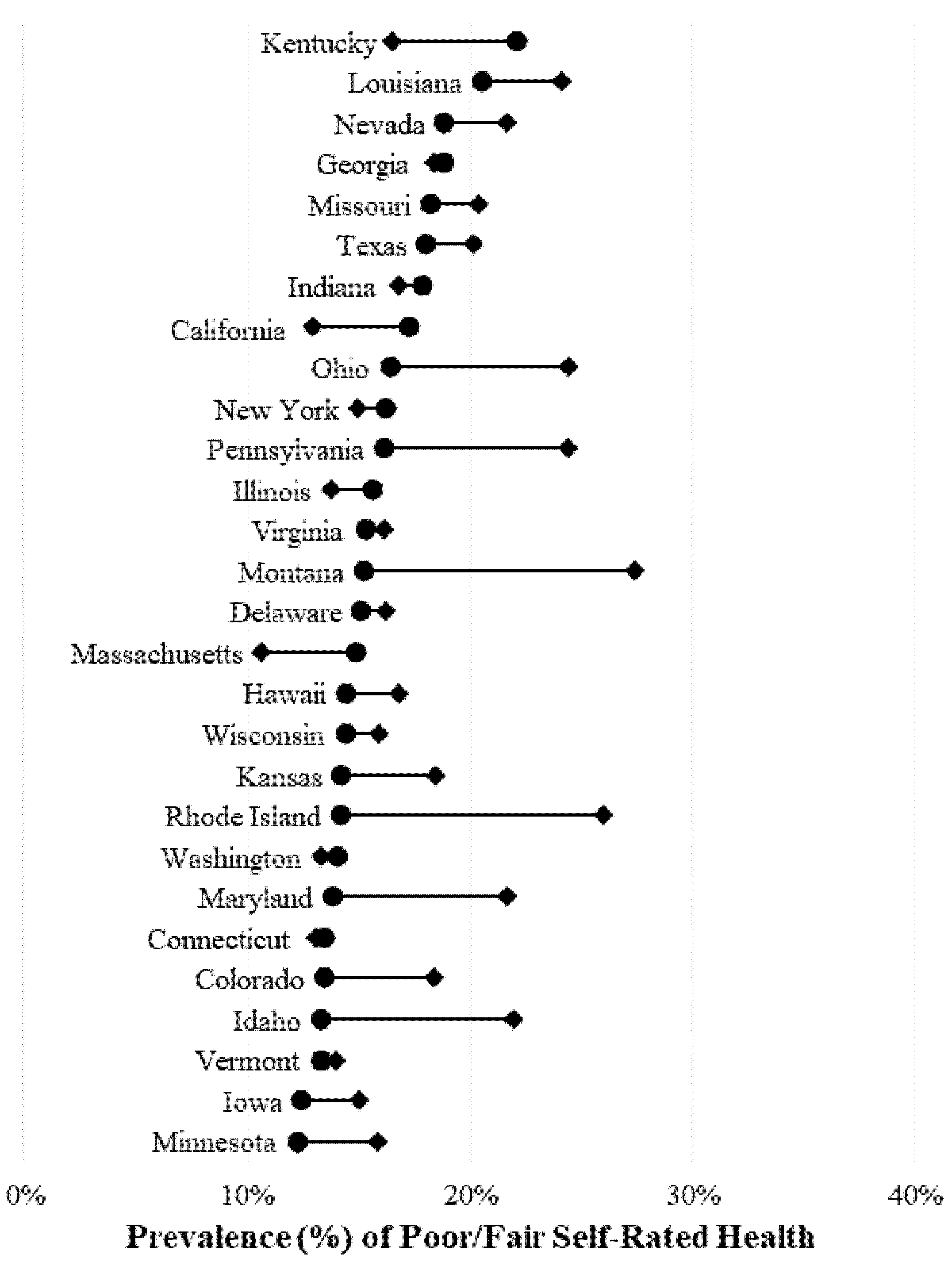
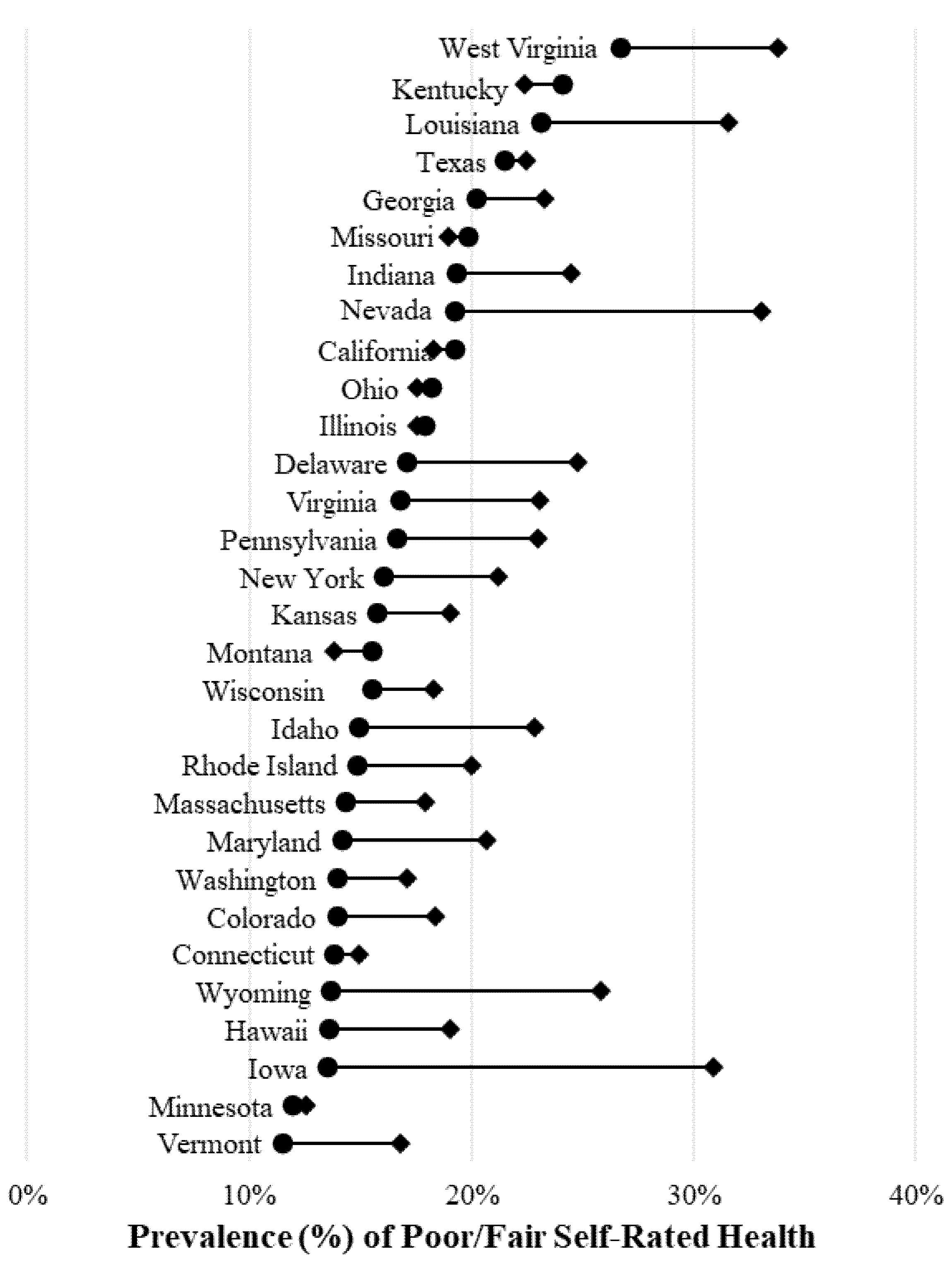
3.1. State-Specific Disparities in Self-Rated Health
3.2. Association between State Policy Environments and Self-Rated Health Disparities
4. Discussion
Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Conron, K.J.; Mimiaga, M.J.; Landers, S.J. A Population-Based Study of Sexual Orientation Identity and Gender Differences in Adult Health. Am. J. Public Health 2010, 100, 1953–1960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzales, G.; Przedworski, J.; Henning-Smith, C. Comparison of Health and Health Risk Factors between Lesbian, Gay, and Bisexual Adults and Heterosexual Adults in the United States: Results from the National Health Interview Survey. JAMA Intern. Med. 2016, 176, 1344–1351. [Google Scholar] [CrossRef] [PubMed]
- Blosnich, J.R.; Farmer, G.W.; Lee, J.G.L.; Silenzio, V.M.B.; Bowen, D.J. Health Inequalities among Sexual Minority Adults. Am. J. Prev. Med. 2014, 46, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.; Henning-Smith, C. Health Disparities by Sexual Orientation: Results and Implications from the Behavioral Risk Factor Surveillance System. J. Commun. Health 2017, 42, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Barnhill, M.M.; Lee, J.G.L.; Rafferty, A.P. Health Inequities among Lesbian, Gay, and Bisexual Adults in North Carolina, 2011–2014. Int. J. Environ. Res. Public Health 2017, 14, 835. [Google Scholar] [CrossRef] [PubMed]
- Daniel, H.; Butkus, R. Lesbian, Gay, Bisexual, and Transgender Health Disparities: Executive Summary of a Policy Position Paper from the American College of Physicians. Ann. Intern. Med. 2015, 163, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.; Blewett, L.A. National and State-Specific Health Insurance Disparities for Adults in Same-Sex Relationships. Am. J. Public Health 2014, 2, e95–e104. [Google Scholar] [CrossRef] [PubMed]
- Dahlhamer, J.M.; Galinsky, A.M.; Joestl, S.S.; Ward, B.W. Barriers to Health Care Among Adults Identifying as Sexual Minorities: A US National Study. Am. J. Public Health 2016, 106, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Minority Stress and Mental Health in Gay Men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef] [PubMed]
