A Systematic Review of Attention Biases in Opioid, Cannabis, Stimulant Use Disorders

Abstract
:1. Introduction
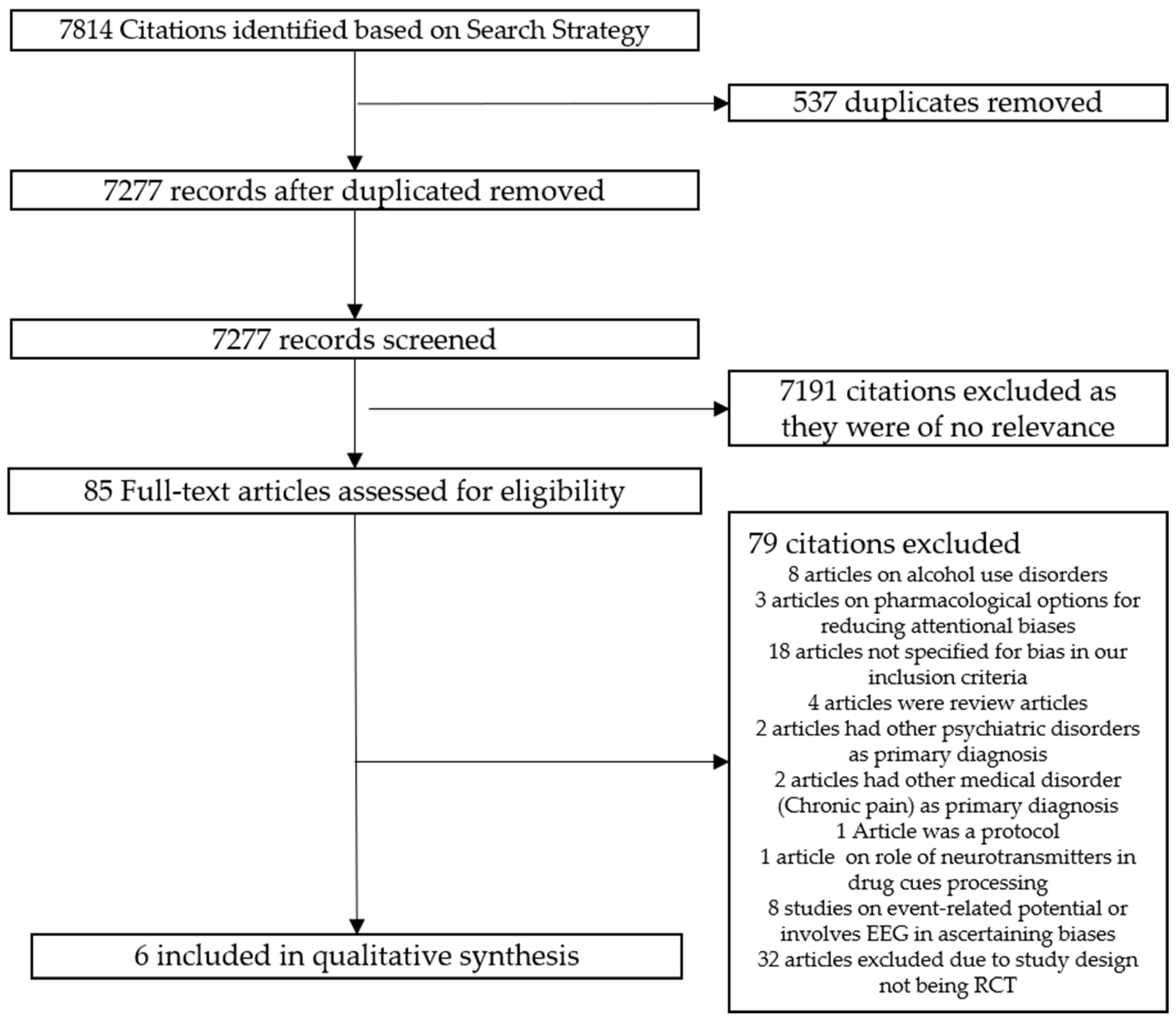
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Selection of Articles
2.3. Statistical Analysis
2.3.1. Extraction
2.3.2. Data Analysis and Synthesis
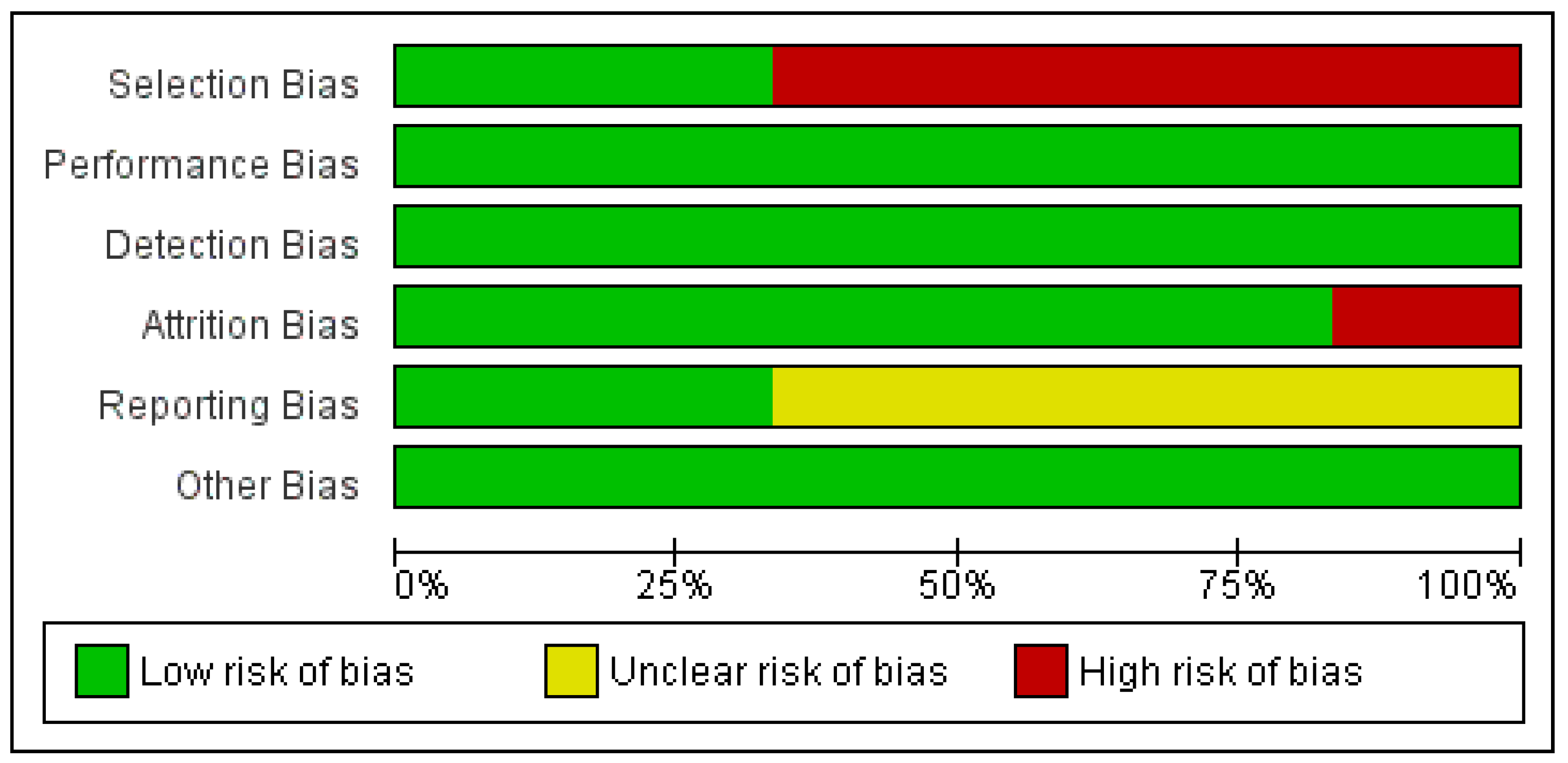
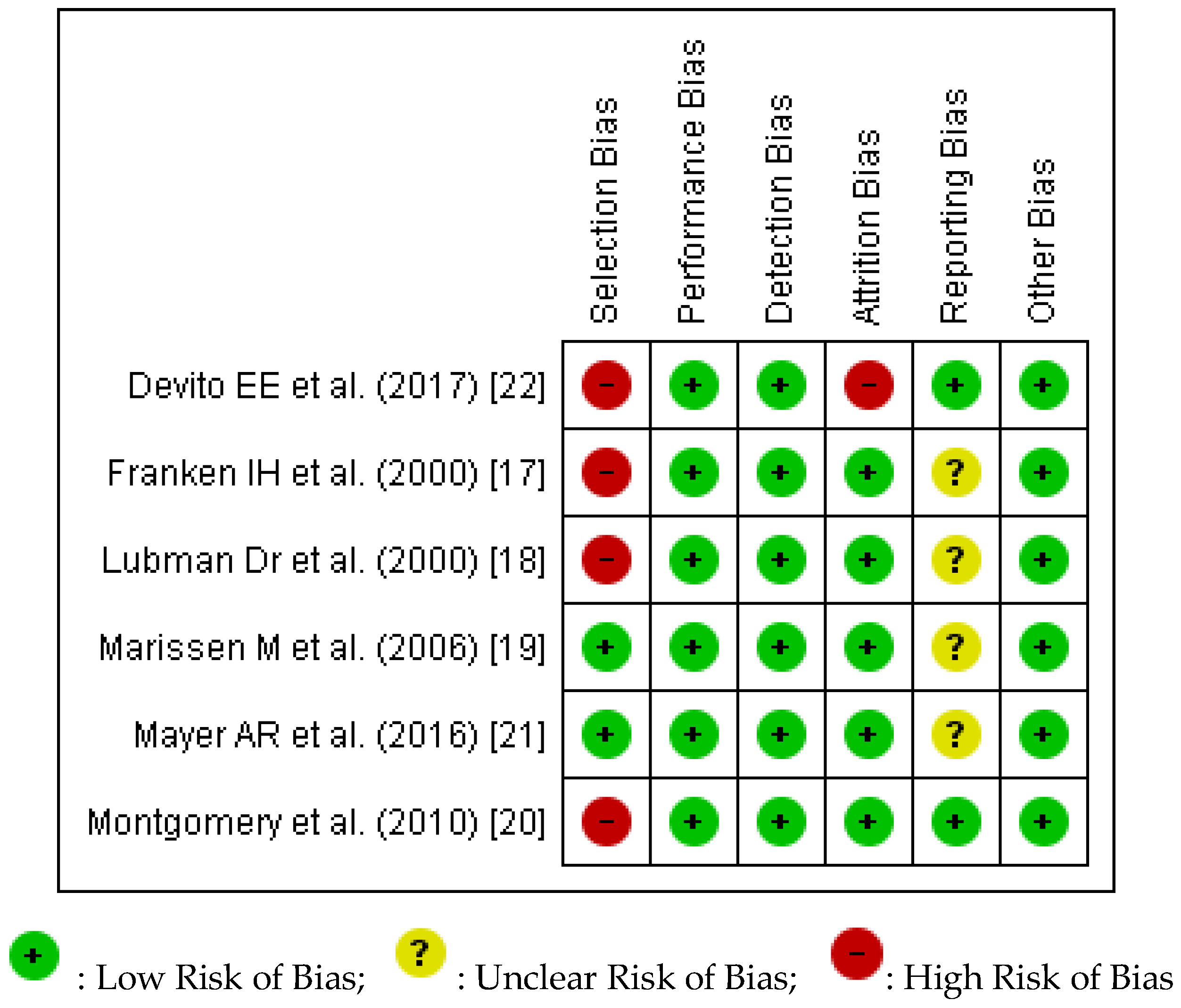
2.3.3. Quality Assessment
3. Results
3.1. Overview of Studies
3.2. Characteristics of Three Studies for Opioid Use Disorders
3.3. Primary and Secondary Outcomes Reported in Three Studies for Opioid Use Disorders
3.4. Characteristics of Three Studies for Stimulant Use (Cocaine) Disorders
3.5. Main Outcomes Reported in Studies for Stimulant Use (Cocaine) Disorders
3.6. Quality and Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations Office on Drugs and Crime. Exexcutive Summary: Conclusions and Policy Implications. Available online: https://www.unodc.org/unodc/en/scientists/world-drug-report-2017---executive-summary-conclusions-and-policy-implications.html (accessed on 12 April 2018).
- European Monitoring Centre for Drugs and Drug Addiction. Perspectives on Drugs: The Role of Psychosocial Interventions in Drug Treatment. Available online: http://www.emcdda.europa.eu/publications/topics/pods/psychosocial-interventions (accessed on 12 April 2018).
- World Health Organization. Clinical Guidelines for Withdrawal Management and Treatment of Drug Dependence in Closed Settings. 2009. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK310654/pdf/Bookshelf_NBK310654.pdf (accessed on 12 April 2018).
