Association between Airborne Fine Particulate Matter and Residents’ Cardiovascular Diseases, Ischemic Heart Disease and Cerebral Vascular Disease Mortality in Areas with Lighter Air Pollution in China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.1.1. Data on Resident Mortality
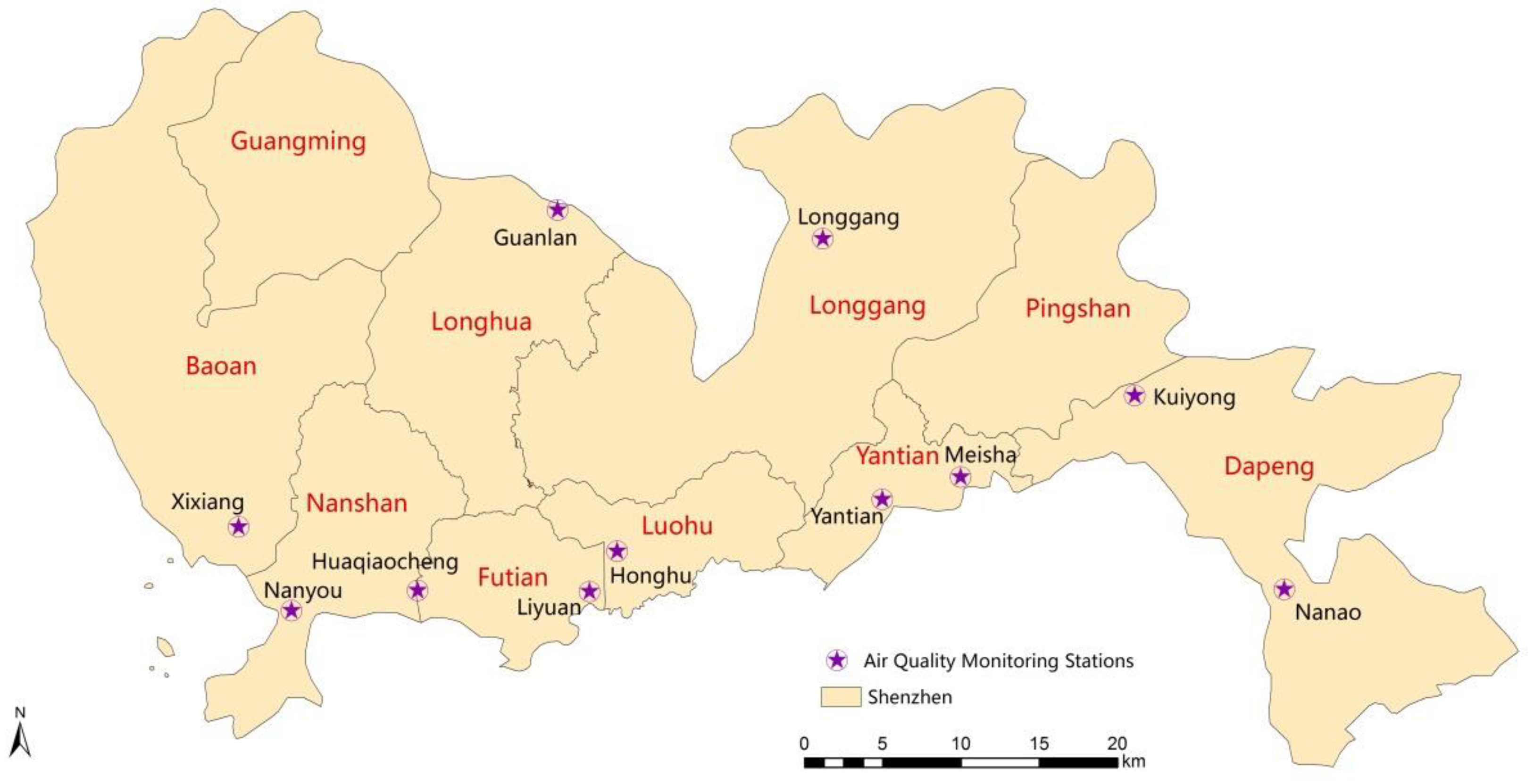
2.1.2. Air Quality Monitoring Data
2.1.3. Meteorological Data
2.2. Methods
2.2.1. Basic Description
2.2.2. Analysis of Time Series
2.2.3. Correlation Analysis
2.2.4. Generalized Additive Models (GAM)
as.factor(holiday) + s(temperature,df2) + s(humidity,df3) + α
3. Results
3.1. Basic Information of the Death of Residents from CVD
3.2. Information of Air Pollutants and Meteorological Factors
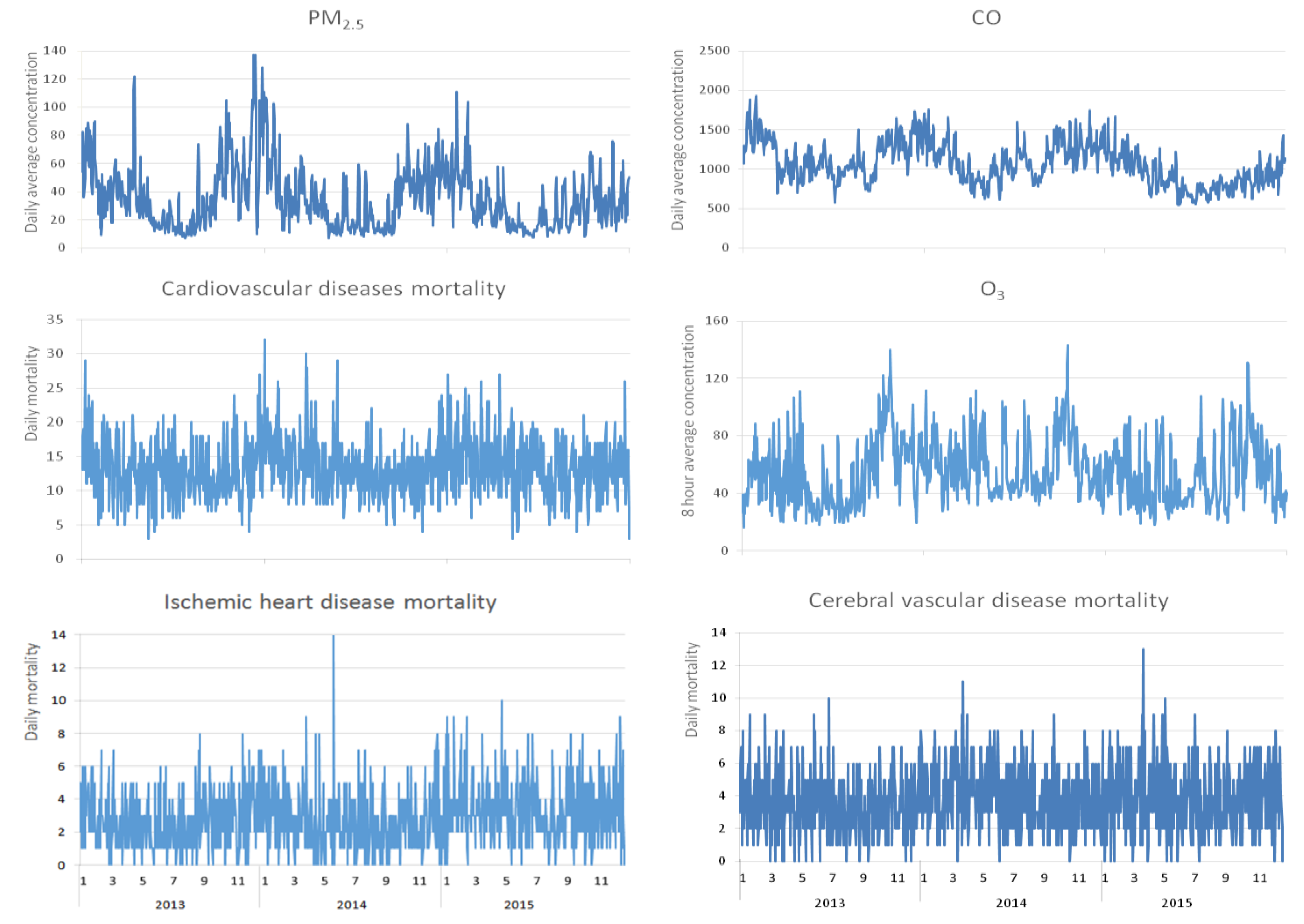
3.3. Time Series Chart on Resident Mortality from CVD versus Air Pollutant Concentration
3.4. Correlation Analysis of Air Pollutants versus Meteorological Factors
3.5. Autocorrelation between Different Lags for PM2.5