- Lick, D.J.; Durso, L.E.; Johnson, K.L. Minority Stress and Physical Health among Sexual Minorities. Perspect. Psychol. Sci. 2013, 8, 521–548. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L. How Does Sexual Minority Stigma “get under the Skin”? A Psychological Mediation Framework. Psychol. Bull. 2009, 135, 707–730. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L.; McLaughlin, K.A.; Keyes, K.M.; Hasin, D.S. The Impact of Institutional Discrimination on Psychiatric Disorders in Lesbian, Gay, and Bisexual Populations: A Prospective Study. Am. J. Public Health 2010, 100, 452–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wight, R.G.; LeBlanc, A.J.; Lee Badgett, M.V. Same-Sex Legal Marriage and Psychological Well-Being: Findings from the California Health Interview Survey. Am. J. Public Health 2013, 103, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Stokols, D. Translating Social Ecological Theory into Guidelines for Community Health Promotion. Am. J. Health Promot. 1996, 10, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Kail, B.L.; Acosta, K.L.; Wright, E.R. State-Level Marriage Equality and the Health of Same-Sex Couples. Am. J. Public Health 2015, 105, 1101–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatzenbuehler, M.L.; Keyes, K.M.; Hasin, D.S. State-Level Policies and Psychiatric Morbidity in Lesbian, Gay, and Bisexual Populations. Am. J. Public Health 2009, 99, 2275–2281. [Google Scholar] [CrossRef] [PubMed]
- Solazzo, A.; Brown, T.N.; Gorman, B.K. State-Level Climate, Anti-Discrimination Law, and Sexual Minority Health Status: An Ecological Study. Soc. Sci. Med. 2018, 196, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G. Association of the New York State Marriage Equality Act with Changes in Health Insurance Coverage. JAMA 2015, 314, 727–728. [Google Scholar] [CrossRef] [PubMed]
