Ovarian Cancer Incidence in the U.S. and Toxic Emissions from Pulp and Paper Plants: A Geospatial Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data on Ovarian Cancer and Toxic Emissions
2.2. Exploratory Spatial Data Analysis Methods
2.3. Regression Analysis of the Relationship between Paper Mill Emissions and Ovarian Cancer
3. Results
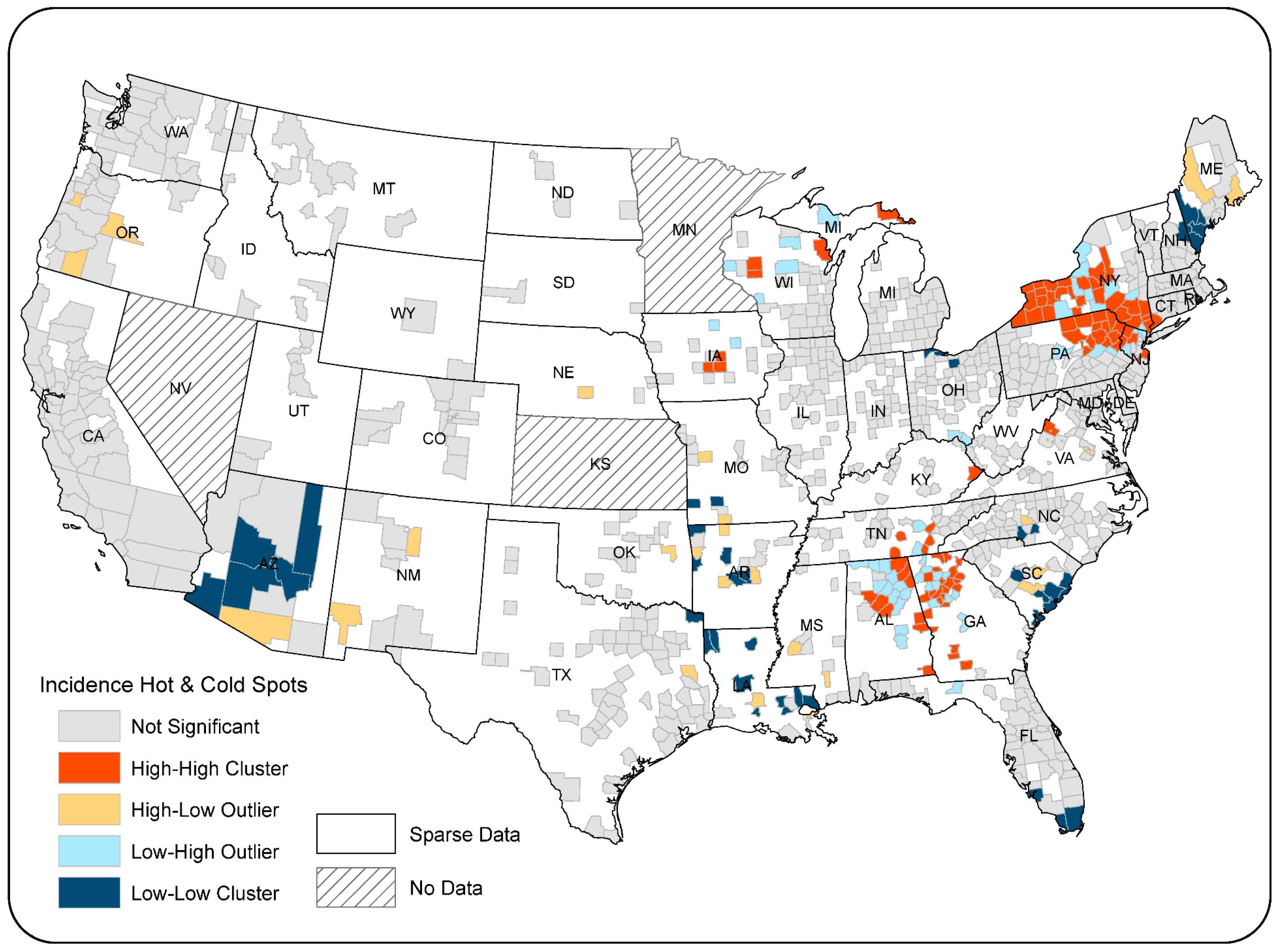
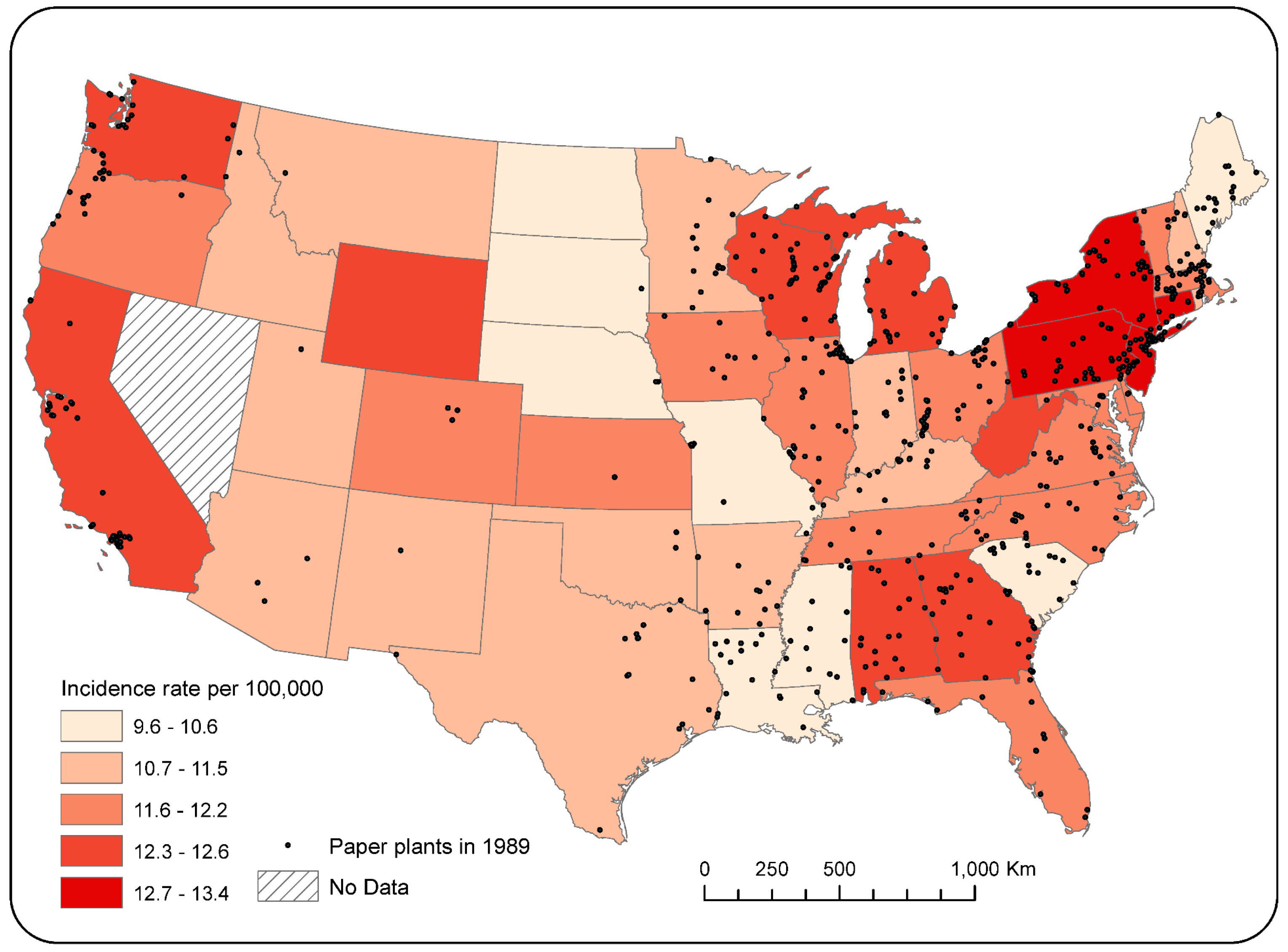
3.1. Spatial Distribution of Ovarian Incidence Rates
3.2. Spatial Patterns of Pulp and Paper Facilities
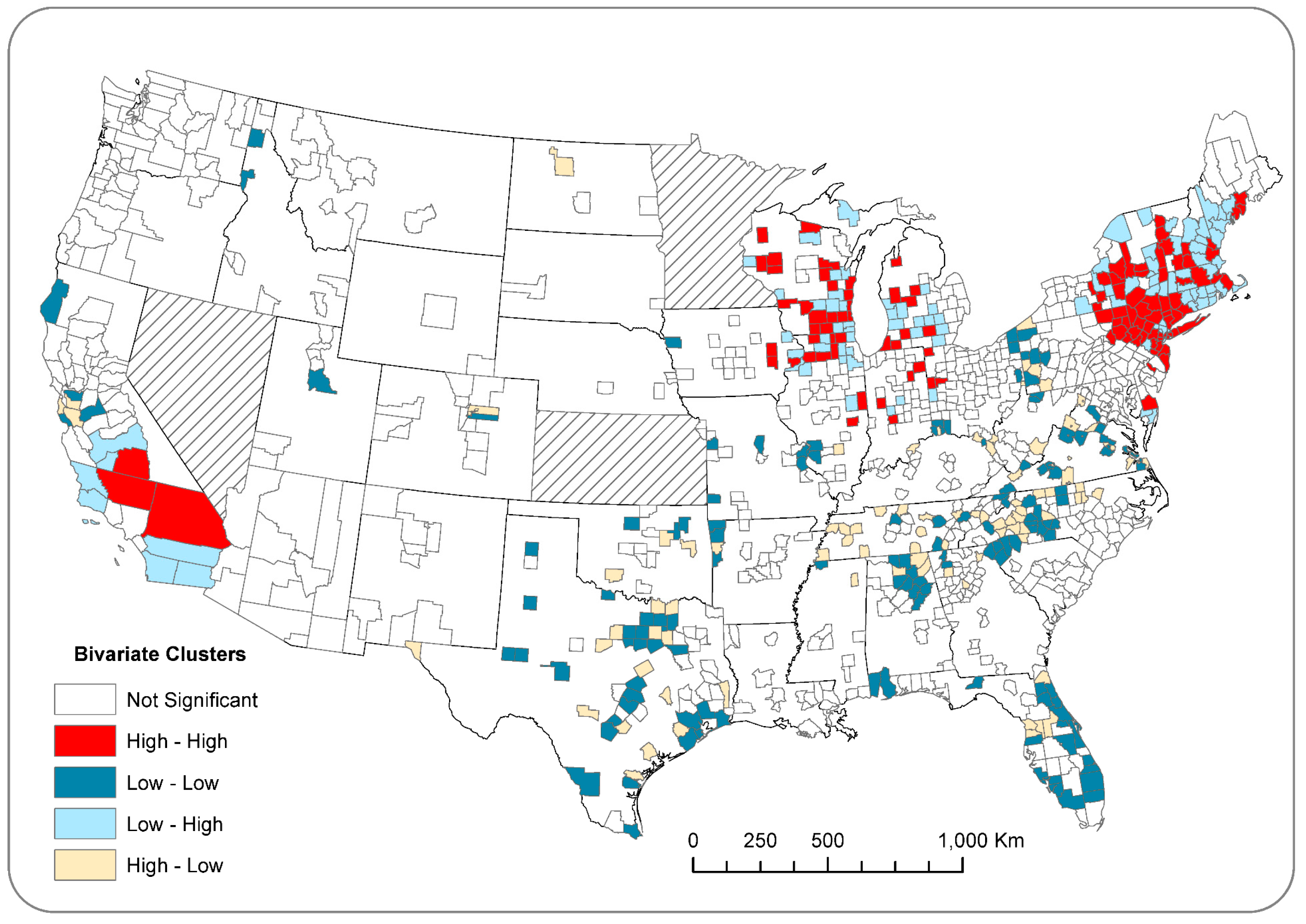
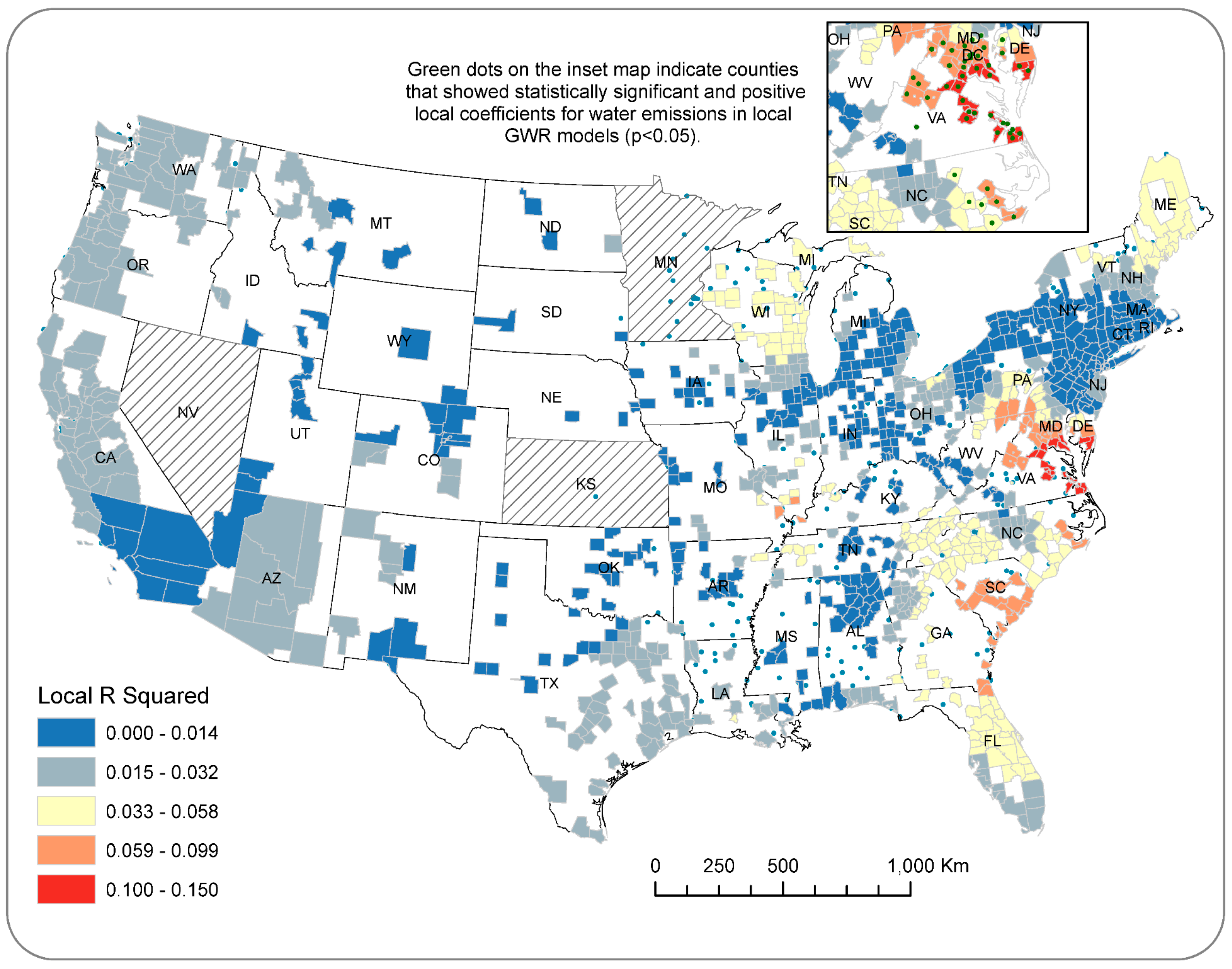
3.3. Impacts of Air and Water Emissions on Ovarian Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- American Cancer Society. Cancer Facts and Figures 2017; American Cancer Socity: Atlanta, GA, USA, 2017. [Google Scholar]
- Tokuoka, S.; Kawai, K.; Shimizu, Y.; Inai, K.; Ohe, K.; Fujikura, T.; Kato, H. Malignant and benign ovarian neoplasms among atomic bomb survivors, Hiroshima and Nagasaki, 1950-80. J. Natl. Cancer Inst. 1987, 79, 47–57. [Google Scholar] [PubMed]