3.6. Analysis of GAM
3.6.1. Effects of PM2.5 Concentration upon CVD Mortality
3.6.2. Effects of PM2.5 Concentration upon IHD Mortality
3.6.3. Effects of PM2.5 Concentration upon EVD Mortality
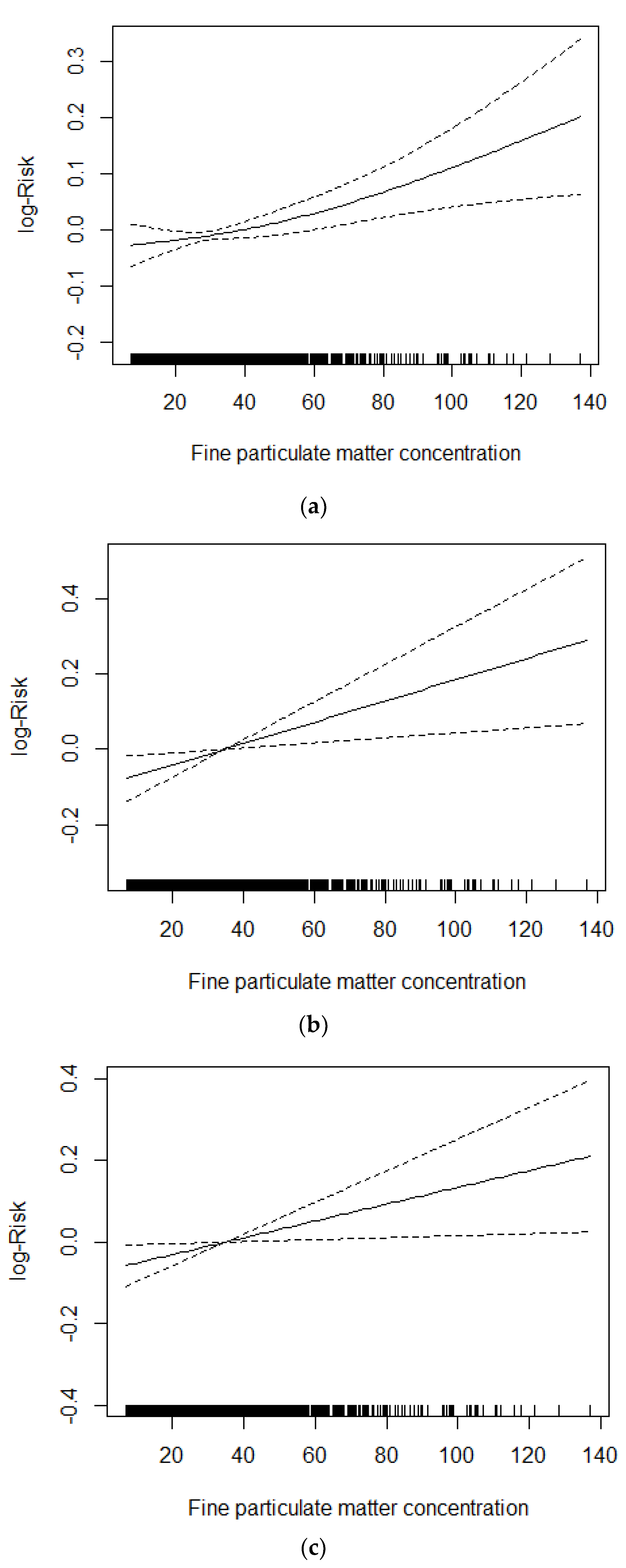
3.7. Concentration–Response Relationship
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Jiménez, E.; Linares, C.; Rodríguez, L.F.; Bleda, M.J.; Díaz, J. Short-term impact of particulate matter (PM2.5) on daily mortality among the over-75 age group in Madrid (Spain). Sci. Total Environ. 2009, 407, 5486–5492. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Mathes, R.; Ross, Z.; Nadas, A.; Thurston, G.; Matte, T. Fine particulate matter constituents associated with cardiovascular hospitalizations and mortality in New York City. Environ. Health Perspect. 2011, 119, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.; Feng, W.Y.; Broadwin, R.; Green, S.; Lipsett, M. The effects of components of fine particulate air pollution on mortality in California: Results from CALFINE. Environ. Health Perspect. 2007, 115, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ito, K.; Lall, R.; Lippmann, M.; Thurston, G. Time-series analysis of mortality effects of fine particulate matter components in Detroit and Seattle. Environ. Health Perspect. 2011, 119, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [PubMed]
- The Report of the 19th Session of National Congress of the Communist Party of China, China, 18 October to 24 October 2017. Available online: http://www.lsctgz.com/article/djzl/dzz/201710/1746.html (accessed on 21 July 2018).
- Ministry of Ecology and Environment of the People’s Republic of China. Chinese Environmental Status Bulletin. Available online: http://www.zhb.gov.cn/hjzl/zghjzkgb/lnzghjzkgb/ (accessed on 21 July 2018).
- National Air Quality Real-time Ranking. Available online: http://www.86pm25.com/paiming.htm (accessed on 21 July 2018).
