Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study


Abstract
:1. Introduction
2. Material and Methods
2.1. Data Sources
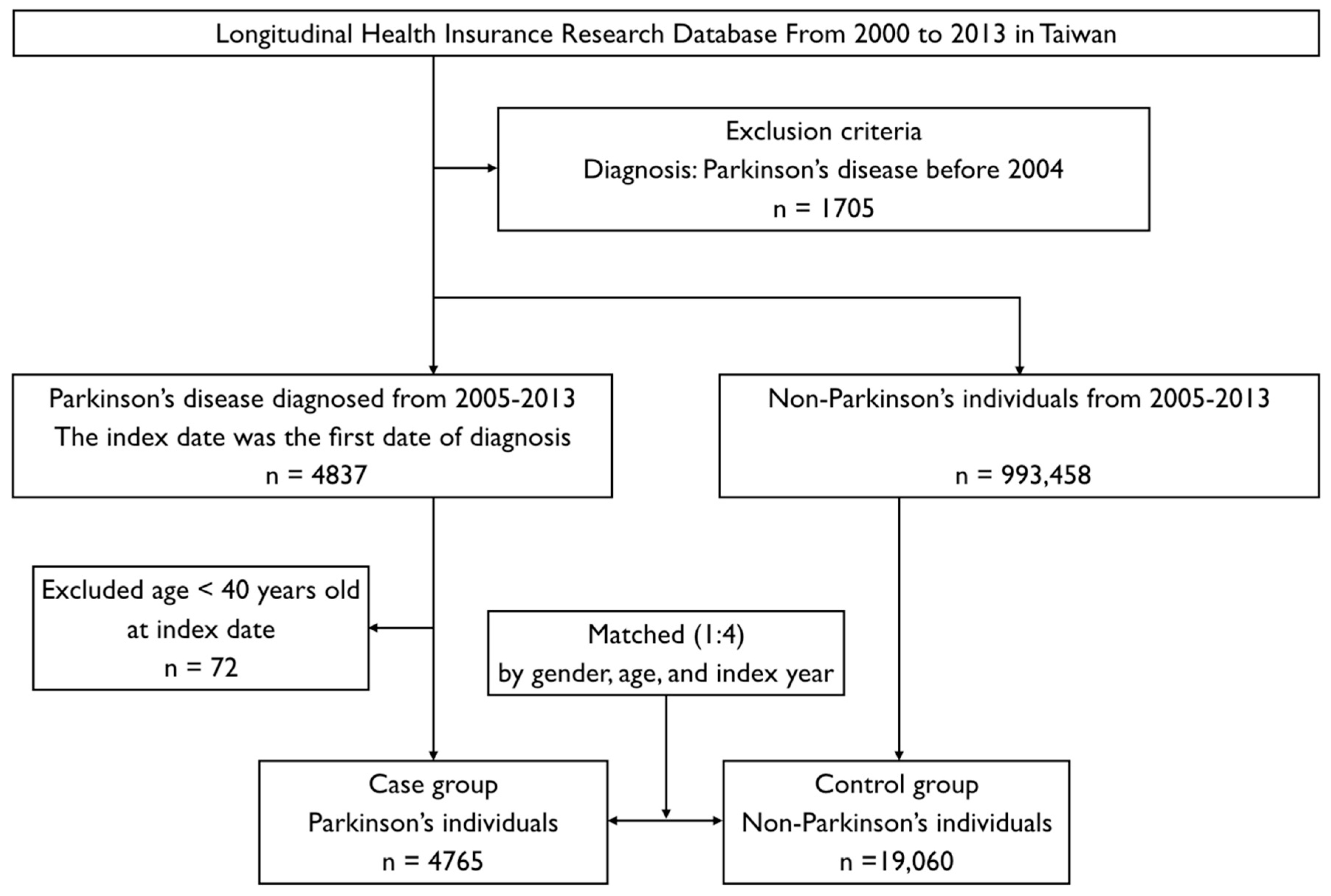
2.2. Study Design and Sampled Individuals
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of interest
References
- Kaur, T.; Uppoor, A.; Naik, D. Parkinson’s disease and periodontitis—The missing link? A review. Gerodontology 2016, 33, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Van Den Eeden, S.K.; Tanner, C.M.; Bernstein, A.L.; Fross, R.D.; Leimpeter, A.; Bloch, D.A.; Nelson, L.M. Incidence of Parkinson’s disease: Variation by age, gender, and race/ethnicity. Am. J. Epidemiol. 2003, 157, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.M.; Wu, R.M.; Lin, J.W.; Liu, Y.C.; Chang, C.H.; Lin, C.H. Time trends in the prevalence and incidence of Parkinson’s disease in Taiwan: A nationwide, population-based study. J. Formos. Med. Assoc. 2016, 115, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Diederich, N.J.; Moore, C.G.; Leurgans, S.E.; Chmura, T.A.; Goetz, C.G. Parkinson disease with old-age onset: A comparative study with subjects with middle-age onset. Arch. Neurol. 2003, 60, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.F.; Wagner, H.N., Jr.; Dannals, R.F.; Links, J.M.; Frost, J.J.; Ravert, H.T.; Wilson, A.A.; Rosenbaum, A.E.; Gjedde, A.; Douglass, K.H.; et al. Effects of age on dopamine and serotonin receptors measured by positron tomography in the living human brain. Science 1984, 226, 1393–1396. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.H.; Lee, W.J.; Chen, Y.H.; Chang, M.H.; Lin, C.H. Premotor Symptoms as Predictors of Outcome in Parkinsons Disease: A Case-Control Study. PLoS ONE 2016, 11, e0161271. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Cappelli, D. Acute-phase reactants in infections and inflammatory diseases. Periodontology 2000 2000, 23, 19–49. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Wu, Y.T.; Chang, Y.C. Periodontal inflammatory disease is associated with the risk of Parkinson’s disease: A population-based retrospective matched-cohort study. PeerJ 2017, 5, e3647. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.G. The effect of subgingival scaling on gingival inflammation. J. Periodontol. 1969, 40, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Ho Chan, W.S. Taiwan’s healthcare report 2010. EPMA J. 2010, 1, 563–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.C.; Wahlqvist, M.L.; Lee, M.S.; Tsai, H.N. Incidence of dementia is increased in type 2 diabetes and reduced by the use of sulfonylureas and metformin. J. Alzheimers Dis. 2011, 24, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Romano, P.S.; Roos, L.L.; Jollis, J.G. Adapting a clinical comorbidity index for use with ICD-9-CM administrative data: Differing perspectives. J. Clin. Epidemiol. 1993, 46, 1075–1079; discussion 1081–1090. [Google Scholar] [CrossRef]
- Tzeng, N.S.; Chung, C.H.; Yeh, C.B.; Huang, R.Y.; Yuh, D.Y.; Huang, S.Y.; Lu, R.B.; Chang, H.A.; Kao, Y.C.; Chiang, W.S.; et al. Are Chronic Periodontitis and Gingivitis Associated with Dementia? A Nationwide, Retrospective, Matched-Cohort Study in Taiwan. Neuroepidemiology 2016, 47, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar]