- Hanna, L.; Adams, M. Prevention of ovarian cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2006, 20, 339–362. [Google Scholar] [CrossRef] [PubMed]
- Hunn, J.; Rodriguez, G.C. Ovarian cancer: Etiology, risk factors, and epidemiology. Clin. Obstet. Gynecol. 2012, 55, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Schildkraut, J.M.; Alberg, A.J.; Bandera, E.V.; Barnholtz-Sloan, J.; Bondy, M.; Cote, M.L.; Funkhouser, E.; Peters, E.; Schwartz, A.G.; Terry, P. A multi-center population-based case–control study of ovarian cancer in African-American women: The African American Cancer Epidemiology Study (AACES). BMC Cancer 2014, 14, 688. [Google Scholar] [CrossRef] [PubMed]
- Cramer, D.W.; Liberman, R.F.; Titus-Ernstoff, L.; Welch, W.R.; Greenberg, E.R.; Baron, J.A.; Harlow, B.L. Genital talc exposure and risk of ovarian cancer. Int. J. Cancer 1999, 81, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Gertig, D.M.; Hunter, D.J.; Cramer, D.W.; Colditz, G.A.; Speizer, F.E.; Willett, W.C.; Hankinson, S.E. Prospective study of talc use and ovarian cancer. J. Natl. Cancer Inst. 2000, 92, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Hanchette, C.L.; Schwartz, G.G. Geographic patterns of prostate cancer mortality. Evidence for a protective effect of ultraviolet radiation. Cancer 1992, 70, 2861–2869. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Hanchette, C.L. UV, latitude, and spatial trends in prostate cancer mortality: All sunlight is not the same (United States). Cancer Causes Control 2006, 17, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Boscoe, F.P.; Schymura, M.J. Solar ultraviolet-B exposure and cancer incidence and mortality in the United States, 1993–2002. BMC Cancer 2006, 6, 264. [Google Scholar] [CrossRef] [PubMed]
- Garland, C.F.; Mohr, S.B.; Gorham, E.D.; Grant, W.B.; Garland, F.C. Role of ultraviolet B irradiance and vitamin D in prevention of ovarian cancer. Am. J. Prev. Med. 2006, 31, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B. An estimate of premature cancer mortality in the US due to inadequate doses of solar ultraviolet-B radiation. Cancer 2002, 94, 1867–1875. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Garland, C.F. The association of solar ultraviolet B (UVB) with reducing risk of cancer: Multifactorial ecologic analysis of geographic variation in age-adjusted cancer mortality rates. Anticancer Res. 2006, 26, 2687–2699. [Google Scholar] [PubMed]
- Lefkowitz, E.S.; Garland, C.F. Sunlight, vitamin D, and ovarian cancer mortality rates in US women. Int. J. Epidemiol. 1994, 23, 1133–1136. [Google Scholar] [CrossRef] [PubMed]
- Cook, L.S.; Neilson, H.K.; Lorenzetti, D.L.; Lee, R.C. A systematic literature review of vitamin D and ovarian cancer. Am. J. Obstet. Gynecol. 2010, 203, 70.e1–70.e8. [Google Scholar] [CrossRef] [PubMed]
- Malvezzi, M.; Carioli, G.; Rodriguez, T.; Negri, E.; la Vecchia, C. Global trends and predictions in ovarian cancer mortality. Ann. Oncol. 2016, 27, 2017–2025. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M. Cancers of the breast, endometrium and ovary: Geographic correlations. Eur. J. Cancer Clin. Oncol. 1989, 25, 1917–1925. [Google Scholar] [CrossRef]
- Runnebaum, I.B.; Stickeler, E. Epidemiological and molecular aspects of ovarian cancer risk. J. Cancer Res. Clin. Oncol. 2001, 127, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Coburn, S.; Bray, F.; Sherman, M.; Trabert, B. International patterns and trends in ovarian cancer incidence, overall and by histologic subtype. Int. J. Cancer 2017, 140, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2014 Incidence and Mortality Web-Based Report; U.S. Department of Health and Human Services: Washington, DC, USA; Centers for Disease Control and Prevention: Atlanta, GA, USA; National Cancer Institute: Atlanta, GA, USA, 2017.
- García-Pérez, J.; Lope, V.; Lopez-Abente, G.; Gonzalez-Sanchez, M.; Fernandez-Navarro, P. Ovarian cancer mortality and industrial pollution. Environ. Pollut. 2015, 205, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Langseth, H.; Andersen, A. Cancer incidence among women in the Norwegian pulp and paper industry. Am. J. Ind. Med. 1999, 36, 108–113. [Google Scholar] [CrossRef]
- Soskolne, C.L.; Sieswerda, L.E. Cancer risk associated with pulp and paper mills: A review of occupational and community epidemiology. Chronic Dis. Can. 2010, 29, 86–100. [Google Scholar] [PubMed]
- Langseth, H.; Kjaerheim, K. Ovarian cancer and occupational exposure among pulp and paper employees in Norway. Scand. J. Work Environ. Health 2004, 30, 356–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camargo, M.C.; Stayner, L.T.; Straif, K.; Reina, M.; Al-Alem, U.; Demers, P.A.; Landrigan, P.J. Occupational exposure to asbestos and ovarian cancer: A meta-analysis. Environ. Health Perspect. 2011, 119, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Sahmoun, A.E. Ovarian cancer incidence in the United States in relation to manufacturing industry. Int. J. Gynecol. Cancer 2014, 24, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Parenteau, M.-P.; Sawada, M.C. The modifiable areal unit problem (MAUP) in the relationship between exposure to NO2 and respiratory health. Int. J. Health Geogr. 2011, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Rundquist, B.C.; Simon, I.J.; Swartz, S.E. Geographic distributions of motor neuron disease mortality and well water use in U.S. counties. Amyotroph. Lateral Scler. Frontotemporal Degener. 2017, 18, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.; Steel, D.; Tranmer, M. Area homogeneity and the modifiable areal unit problem. Geogr. Syst. 1996, 3, 181–200. [Google Scholar]
- Centers for Disease Control and Prevention; National Cancer Institute. State Cancer Profiles; Centers for Disease Control and Prevention: Atlanta, GA, USA; National Cancer Institute: Atlanta, GA, USA, 2017.