- Buchmueller, T.; Carpenter, C.S. The Effect of Requiring Private Employers to Extend Health Benefit Eligibility to Same-Sex Partners of Employees: Evidence from California. J. Policy Anal. Manag. 2012, 31, 388–403. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; O’Cleirigh, C.; Grasso, C.; Mayer, K.; Safren, S.; Bradford, J. Effect of Same-Sex Marriage Laws on Health Care Use and Expenditures in Sexual Minority Men: A Quasi-Natural Experiment. Am. J. Public Health 2012, 102, 285–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System: 2016 Summary Data Quality Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017. [Google Scholar]
- Sell, R.; Holliday, M. Sexual Orientation Data Collection Policy in the United States: Public Health Malpractice. Am. J. Public Health 2014, 104, 967–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dilley, J.A.; Simmons, K.W.; Boysun, M.J.; Pizacani, B.A.; Stark, M.J. Demonstrating the Importance and Feasibility of Including Sexual Orientation in Public Health Surveys: Health Disparities in the Pacific Northwest. Am. J. Public Health 2010, 100, 460–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Fredriksen-Goldsen, K.I. Nonresponse to a Question on Self-Identified Sexual Orientation in a Public Health Survey and Its Relationship to Race and Ethnicity. Am. J. Public Health 2013, 103, 67–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VanKim, N.A.; Padilla, J.L.; Lee, J.G.L.; Goldstein, A.O. Adding Sexual Orientation Questions to Statewide Public Health Surveillance: New Mexico’s Experience. Am. J. Public Health 2010, 100, 2392–2396. [Google Scholar] [CrossRef] [PubMed]
- Gill, A. 2014 State Equality Index; Human Rights Campaign Foundation: Washington, DC, USA, 2015. [Google Scholar]
- Warbelow, S.; Persad, X. 2015 State Equality Index; Human Rights Campaign Foundation: Washington, DC, USA, 2016; Volume 53. [Google Scholar]
- Warbelow, S.; Diaz, B. 2016 State Equality Index; Human Rights Campaign Foundation: Washington, DC, USA, 2016. [Google Scholar]
- Gates, G.J. In US, More Adults Identifying as LGBT. Available online: http://www.gallup.com/poll/201731/lgbt-identification-rises.aspx (accessed on 22 January 2017).