- Yang, Y.W.; Hsieh, T.F.; Li, C.I.; Liu, C.S.; Lin, W.Y.; Chiang, J.H.; Li, T.C.; Lin, C.C. Increased risk of Parkinson disease with diabetes mellitus in a population-based study. Medicine 2017, 96, e5921. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.P.; Yang, C.J.; Hu, K.F.; Chao, A.C.; Chang, Y.H.; Hsieh, K.P.; Tsai, J.H.; Ho, P.S.; Lim, S.Y. Risk factors for pneumonia among patients with Parkinson’s disease: A Taiwan nationwide population-based study. Neuropsychiatr. Dis. Treat. 2016, 12, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, Z.; Mele, B.; Guo, S.; Hanson, H.; Jette, N.; Patten, S.; Pringsheim, T.; Holroyd-Leduc, J. Guidelines for dementia or Parkinson’s disease with depression or anxiety: A systematic review. BMC Neurol. 2016, 16, 244. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.C.; Chang, C.W.; Lee, H.L.; Chuang, C.C.; Chiu, H.C.; Li, W.Y.; Horng, J.T.; Fu, E. Association between History of Dental Amalgam Fillings and Risk of Parkinson’s Disease: A Population-Based Retrospective Cohort Study in Taiwan. PLoS ONE 2016, 11, e0166552. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.C.; Sheu, J.J.; Lin, H.C.; Jensen, D.A. Increased risk of Parkinsonism following chronic periodontitis: A retrospective cohort study. Mov. Disord. 2013, 28, 1307–1308. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.S.; Lin, Y.C.; Hong, L.Y.; Chen, T.T.; Ma, H.P.; Hsu, Y.H.; Tsai, S.H.; Lin, Y.F.; Wu, M.Y. Increased Long-Term Risk of Dementia in Patients With Carbon Monoxide Poisoning: A Population-Based Study. Medicine 2016, 95, e2549. [Google Scholar] [CrossRef] [PubMed]
- Bohatschek, M.; Werner, A.; Raivich, G. Systemic LPS injection leads to granulocyte influx into normal and injured brain: Effects of ICAM-1 deficiency. Exp. Neurol. 2001, 172, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Noack, B.; Genco, R.J.; Trevisan, M.; Grossi, S.; Zambon, J.J.; De Nardin, E. Periodontal infections contribute to elevated systemic C-reactive protein level. J. Periodontol. 2001, 72, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Wu, Y.T.; Chang, Y.C. Association between chronic periodontitis and the risk of Alzheimer’s disease: A retrospective, population-based, matched-cohort study. Alzheimers Res. Ther. 2017, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.M.; Buchanan, S.A.; Hoover, C.I.; Newbrun, E.; Taggart, E.J.; Armitage, G.C.; Robertson, P.B. Clinical and microbiologic effects of single-dose metronidazole or scaling and root planing in treatment of adult periodontitis. J. Clin. Periodontol. 1986, 13, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, P.B.; Brennan, M.T.; Thornhill, M.; Michalowicz, B.S.; Noll, J.; Bahrani-Mougeot, F.K.; Sasser, H.C. Poor oral hygiene as a risk factor for infective endocarditis-related bacteremia. J. Am. Dent. Assoc. 2009, 140, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, A.R.; Singh, S.P.; Martande, S.S.; Raju, A.P.; Rustagi, T.; Suke, D.K.; Naik, S.B. Clinical evaluation of the periodontal health condition and oral health awareness in Parkinson’s disease patients. Gerodontology 2015, 32, 100–106. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Control Group without PD n = 19,060 | Case Group with PD n = 4765 | p-Value |
|---|---|---|---|
| Sex | 1.0000 | ||
| Female | 9624 (50.49%) | 2406 (50.49%) | |
| Male | 9436 (49.51%) | 2359 (49.51%) | |