- Chen, R.J.; Yin, P.; Meng, X.; Liu, C.; Wang, L.J.; Xu, X.H.; Ross, J.A.; Tse, L.A.; Zhao, Z.H.; Kan, H.D.; et al. Fine Particulate Air Pollution and Daily Mortality. A Nationwide Analysis in 272 Chinese Cities. Am. J. Respir. Crit. Care Med. 2017, 196, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Peng, R.D.; Dominici, F.; Samet, J.M. Emergency hospital admissions for cardiovascular diseases and ambient levels of carbon monoxide: Results for 126 United States urban counties, 1999–2005. Circulation 2009, 120, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Speakman, J.R. Impact of Obesity and Ozone on the Association between Particulate Air Pollution and Cardiovascular Disease and Stroke Mortality among US Adults. J. Am. Heart Assoc. 2018, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.; Tibshirani, R. Generalized additive models for medical research. Stat. Methods Med. Res. 1995, 4, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Laden, F.; Zanobetti, A. The Concentration-Response Relation between PM2.5 and Daily Deaths. Environ. Health Perspect. 2002, 110, 1025–1029. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J. Air pollution and daily mortality: A review and meta-analysis. Environ. Res. 1994, 64, 36–52. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Schwartz, J.; Groot, B.; Eilers, P. Effects of ambient particulate matter and ozone on daily mortality in Rotterdam, The Netherlands. Arch. Environ. Health 1997, 52, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Michelozzi, P.; Forastiere, F.; Fusco, D.; Perucci, C.A.; Ostro, B.; Ancona, C.; Pallotti, G. Air pollution and daily mortality in Rome, Italy. Occup. Environ. Med. 1998, 55, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsouyanni, K.; Touloumi, G.; Samoli, E.; Gryparis, A.L.; Tertre, A.; Monopolis, Y.; Rossi, G.; Zmirou, D.; Ballester, F.; Boumghar, A.; et al. Confounding and effect modification in the short-term effects of ambient particles on total mortality: Results from 29 European Cities within the APHEA2 Project. Epidemiology 2001, 12, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Ver Hoef, J.M.; Boveng, P.L. Quasi-Poisson vs.negative binomial regression: How should we model overdispersed count data? Ecology 2007, 88, 2766–2772. [Google Scholar] [CrossRef] [PubMed]
- Kloog, I.; Ridgway, B.; Koutrakis, P.; Coull, B.A.; Schwartz, J.D. Long-and short-term exposure to PM2.5 and mortality: Using novel exposure models. Epidemiology 2013, 24, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Yu, I.T.; Tian, L.; Wang, X.; Tse, L.A.; Tam, W.; Wong, T.W. Effects of Coarse Particulate Matter on Emergency Hospital Admissions for Respiratory Diseases: A Time-Series Analysis in Hong Kong. Environ. Health Perspect. 2012, 120, 572–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, T.W.; Tam, W.; Tak Sun Yu, I.; Wun, Y.T.; Wong, A.H.; Wong, C.M. Association between air pollution and general practitioner visits for respiratory diseases in Hong Kong. Thorax 2006, 61, 585–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, S.N. Generalized Additive Models: An Introduction with R; CRC Press: Boca Raton, FL, USA, 2006; Available online: https://www.crcpress.com/Generalized-Additive-Models-An-Introduction-with-R/Wood/9781584884743 (accessed on 5 August 2015).
- Dai, L.Z.; Zanobetti, A.; Koutrakis, P.; Schwartz, J.D. Associations of Fine Particulate Matter Species with Mortality in the United States: A Multicity Time-Series Analysis. Environ. Health Perspect. 2014, 122, 837–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kan, H.D.; London, S.J.; Chen, G.H.; Zhang, Y.H.; Song, G.X.; Zhao, N.Q.; Jiang, L.L.; Chen, B. Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China. Environ. Int. 2007, 33, 376–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, L.H.; Zanobetti, A.; Kloog, I.; Coull, B.A.; Koutrakis, P.; Melly, S.J.; Schwartz, J.D. Low-Concentration PM2.5 and Mortality: Estimating Acute and Chronic Effects in a Population-Based Study. Environ. Health Perspect. 2016, 124, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Badaloni, C.; Gariazzo, C.; Stafoggia, M.; Sozzi, R.; Davoli, M.; Forastiere, F. Long-Term Exposure to Urban Air Pollution and Mortality in a Cohort of More than a Million Adults in Rome. Environ. Health Perspect. 2013, 121, 324–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thurston, G.D.; Burnett, R.T.; Turner, M.C.; Shi, Y.; Krewski, D.; Lall, R.; Ito, K.; Jerrett, M.; Gapstur, S.M.; Diver, W.R.; et al. Ischemic Heart Disease Mortality and Long-Term Exposure to Source-Related Components of U.S. Fine Particle Air Pollution. Environ. Health Perspect. 2016, 124, 785–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cifuentes, L.A.; Vega, J.; Köpfer, K.; Lave, L.B. Effect of the Fine Fraction of Particulate Matter versus the Coarse Mass and Other Pollutants on Daily Mortality in Santiago, Chile. J. Air Waste Manag. Assoc. 2000, 50, 1287–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krall, J.R.; Anderson, G.B.; Dominici, F.; Bell, M.L.; Peng, R.D. Short-term Exposure to Particulate Matter Constituents and Mortality in a National Study of U.S. Urban Communities. Environ. Health Perspect. 2013, 121, 1148–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.L.; Samet, J.M.; Dominici, F. Time-series studies of particulate matter. Annu. Rev. Public Health 2004, 25, 247–280. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S. A new model for investigating the mortality effects of multiple air pollutants in air pollution mortality time-series studies. J. Toxicol. Environ. Health A 2006, 69, 417–435. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.H.; Huang, W.; London, S.J.; Song, G.X.; Chen, G.H.; Jiang, L.L.; Zhao, N.Q.; Chen, B.H.; Kan, H.D. Ozone and daily mortality in Shanghai, China. Environ. Health Perspect. 2006, 114, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.A.; Fischer, P.; Marra, M.; Ameling, C.; Cassee, F.R. Short-term effects of PM2.5, PM10 and PM2.5–10 on daily mortality in the Netherlands. Sci. Total Environ. 2013, 463–464, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Environmental Protection of the People’s Republic of China. Ambient Air Quality Standards. GB3095-2012. Available online: http://kjs.mep.gov.cn/hjbhbz/bzwb/dqhjbh/dqhjzlbz/201203/t20120302_224165.htm (accessed on 6 February 2018).