- McHugh, R.K.; Hearon, B.A.; Otto, M.W. Cognitive behavioral therapy for substance use disorders. Psychiatr. Clin. N. Am. 2010, 33, 511–525. [Google Scholar] [CrossRef] [PubMed]
- Cutler, R.B.; Fishbain, D.A. Are alcoholism treatments effective? The Project MATCH data. BMC Public Health 2005, 5, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boffo, M.; Pronk, T.; Wiers, R.W.; Mannarini, S. Combining cognitive bias modification training with motivational support in alcohol dependent outpatients: Study protocol for a randomised controlled trial. Trials 2015, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Bechara, A. Decision making, impulse control and loss of willpower to resist drugs: A neurocognitive perspective. Nat. Neurosci. 2005, 8, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Wiers, R.W.; Teachman, B.A.; De Houwer, J. Implicit cognitive processes in psychopathology: An introduction. J. Behav. Ther. Exp. Psychiatry 2007, 38, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Field, M.; Cox, W.M. Attentional bias in addictive behaviors: A review of its development, causes, and consequences. Drug Alcohol Depend. 2008, 97, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Field, M.; Marhe, R.; Franken, I.H. The clinical relevance of attentional bias in substance use disorders. CNS Spectr. 2014, 19, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Leeman, R.F.; Robinson, C.D.; Waters, A.J.; Sofuoglu, M. A critical review of the literature on attentional bias in cocaine use disorder and suggestions for future research. Exp. Clin. Psychopharmacol. 2014, 22, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Wier, R.W.; Gladwin, T.E.; Rinck, M. Should we train alcohol-dependent patients to avoid alcohol. Front. Psychiatry 2013, 4, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristea, I.A.; Kok, R.N.; Cuijpers, P. The Effectiveness of Cognitive Bias Modification Interventions for Substance Addictions: A Meta-Analysis. PLoS ONE 2016, 11, e0162226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christiansen, P.; Schoenmakers, T.M.; Field, M. Less than meets the eye: Reappraising the clinical relevance of attentional bias in addiction. Addict. Behav. 2015, 44, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ying, J.; Song, G.; Ho, R.C.; Fung, D.S.; Smith, H. Attention Bias in Individuals with Addictive Disorders: Systematic Review Protocol. JMIR Res. Protoc. 2018, 7, e41. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Br. Med. J. 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Franken, I.H.; Kroon, L.Y.; Wiers, R.W.; Jansen, A. Selective Cognitive processing of drug cues in heroin dependence. J. Psychopharmacol. 2000, 14, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Lubman, D.I.; Peters, L.A.; Mogg, K.; Bradley, B.P.; Deakin, J.F. Attentional bias for drug cues in opiate dependence. Psychol. Med. 2000, 30, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Marissen, M.A.; Franken, I.H.; Waters, A.J.; Blanken, P.; van den Brink, W.; Hendriks, V.M. Attentional bias predicts heroin relapse following treatment. Addiction 2006, 101, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, C.; Field, M.; Atkinson, A.M.; Cole, J.C.; Goudie, A.J.; Sumnall, H.R. Effects of alcohol preload on attentional bias towards cocaine-related cues. Psychopharmacology 2010, 210, 365–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, A.R.; Wilcox, C.E.; Dodd, A.B.; Klimaj, S.D.; Dekonenko, C.J.; Claus, E.D.; Bogenschutz, M. The efficacy of attention bias modification therapy in cocaine use disorders. Am. J. Drug Alcohol Abus. 2016, 42, 459–468. [Google Scholar] [CrossRef] [PubMed]
- DeVito, E.E.; Kiluk, B.D.; Nich, C.; Mouratidis, M.; Carroll, K.M. Drug Stroop: Mechanisms of response to computerized cognitive behavioral therapy for cocaine dependence in a randomized clinical trial. Drug Alcohol Depend. 2017, 183, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Community. Review Manager, Version 5.3; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Heitmann, J.; van Hemel-Ruiter, M.E.; Vermeulen, K.M.; Ostafin, B.D.; MacLeod, C.; Wiers, R.W.; DeFuentes-Merillas, L.; Fledderus, M.; Markus, W.; de Jong, P.J. Internet-based attentional bias modification training as add-on to regular treatment in alcohol and cannabis dependent outpatients: A study protocol of a randomized control trial. BMC Psychiatry 2017, 17, 193. [Google Scholar] [CrossRef] [PubMed]
- De Hullu, E.; Sportel, B.E.; Nauta, M.H.; de Jong, P.J. Cognitive bias modification and CBT as early interventions for adolescent social and test anxiety: Two-year follow-up of a randomized controlled trial. J. Behav. Ther. Exp. Psychiatry 2017, 55, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Shrier, I.; Boivin, J.F.; Steele, R.J.; Platt, R.W.; Furlan, A.; Kakuma, R.; Brophy, J.; Rossignol, M. Should meta-analyses of interventions include observational studies in addition to randomized controlled trials? A critical examination of underlying principles. Am. J. Epidemiol. 2007, 166, 1203–1209. [Google Scholar] [CrossRef] [PubMed]