- Moorman, P.G.; Palmieri, R.T.; Akushevich, L.; Berchuck, A.; Schildkraut, J.M. Ovarian cancer risk factors in African-American and white women. Am. J. Epidemiol. 2009, 170, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Ness, R.B.; Grisso, J.A.; Klapper, J.; Vergona, R. Racial differences in ovarian cancer risk. J. Natl. Med. Assoc. 2000, 92, 176–182. [Google Scholar] [PubMed]
- U.S. Environmental Protection Agency. TRI Explorer; U.S. Environmental Protection Agency: Washington, DC, USA, 2017.
- Karoutsou, E.; Karoutsos, P.; Karoutsos, D. Endocrine Disruptors and Carcinogenesis. Arch. Cancer Res. 2017, 5, 1–8. [Google Scholar] [CrossRef]
- Anselin, L. Interactive techniques and exploratory spatial data analysis. In Geographical Information Systems: Principles, Techniques, Management and Applications; John Wiley & Son: Hoboken, NJ, USA, 1999; Volume 1, pp. 251–264. [Google Scholar]
- Kanaroglou, P.; Delmelle, E. Spatial Analysis in Health Geography; Routledge: Abingdon-on-Thames, UK, 2016. [Google Scholar]
- Sridharan, S.; Tunstall, H.; Lawder, R.; Mitchell, R. An exploratory spatial data analysis approach to understanding the relationship between deprivation and mortality in Scotland. Soc. Sci. Med. 2007, 65, 1942–1952. [Google Scholar] [CrossRef] [PubMed]
- Anselin, L. Spatial Regression. In The SAGE Handbook of Spatial Analysis; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2009; Volume 1, pp. 255–276. [Google Scholar]
- Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships; John Wiley & Son: Hoboken, NJ, USA, 2003. [Google Scholar]
- Kirby, R.S.; Delmelle, E.; Eberth, J.M. Advances in spatial epidemiology and geographic information systems. Ann. Epidemiol. 2017, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rezaeian, M.; Dunn, G.; Leger, S.S.; Appleby, L. Geographical epidemiology, spatial analysis and geographical information systems: A multidisciplinary glossary. J. Epidemiol. Community Health 2007, 61, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Brewer, C.A. Basic mapping principles for visualizing cancer data using Geographic Information Systems (GIS). Am. J. Prev. Med. 2006, 30, S253–S256. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, P. Where the Paper Industry went. Bangor Daily News, 14 December 2015. [Google Scholar]
- Choi, H.S.; Shim, Y.K.; Kaye, W.E.; Ryan, P.B. Potential residential exposure to toxics release inventory chemicals during pregnancy and childhood brain cancer. Environ. Health Perspect. 2006, 114, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, A.S.; Rahbar, M.H.; Han, I.; Bakian, A.V.; Bilder, D.A.; Harrington, R.A.; Pettygrove, S.; Durkin, M.; Kirby, R.S.; Wingate, M.S.; et al. Autism spectrum disorder prevalence and proximity to industrial facilities releasing arsenic, lead or mercury. Sci. Total Environ. 2015, 536, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, C.M. Improving the U.S. EPA Toxic Release Inventory database for environmental health research. J. Toxicol. Environ. Health B Crit. Rev. 1998, 1, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Rowntree, L.; Lewis, M.; Price, M.; Wyckoff, W. Diversity amid Globalization: World Regions, Environment, Development, 7th ed.; Pearson: San Francisco, CA, USA, 2017. [Google Scholar]
- U.S. Census Bureau; American Community Survey. Geographic Mobility in the Past Year by Age for Current Residence in the United States (B07001); 2011–2015 American Community Survey; U.S. Census Bureau: Suitland, MD, USA, 2017.