- Brook, R.D.; Franklin, B.; Cascio, W.; Hong, Y.; Howard, G.; Lipsett, M.; Luepker, R.; Mittleman, M.; Samet, J.; Smith, S.C., Jr.; et al. Air Pollution and Cardiovascular Disease: A Statement for Healthcare Professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 2004, 109, 2655–2671. [Google Scholar] [CrossRef] [PubMed]
- Maté, T.; Guaita, R.; Pichiule, M.; Linares, C.; Díaz, J. Short-term effect of fine particulate matter (PM2.5) on daily mortality due to diseases of the circulatory system in Madrid (Spain). Sci. Total Environ. 2010, 408, 5750–5757. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Stafoggia, M.; Raaschou-Nielsen, O.; Andersen, Z.J.; Xun, W.W.; Katsouyanni, K.; Dimakopoulou, K.; Brunekreef, B.; Weinmayr, G.; Hoffmann, B.; et al. Long-term exposure to air pollution and cardiovascular mortality: An analysis of 22 European cohorts. Epidemiology 2014, 25, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Burnett, R.T.; Copes, R.; Kwong, J.C.; Villeneuve, P.J.; Goldberg, M.S.; Brook, R.D.; van Donkelaar, A.; Jerrett, M.; Martin, R.V.; et al. Ambient Fine Particulate Matter and Mortality among Survivors of Myocardial Infarction: Population-Based Cohort Study. Environ. Health Perspect. 2016, 124, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Pinault, L.; Tjepkema, M.; Crouse, D.L.; Weichenthal, S.; van Donkelaar, A.; Martin, R.V.; Brauer, M.; Chen, H.; Burnett, R.T. Risk estimates of mortality attributed to low concentrations of ambient fine particulate matter in the Canadian community health survey cohort. Environ. Health 2016, 11, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.M.; Lai, H.K.; Tsang, H.; Thach, T.Q.; Thomas, G.N.; Lam, K.B.; Chan, K.; Yang, L.; Lau, A.K.; Ayres, J.G.; et al. Satellite-Based Estimates of Long-Term Exposure to Fine Particles and Association with Mortality in Elderly Hong Kong Residents. Environ. Health Perspect. 2015, 123, 1167–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanobetti, A.; Schwartz, J. The effect of fine and coarse particulate air pollution on mortality: A national analysis. Environ. Health Perspect. 2009, 117, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; Burnett, R.T.; Ma, R.; Pope, C.A., 3rd; Krewski, D.; Newbold, K.B.; Thurston, G.; Shi, Y.; Finkelstein, N.; Calle, E.E.; et al. Spatial analysis of air pollution and mortality in Los Angeles. Epidemiology 2005, 16, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Li, G.; Zhao, D.; Xie, X.; Wei, Z.; Wang, W.; Wang, M.; Li, G.; Liu, W.; Sun, J.; et al. Relationship between fine particulate air pollution and ischaemic heart disease morbidity and mortality. Heart 2015, 101, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Eliot, M.N.; Wellenius, G.A. Short-term Changes in Ambient Particulate Matter and Risk of Stroke: A Systematic Review and Meta-analysis. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics of the People’s Republic of China. TABULATION ON THE 2010 POPULATION CENSUS OF THE PEOPLES REPUBLIC OF CHINA. Available online: http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm (accessed on 6 February 2018).
- SHENZHEN CHINA. Shenzhen Statistics. SHENZHEN STAISTICAL YEARBOOK. Available online: http://www.sztj.gov.cn/xxgk/tjsj/tjnj/201606/W020160607351981905550.pdf (accessed on 6 February 2018).
- National Bureau of Statistics of the People’s Republic of China. CHINA STAISTICAL YEARBOOK. Available online: http://www.stats.gov.cn/tjsj/tjcbw/201512/t20151210_1287840.html (accessed on 6 February 2018).