- Peinemann, F.; Tushabe, D.A.; Kleijnen, J. Using multiple types of studies in systematic reviews of health care interventions—A systematic review. PLoS ONE 2013, 8, e85035. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Sample Size | Types of Sample | Demographics of Sample | Country | Diagnosis of Sample | Method of Diagnosis | Attention Bias Method | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Franken, I.H. et al. (2000) [17] | Randomised trial | 21 heroin-dependent participants 30 control participants | Participants with heroin dependence were recruited from an inpatient treatment centre Participants in the control group were recruited among clinical and administrative staff in the clinic | 71.4% males (heroin-dependent) 83.3% (control group) Mean age 31.5 years (heroin-dependent) Mean age 34.8 (control group) Mean self-reported duration of heroin dependence was 93.9 months | Netherlands | Heroin Dependence | Based on the DSM-IV criteria for heroin dependence | Drug Stroop task | Higher overall reaction time for heroin participants as compared to control participants Mean pre-experimental craving was 13.8, mean post masked Stroop was 7.19 and mean post unmasked Stroop was 15.2 |
| Lubman, D.I. et al. (2000) [18] | Randomised trial | 16 methadone-maintained opiate addicts 16 age-matched control | Heroin addicts were recruited from local drug services Staff from these services were recruited as controls | Opiate group: mean age 31.4, Male to Female 11:5 Control group: mean age 31.7, male to female 8:8 | United Kingdom | Heroin Dependence | ICD-10 and DSM IV | Pictorial Probe Detection Task | Faster reaction times to probes that replaced drug stimuli, indicative of the presence of an attentional bias |
| Marissen, M. et al. (2006) [19] | Randomised trial | 110 Participants assigned to either cue exposure therapy or placebo psychotherapy | Abstinent heroin addicts who were admitted voluntarily to an in-patient drug-free therapeutic centre in the Hague | 89% males, mean age 34 years old Average age of onset of heroin usage was 21.4 years, most have used heroin for 9.3 years | Netherlands | Heroin Dependence | DSM-IV criteria for heroin dependence | Emotional Stroop Task | Pre-treatment attentional bias predicted relapse at three months follow-up Reduction of attentional biases in both experimental conditions |
| Montgomery et al. (2010) [20] | Randomised trial | 32 regular cocaine users and 40 non-users | Student Population at Liverpool John Moores University and the general population in the surrounding areas | Mean age for cocaine users assigned to placebo 19.29, assigned to alcohol 20.23 Mean age for non-users assigned to placebo 19.59, assigned to alcohol 20.0 13 male in cocaine use group 19 male in non-cocaine use group | United Kingdom | Cocaine dependence | Questionnaire | Visual Probe and Modified Stroop task | Cocaine participants who received alcohol had increased attentional bias for cocaine pictures The cocaine Stroop revealed no differences between cocaine users and non-users, and no effects of alcohol in either group |
| Mayer, A.R. et al. (2016) [21] | Randomised trial | 37 participants assigned to either attentional bias modification therapy (ABMT) or control therapy | Not mentioned | ABMT group: 14 male, and 5 female, mean age 37.4 Control group: 10 male and 8 female, mean age 38.9 | United States | Cocaine dependence | Structured clinical interview for DSM-IV | Visual Probe task | Presence of attentional bias Attentional bias not subjected to modification by ABMT |
| DeVito, E.E. (2017) [22] | Randomised trial | 38 in treatment as usual plus computer-based CBT (CBT4CBT) 41 in treatment as usual | Recruited from community-based outpatient clinic | 46% female, mean age 42.2 | United States | Cocaine use disorder | DSM-IV | Computerized drug Stroop test | Stroop testing revealed that participants who have had a longer duration of cocaine abstinence during treatment (3+ weeks) have greater reductions in Drug Stroop effect. Engagement with CBT4CBT intervention also led to a reduction in Drug Stroop effect |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Ying, J.; Wing, T.; Song, G.; Fung, D.S.S.; Smith, H. A Systematic Review of Attention Biases in Opioid, Cannabis, Stimulant Use Disorders. Int. J. Environ. Res. Public Health 2018, 15, 1138. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061138
Zhang M, Ying J, Wing T, Song G, Fung DSS, Smith H. A Systematic Review of Attention Biases in Opioid, Cannabis, Stimulant Use Disorders. International Journal of Environmental Research and Public Health. 2018; 15(6):1138. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061138
Chicago/Turabian StyleZhang, Melvyn, Jiangbo Ying, Tracey Wing, Guo Song, Daniel S. S. Fung, and Helen Smith. 2018. "A Systematic Review of Attention Biases in Opioid, Cannabis, Stimulant Use Disorders" International Journal of Environmental Research and Public Health 15, no. 6: 1138. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061138