- LaVeist, T.A.; Gaskin, D.; Richard, P. Estimating the Economic Burden of Racial Health Inequalities in the United States. Int. J. Health Serv. 2011, 41, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.G.; Goesling, B.; Avellar, S. The Effects of Marriage on Health: A Synthesis of Research Research Evidence; Mathematica Policy Research, Inc.: Princeton, NJ, USA, 2007; Available online: https://www.mathematica-mpr.com/our-publications-and-findings/publications/the-effects-of-marriage-on-health-a-synthesis-of-recent-research-evidence (accessed on 22 May 2018).
- Orloff, A.S. Gender and the Social Rights of Citizenship: The Comparative Analysis of Gender Relations and Welfare States. Am. Sociol. Rev. 1993, 58, 303–328. [Google Scholar] [CrossRef]
- Orloff, A.S. Gender in the Welfare State. Annu. Rev. Sociol. 1996, 22, 51–78. [Google Scholar] [CrossRef] [Green Version]
- Grant, J.M.; Mottett, L.A.; Tanis, J.; Harrison, J.; Herman, J.L.; Keisling, M. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey; National Center for Transgender Equality and National Gay and Lesbian Task Force: Washington, DC, USA, 2011. [Google Scholar]



{kind=link}
{kind=link}
| Sociodemographic Characteristics | Men | Women | ||||
|---|---|---|---|---|---|---|
| Heterosexual | Sexual Minority | p Value | Heterosexual | Sexual Minority | p Value | |
| (n = 207,562) | (n = 6894) | (n = 282,509) | (n = 7793) | |||
| Total | 96.4 | 3.6 | <0.001 | 96.2 | 3.8 | <0.001 |
| Age, years | <0.001 | <0.001 | ||||
| 18–24 | 12.6 | 21.8 | 10.7 | 31.3 | ||
| 25–34 | 16.2 | 21.7 | 14.7 | 26.3 | ||
| 35–44 | 16.3 | 12.9 | 15.6 | 14.6 | ||
| 45–54 | 17.9 | 18.2 | 17.7 | 12.3 | ||
| 55–64 | 17.5 | 14.3 | 17.7 | 8.0 | ||
| ≥65 | 18.8 | 10.8 | 22.8 | 7.1 | ||
| Missing data | 0.7 | 0.2 | 0.9 | 0.4 | ||
| Race/Ethnicity | 0.01 | <0.001 | ||||
| White | 67.1 | 64.5 | 67.5 | 62.6 | ||
| Black | 10.5 | 10.8 | 12.0 | 13.6 | ||
| Hispanic | 13.2 | 14.0 | 12.5 | 12.9 | ||
| Other/Multiple Races | 7.5 | 9.4 | 6.7 | 9.6 | ||
| Missing data | 1.8 | 1.3 | 1.3 | 1.3 | ||
| Relationship status | <0.001 | <0.001 | ||||
| Married or living with a partner | 58.7 | 32.8 | 55.2 | 36.4 | ||
| Divorced, separated, or widowed | 15.7 | 10.6 | 24.6 | 15.3 | ||
| Never married | 25.1 | 55.8 | 19.8 | 47.7 | ||
| Missing data | 0.5 | 0.8 | 0.4 | 0.6 | ||
| Children in the household | <0.001 | 0.017 | ||||
| None | 64.7 | 80.8 | 61.3 | 58.4 | ||
| At least one child | 34.8 | 18.8 | 38.2 | 41.3 | ||
| Missing data | 0.6 | 0.3 | 0.4 | 0.3 | ||
| Educational attainment | <0.001 | 0.001 | ||||
| Less than high school | 13.3 | 9.9 | 11.9 | 13.6 | ||
| High school graduate | 30.8 | 26.3 | 27.9 | 26.4 | ||
| Some college | 29.2 | 32.3 | 32.7 | 35.7 | ||
| College graduate | 26.4 | 31.2 | 27.3 | 24.1 | ||
| Missing data | 0.3 | 0.3 | 0.2 | 0.2 | ||
| Employment status | <0.001 | <0.001 | ||||
| Employed | 64.5 | 60.6 | 50.5 | 54.9 | ||
| Unemployed | 5.8 | 7.7 | 5.0 | 9.6 | ||
| Not in labor force | 29.0 | 31.1 | 43.9 | 34.8 | ||
| Missing data | 0.7 | 0.5 | 0.6 | 0.8 | ||
| Household income, $ | <0.001 | <0.001 | ||||
| 0–9999 | 3.6 | 5.8 | 4.9 | 8.6 | ||
| 10,000–19,999 | 9.1 | 11.8 | 11.5 | 14.0 | ||