{kind=link}
{kind=link}
{kind=link}
| Category | Total Deaths | Percent Among Total Deaths (%) | Daily Average Number of Deaths | Standard Deviation | Lowest Daily Deaths | Q1 | Q2 | Q3 | Highest Daily Deaths |
|---|---|---|---|---|---|---|---|---|---|
| Total death | 41,815 | 100.0 | 38.2 | 7.6 | 10 | 33 | 38 | 43 | 77 |
| CVD death | 14,537 | 34.8 | 13.3 | 4.1 | 3 | 11 | 13 | 16 | 32 |
| IHD death | 3188 | 7.6 | 2.9 | 1.8 | 0 | 2 | 3 | 4 | 14 |
| EVD death | 4028 | 9.6 | 3.7 | 2.0 | 0 | 2 | 4 | 5 | 13 |
| Indicator | Mean | Standard Deviation | Minimum | Q1 | Q2 | Q3 | Maximum | No. of Days of Exceeding Grade 1 Criterion * | No. of Days of Exceeding Grade 2 Criterion ** |
|---|---|---|---|---|---|---|---|---|---|
| Air pollutants | |||||||||
| PM2.5 (μg/m3) | 35.0 | 21.9 | 7.1 | 17.4 | 29.9 | 47.1 | 137.1 | 458 | 58 |
| PM10 (μg/m3) | 55.6 | 30.2 | 10.9 | 31.4 | 47.7 | 71.6 | 181.8 | 513 | 11 |
| SO2 (μg/m3) | 10.4 | 4.8 | 3.5 | 7.4 | 9.2 | 11.9 | 54.8 | 1 | 0 |
| NO2 (μg/m3) | 43.8 | 17.5 | 14.7 | 31.9 | 39.7 | 51.6 | 133.7 | 47 | 47 |
| CO (μg/m3) | 1061.9 | 259.7 | 542.9 | 857.1 | 1034.1 | 1239.1 | 1930.4 | 0 | 0 |
| O3 (μg/m3) | 55.2 | 22.3 | 16.4 | 37.6 | 50.8 | 70.0 | 143.3 | 42 | 0 |
| Meteorological factors | |||||||||
| Daily average temperature (°C) | 23. 5 | 5.5 | 6.0 | 19.2 | 24.8 | 28.2 | 33.0 | ||
| Daily average RH (%) | 73.3 | 13.3 | 19.0 | 67.0 | 75.0 | 82.0 | 100.0 | ||
| Daily average atmosphere pressure (kpa) | 1005.6 | 6.4 | 986.8 | 1000.7 | 1005.5 | 1010.8 | 1019.9 | ||
| Daily average wind speed (m/s) | 2.1 | 0.8 | 0.3 | 1.5 | 2.0 | 2.5 | 5.5 |
| Items | PM10 | SO2 | NO2 | CO | O3 | Daily Average Temperature | Daily Average RH | Daily Average Atmosphere Pressure | Daily Average Wind Speed |
|---|---|---|---|---|---|---|---|---|---|
| PM2.5 | 0.956 | 0.622 | 0.628 | 0.447 | 0.567 | −0.556 | −0.515 | 0.595 | −0.111 |
| PM10 | 0.680 | 0.628 | 0.399 | 0.601 | −0.447 | −0.591 | 0.529 | −0.127 | |
| SO2 | 0.612 | 0.257 | 0.318 | −0.176 | −0.515 | 0.270 | −0.143 | ||
| NO2 | 0.343 | 0.063 * | −0.415 | −0.118 | 0.346 | −0.400 | |||
| CO | 0.189 | −0.315 | −0.075* | 0.242 | 0.037n | ||||
| O3 | −0.117n | −0.572 | 0.240 | 0.078 * | |||||
| Daily average temperature (°C) | 0.200 | −0.858 | −0.093 | ||||||
| Daily average RH (%) | −0.451 | −0.046n | |||||||
| Daily average atmosphere pressure (kpa) | 0.047n | ||||||||
| Items | lag1 | lag2 | lag3 | lag4 | lag5 |
|---|---|---|---|---|---|
| lag0 | 0.825 | 0.692 | 0.631 | 0.582 | 0.531 |
| lag1 | 0.825 | 0.692 | 0.631 | 0.583 | |
| lag2 | 0.824 | 0.691 | 0.631 | ||
| lag3 | 0.825 | 0.691 | |||
| lag4 | 0.824 |
| Items | Single Pollutant Model (Without Controlling Other Pollutants) | 2-Pollutant Model (Controlling CO) | 2-Pollutant Model (Controlling O3) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | StdErr | P | ER% (95% CI) | β | StdErr | P | ER% (95% CI) | β | StdErr | P | ER (95% CI) | |
| Cardiovascular disease mortality | ||||||||||||