- Inoue-Choi, M.; Jones, R.R.; Anderson, K.E.; Cantor, K.P.; Cerhan, J.R.; Krasner, S.; Robien, K.; Weyer, P.J.; Ward, M.H. Nitrate and nitrite ingestion and risk of ovarian cancer among postmenopausal women in Iowa. Int. J. Cancer 2015, 137, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Tretli, S.; Vos, L.; Robsahm, T.E. Prediagnostic serum calcium and albumin and ovarian cancer: A nested case-control study in the Norwegian Janus Serum Bank Cohort. Cancer Epidemiol. 2017, 49, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Koutros, S.; Langseth, H.; Grimsrud, T.K.; Barr, D.B.; Vermeulen, R.; Portengen, L.; Wacholder, S.; Freeman, L.E.; Blair, A.; Hayes, R.B.; et al. Prediagnostic serum organochlorine concentrations and metastatic prostate cancer: A Nested Case-Control Study in the Norwegian Janus Serum Bank Cohort. Environ. Health Perspect. 2015, 123, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Laden, F.; Bertrand, K.A.; Altshul, L.; Aster, J.C.; Korrick, S.A.; Sagiv, S.K. Plasma organochlorine levels and risk of non-Hodgkin lymphoma in the Nurses' Health Study. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1381–1384. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | OLS Models | Spatial Lag Models | |||||
|---|---|---|---|---|---|---|---|
| Variables | All Emissions (n = 48) | Dioxin (n = 46) | OSHA Carcinogens (n = 46) | All Emissions (n = 48) | Dioxin (n = 46) | OSHA Carcinogens (n = 46) | |
| Intercept | 11.5283 | 11.6374 | 11.5851 | 5.96116 *** | 5.70606 *** | 5.53864 *** | |
| Air emissions | 0.00002 | −0.00119 | 0.00027 | −0.00002 | –0.00031 | 0.00009 | |
| Surface water | 0.00172 * | 0.00628 | 0.02813 | 0.00153 * | 0.00476 | 0.02793 | |
| Lagged incidence | n.a. | n.a. | n.a. | 0.47707 ** | 0.50422 *** | 0.51517 *** | |
| Adjusted R squared | 0.06982 | −0.02065 | 0.00485 | 0.28249 | 0.2348 | 0.2658 | |
| Akaike info criterion (AICc) | 122.754 | 123.37 | 122.206 | 117.442 | 117.638 | 115.926 | |
| Moran’s I diagnosis of residuals | 0.2515 ** | 0.2877 ** | 0.3044 *** | 0.01048 | 0.03608 | 0.04585 | |
| Models | OLS Models (n = 987) | GWR (n = 987) | |||||
|---|---|---|---|---|---|---|---|
| Variables | All Emissions | Dioxin | OSHA Carcinogens | All Emissions | Dioxin | OSHA Carcinogens | |
| Intercept | 12.6906 *** | 12.6549 *** | 12.6608 *** | 12.7146 *** | 12.7280 | 12.6967 | |
| Air emissions | −0.00204 * | −0.03467 * | −0.00715 | −0.00201 | −0.0387 | 0.000 | |
| Surface water | −0.00187 | 0.01119 | −0.1672 | −0.0413 | 0.0028 | 0.00002 | |
| Adjusted R squared | 0.00486 | 0.00216 | 0.00359 | 0.0466 | 0.0085 | 0.0412 | |
| Akaike info criterion (AICc) | 4856.083 | 4856.72 | 4855.31 | 4843.762 | 4854.897 | 4849.515 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanchette, C.; Zhang, C.H.; Schwartz, G.G. Ovarian Cancer Incidence in the U.S. and Toxic Emissions from Pulp and Paper Plants: A Geospatial Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081619
Hanchette C, Zhang CH, Schwartz GG. Ovarian Cancer Incidence in the U.S. and Toxic Emissions from Pulp and Paper Plants: A Geospatial Analysis. International Journal of Environmental Research and Public Health. 2018; 15(8):1619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081619
Chicago/Turabian StyleHanchette, Carol, Charlie H. Zhang, and Gary G. Schwartz. 2018. "Ovarian Cancer Incidence in the U.S. and Toxic Emissions from Pulp and Paper Plants: A Geospatial Analysis" International Journal of Environmental Research and Public Health 15, no. 8: 1619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081619