| 20,000–34,999 | 15.6 | 16.8 | 17.1 | 18.8 | ||
| 35,000–49,999 | 12.7 | 13.0 | 11.6 | 11.5 | ||
| 50,000–74,999 | 14.4 | 12.4 | 12.9 | 10.0 | ||
| ≥75,000 | 32.7 | 28.1 | 26.7 | 21.3 | ||
| Missing data | 12.0 | 12.0 | 15.3 | 15.9 | ||
| Chronic disease diagnoses | 0.06 | 0.008 | ||||
| None | 58.2 | 60.8 | 50.6 | 53.1 | ||
| One chronic disease | 23.1 | 21.4 | 26.7 | 26.4 | ||
| Multiple chronic diseases | 15.9 | 14.7 | 20.3 | 17.6 | ||
| Missing data | 2.8 | 3.1 | 2.5 | 2.9 | ||
| Health insurance status | 0.86 | <0.001 | ||||
| Insured | 87.4 | 87.4 | 90.7 | 86.8 | ||
| Uninsured | 12.0 | 11.7 | 8.9 | 12.6 | ||
| Missing data | 0.6 | 0.9 | 0.4 | 0.6 | ||
| Has usual source of care | 0.85 | <0.001 | ||||
| Yes | 68.7 | 69.3 | 78.9 | 69.1 | ||
| No | 30.7 | 30.2 | 20.8 | 30.5 | ||
| Missing data | 0.6 | 0.6 | 0.4 | 0.4 | ||
| Study Sample | Weighted Prevalence (%) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) † | ||
|---|---|---|---|---|---|
| Men in all 31 study states | |||||
| Heterosexual | 16.4 | 1.00 | [Reference] | 1.00 | [Reference] |
| Sexual Minority | 17.4 | 1.07 | (0.95–1.21) | 1.10 | (0.94–1.28) |
| Men in 16 study states with comprehensive protections | |||||
| Heterosexual | 15.4 | 1.00 | [Reference] | 1.00 | [Reference] |
| Sexual Minority | 14.9 | 0.96 | (0.82–1.13) | 0.96 | (0.79–1.16) |
| Men in 15 study states with limited protections | |||||
| Heterosexual | 17.4 | 1.00 | [Reference] | 1.00 | [Reference] |
| Sexual Minority | 20.6 | 1.23 | (1.03–1.47) ** | 1.30 | (1.03–1.64) ** |
| Study Sample | Weighted Prevalence (%) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) † | ||
|---|---|---|---|---|---|
| Women in all 31 study states | |||||
| Heterosexual | 17.7 | 1.00 | [Reference] | 1.00 | [Reference] |
| Sexual Minority | 20.7 | 1.21 | (1.09–1.35) ** | 1.35 | (1.17–1.55) *** |
| Women in 16 study states with comprehensive protections | |||||
| Heterosexual | 16.1 | 1.00 | [Reference] | 1.00 | [Reference] |
| Sexual Minority | 19.5 | 1.26 | (1.08–1.46) ** | 1.44 | (1.19–1.75) *** |
| Women in 15 study states with limited protections | |||||
| Heterosexual | 19.2 | 1.00 | [Reference] | 1.00 | [Reference] |
| Sexual Minority | 22.0 | 1.19 | (1.01–1.40) ** | 1.28 | (1.04–1.57) ** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzales, G.; Ehrenfeld, J.M. The Association between State Policy Environments and Self-Rated Health Disparities for Sexual Minorities in the United States. Int. J. Environ. Res. Public Health 2018, 15, 1136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061136
Gonzales G, Ehrenfeld JM. The Association between State Policy Environments and Self-Rated Health Disparities for Sexual Minorities in the United States. International Journal of Environmental Research and Public Health. 2018; 15(6):1136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061136
Chicago/Turabian StyleGonzales, Gilbert, and Jesse M. Ehrenfeld. 2018. "The Association between State Policy Environments and Self-Rated Health Disparities for Sexual Minorities in the United States" International Journal of Environmental Research and Public Health 15, no. 6: 1136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061136