| lag0 | 0.0016 | 0.0006 | 0.005 # | 1.60 (0.48–2.73) | 0.0018 | 0.0006 | 0.005 # | 1.83 (0.54–3.13) | 0.0016 | 0.0006 | 0.007 # | 1.63 (0.45–2.82) |
| lag1 | 0.0014 | 0.0005 | 0.010 * | 1.40 (0.33–2.49) | 0.0016 | 0.0006 | 0.006 # | 1.65 (0.46–2.86) | 0.0016 | 0.0006 | 0.008 # | 1.58 (0.41–2.76) |
| lag2 | 0.0014 | 0.0005 | 0.010 * | 1.37 (0.33–2.42) | 0.0016 | 0.0006 | 0.005 # | 1.65 (0.51–2.82) | 0.0015 | 0.0006 | 0.009 # | 1.55 (0.39–2.73) |
| lag3 | 0.0010 | 0.0005 | 0.053 @ | 1.00 (−0.01–2.02) | 0.0011 | 0.0006 | 0.042 * | 1.15 (0.04–2.28) | 0.0010 | 0.0006 | 0.074 @ | 1.04 (−0.1–2.2) |
| lag4 | 0.0009 | 0.0005 | 0.081 @ | 0.89 (−0.11–1.90) | 0.0012 | 0.0006 | 0.034 * | 1.19 (0.09–2.31) | 0.0012 | 0.0006 | 0.031 * | 1.25 (0.12–2.4) |
| lag5 | 0.0015 | 0.0005 | 0.003 # | 1.50 (0.51–2.50) | 0.0016 | 0.0006 | 0.004 # | 1.61 (0.52–2.72) | 0.0023 | 0.0006 | 0.000 # | 2.28 (1.15–3.42) |
| lag01 | 0.0018 | 0.0006 | 0.003 # | 1.85 (0.63–3.09) | 0.0021 | 0.0007 | 0.002 # | 2.1 (0.75–3.48) | 0.0020 | 0.0007 | 0.003 # | 2.04 (0.7–3.39) |
| lag02 | 0.0021 | 0.0007 | 0.002 # | 2.09 (0.79–3.41) | 0.0023 | 0.0007 | 0.001 # | 2.37 (0.96–3.81) | 0.0024 | 0.0007 | 0.001 # | 2.45 (0.98–3.93) |
| lag03 | 0.0021 | 0.0007 | 0.002 # | 2.14 (0.79–3.51) | 0.0024 | 0.0007 | 0.001 # | 2.39 (0.93–3.86) | 0.0025 | 0.0008 | 0.001 # | 2.56 (1–4.14) |
| lag04 | 0.0021 | 0.0007 | 0.002 # | 2.17 (0.78–3.59) | 0.0024 | 0.0008 | 0.001 # | 2.43 (0.93–3.95) | 0.0027 | 0.0008 | 0.001 # | 2.77 (1.14–4.43) |
| Ischemic heart disease mortality | ||||||||||||
| lag0 | 0.0021 | 0.0012 | 0.072 @ | 2.12 (−0.18–4.47) | 0.0032 | 0.0014 | 0.018 * | 3.26 (0.56–6.03) | 0.0026 | 0.0012 | 0.035 * | 2.62 (0.19–5.11) |
| lag1 | 0.0029 | 0.0011 | 0.010 * | 2.92 (0.69–5.20) | 0.0042 | 0.0013 | 0.001 # | 4.3 (1.76–6.91) | 0.0033 | 0.0012 | 0.006 # | 3.36 (0.93–5.85) |
| lag2 | 0.0028 | 0.0011 | 0.009 # | 2.87 (0.71–5.07) | 0.0043 | 0.0012 | 0.000 # | 4.38 (1.93–6.88) | 0.0031 | 0.0012 | 0.010 * | 3.14 (0.74–5.61) |
| lag3 | 0.0011 | 0.0011 | 0.289 | 1.12 (−0.94–3.24) | 0.0020 | 0.0012 | 0.091 @ | 2.01 (−0.32–4.39) | 0.0008 | 0.0012 | 0.487 | 0.84 (−1.5–3.23) |
| lag4 | 0.0014 | 0.0010 | 0.179 | 1.41 (−0.64–3.50) | 0.0020 | 0.0012 | 0.089 @ | 2 (−0.3–4.35) | 0.0019 | 0.0012 | 0.104 | 1.94 (−0.4–4.34) |
| lag5 | 0.0023 | 0.0010 | 0.023 * | 2.37 (0.33–4.46) | 0.0026 | 0.0012 | 0.022 * | 2.68 (0.39–5.03) | 0.0033 | 0.0012 | 0.005 # | 3.33 (0.98–5.73) |
| lag01 | 0.0031 | 0.0013 | 0.014 * | 3.15 (0.63–5.75) | 0.0044 | 0.0014 | 0.002 # | 4.55 (1.67–7.5) | 0.0038 | 0.0014 | 0.006 # | 3.85 (1.1–6.68) |
| lag02 | 0.0038 | 0.0013 | 0.005 # | 3.86 (1.17–6.63) | 0.0053 | 0.0015 | 0.000 # | 5.39 (2.38–8.49) | 0.0046 | 0.0015 | 0.002 # | 4.71 (1.68–7.83) |
| lag03 | 0.0035 | 0.0014 | 0.011 * | 3.60 (0.82–6.45) | 0.0050 | 0.0015 | 0.001 # | 5.08 (2.01–8.25) | 0.0042 | 0.0016 | 0.008 # | 4.34 (1.14–7.64) |