| Age | 1.0000 | ||
| 40–69 | 5552 (29.13%) | 1388 (29.13%) | |
| ≥70 | 13,508 (70.87%) | 3377 (70.87%) | |
| Urbanization | <0.0001 | ||
| Level 1 | 10,369 (54.40%) | 2440 (51.21%) | |
| Level 2 | 5642 (29.60%) | 1256 (26.36%) | |
| Level 3 | 3049 (16.00%) | 1069 (22.43%) | |
| Comorbidities | |||
| Periodontal inflammatory disease | 8554 (44.88%) | 2322 (48.73%) | <0.0001 |
| Diabetes mellitus | 6925 (36.33%) | 2146 (45.04%) | <0.0001 |
| Hypertension | 13,151 (69.00%) | 3784 (79.41%) | <0.0001 |
| Hyperlipidemia | 9066 (47.57%) | 2601 (54.59%) | <0.0001 |
| Chronic kidney disease | 4996 (26.21%) | 1658 (34.80%) | <0.0001 |
| Depression | 646 (3.39%) | 447 (9.38%) | <0.0001 |
| Stroke | 3217 (16.88%) | 1669 (35.03%) | <0.0001 |
| Traumatic brain injury | 5678 (29.79%) | 2598 (54.52%) | <0.0001 |
| Dental scaling * | <0.0001 | ||
| No treatment | 9773 (51.27%) | 2282 (47.89%) | |
| Not 5 consecutive years | 8615 (45.2%) | 2336 (49.02%) | |
| For 5 consecutive years | 672 (3.53%) | 147 (3.08%) |
| Variables | Individuals | Multivariable Analysis | ||
|---|---|---|---|---|
| aOR | 95% CI | p-Value | ||
| Subgroup 1: 40–69 years old | ||||
| No treatment without PID | 2336 | Reference | - | - |
| Not 5 consecutive years without PID | 1001 | 0.943 | 0.770–1.155 | 0.5698 |
| For 5 consecutive years without PID | 35 | 0.204 | 0.047–0.886 | 0.0339 |
| No treatment with PID | 515 | 1.030 | 0.801–1.324 | 0.8159 |
| Not 5 consecutive years with PID | 2781 | 1.056 | 0.908–1.228 | 0.4763 |
| For 5 consecutive years with PID | 272 | 0.718 | 0.495–1.040 | 0.0796 |
| Subgroup 2: ≥70 years old | ||||
| No treatment without PID | 7645 | Reference | - | - |
| Not 5 consecutive years without PID | 1866 | 1.171 | 1.026–1.336 | 0.0192 |
| For 5 consecutive years without PID | 66 | 1.132 | 0.604–2.124 | 0.6986 |
| No treatment with PID | 1559 | 1.160 | 1.008–1.336 | 0.0387 |
| Not 5 consecutive years with PID | 5303 | 1.234 | 1.123–1.356 | <0.0001 |
| For 5 consecutive years with PID | 446 | 1.133 | 0.885–1.452 | 0.3217 |
| Annual Dental Scaling without PID | aOR | 95% CI | p-Value |
|---|---|---|---|
| Within 1 year before index date | 0.974 | 0.731–1.297 | 0.856 |
| 2 consecutive years before index date | 0.742 | 0.464–1.187 | 0.213 |
| 3 consecutive years before index date | 0.479 | 0.23–0.998 | 0.049 |
| 4 consecutive years before index date | 0.233 | 0.07–0.774 | 0.017 |
| 5 consecutive years before index date | 0.204 | 0.05–0.886 | 0.034 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-K.; Huang, J.-Y.; Wu, Y.-T.; Chang, Y.-C. Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study. Int. J. Environ. Res. Public Health 2018, 15, 1587. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081587
Chen C-K, Huang J-Y, Wu Y-T, Chang Y-C. Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study. International Journal of Environmental Research and Public Health. 2018; 15(8):1587. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081587
Chicago/Turabian StyleChen, Chang-Kai, Jing-Yang Huang, Yung-Tsan Wu, and Yu-Chao Chang. 2018. "Dental Scaling Decreases the Risk of Parkinson’s Disease: A Nationwide Population-Based Nested Case-Control Study" International Journal of Environmental Research and Public Health 15, no. 8: 1587. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081587