| lag04 | 0.0035 | 0.0014 | 0.014 * | 3.58 (0.73–6.51) | 0.0049 | 0.0016 | 0.002 # | 4.98 (1.84–8.22) | 0.0045 | 0.0017 | 0.007 # | 4.55 (1.21–8.01) |
| Cerebral vascular disease mortality | ||||||||||||
| lag0 | 0.0020 | 0.0010 | 0.045 * | 2.03 (0.04–4.06) | 0.0021 | 0.0011 | 0.062 @ | 2.16 (−0.1–4.47) | 0.0017 | 0.0011 | 0.121 | 1.67 (−0.44–3.81) |
| lag1 | 0.0020 | 0.0010 | 0.034 * | 2.07 (0.16–4.02) | 0.0019 | 0.0011 | 0.068 @ | 1.95 (−0.14–4.1) | 0.0018 | 0.0011 | 0.092 @ | 1.81 (−0.29–3.96) |
| lag2 | 0.0015 | 0.0009 | 0.126 | 1.46 (−0.40–3.36) | 0.0013 | 0.0010 | 0.199 | 1.34 (−0.7–3.42) | 0.0017 | 0.0011 | 0.108 | 1.74 (−0.38–3.91) |
| lag3 | 0.0019 | 0.0009 | 0.040 * | 1.90 (0.08–3.75) | 0.0018 | 0.0010 | 0.080 @ | 1.78 (−0.21–3.81) | 0.0021 | 0.0011 | 0.049 * | 2.09 (0–4.23) |
| lag4 | 0.0021 | 0.0009 | 0.023 * | 2.09 (0.28–3.92) | 0.0025 | 0.0010 | 0.014 * | 2.49 (0.5–4.51) | 0.0018 | 0.0011 | 0.085 @ | 1.83 (−0.25–3.95) |
| lag5 | 0.0020 | 0.0009 | 0.029 * | 1.99 (0.20–3.81) | 0.0020 | 0.0010 | 0.043 * | 2.03 (0.07–4.04) | 0.0018 | 0.0010 | 0.083 @ | 1.83 (−0.23–3.94) |
| lag01 | 0.0024 | 0.0011 | 0.024 * | 2.46 (0.32–4.64) | 0.0024 | 0.0012 | 0.043 * | 2.43 (0.07–4.84) | 0.0020 | 0.0012 | 0.085 @ | 2.06 (−0.28–4.47) |
| lag02 | 0.0025 | 0.0011 | 0.028 * | 2.52 (0.27–4.82) | 0.0024 | 0.0012 | 0.051 @ | 2.43 (−0.01–4.93) | 0.0024 | 0.0013 | 0.064 @ | 2.43 (−0.14–5.06) |
| lag03 | 0.0027 | 0.0012 | 0.019 * | 2.78 (0.45–5.16) | 0.0026 | 0.0013 | 0.039 * | 2.63 (0.13–5.19) | 0.0028 | 0.0014 | 0.043 * | 2.82 (0.09–5.62) |
| lag04 | 0.0030 | 0.0012 | 0.012 * | 3.08 (0.68–5.53) | 0.0029 | 0.0013 | 0.022 * | 2.99 (0.43–5.61) | 0.0029 | 0.0014 | 0.041 * | 2.97 (0.12–5.91) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, J.; Yu, S.; Pei, Y.; Peng, C.; Liao, Y.; Liu, N.; Ji, J.; Cheng, J. Association between Airborne Fine Particulate Matter and Residents’ Cardiovascular Diseases, Ischemic Heart Disease and Cerebral Vascular Disease Mortality in Areas with Lighter Air Pollution in China. Int. J. Environ. Res. Public Health 2018, 15, 1918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091918
Cai J, Yu S, Pei Y, Peng C, Liao Y, Liu N, Ji J, Cheng J. Association between Airborne Fine Particulate Matter and Residents’ Cardiovascular Diseases, Ischemic Heart Disease and Cerebral Vascular Disease Mortality in Areas with Lighter Air Pollution in China. International Journal of Environmental Research and Public Health. 2018; 15(9):1918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091918
Chicago/Turabian StyleCai, Junfang, Shuyuan Yu, Yingxin Pei, Chaoqiong Peng, Yuxue Liao, Ning Liu, Jiajia Ji, and Jinquan Cheng. 2018. "Association between Airborne Fine Particulate Matter and Residents’ Cardiovascular Diseases, Ischemic Heart Disease and Cerebral Vascular Disease Mortality in Areas with Lighter Air Pollution in China" International Journal of Environmental Research and Public Health 15, no. 9: 1918. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091918