Mind-Body Exercise (Wuqinxi) for Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Inclusion Criteria and Study Selection
2.3. Assessment of Study Quality
2.4. Data Extraction and Synthesis
3. Results
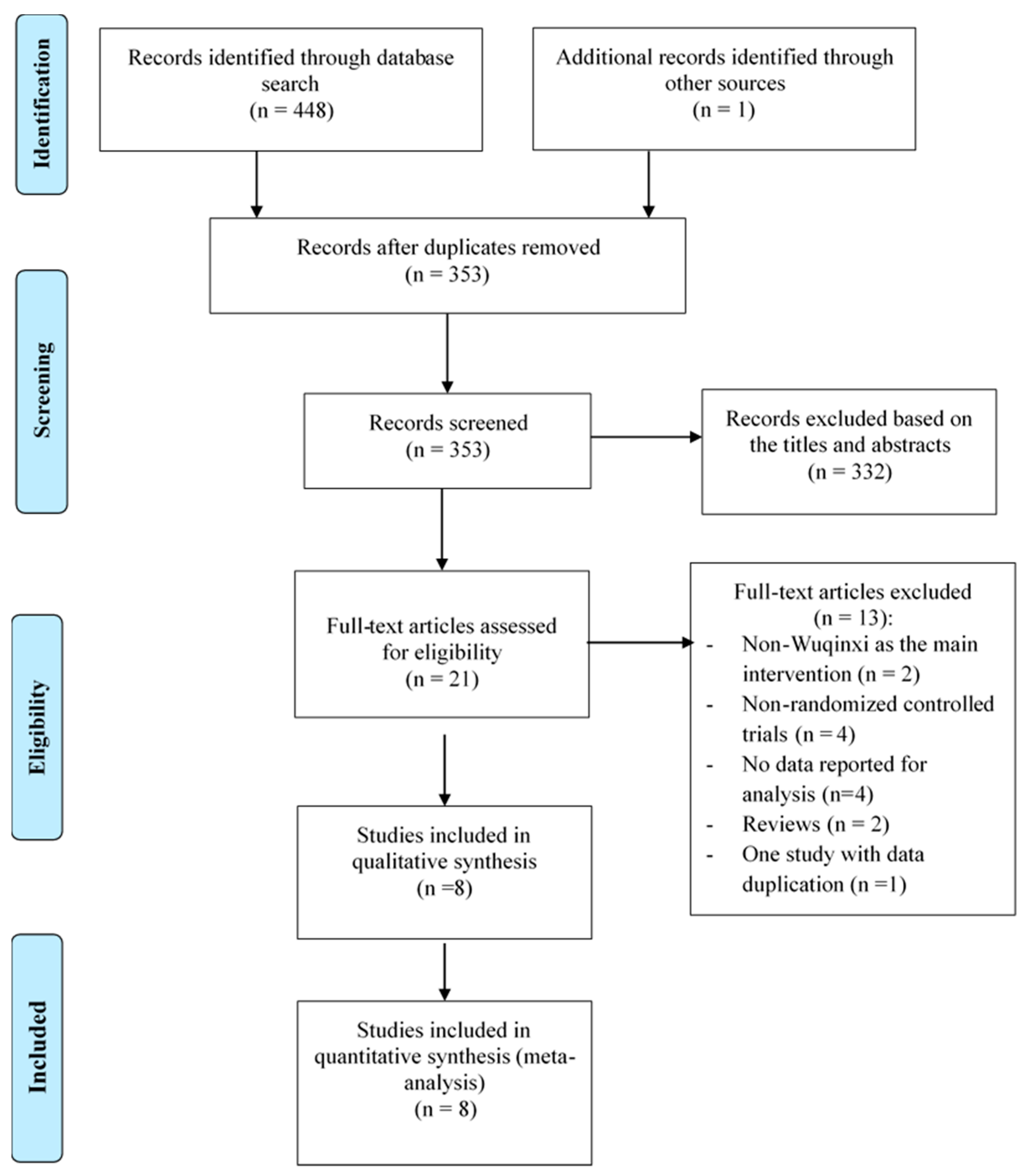
3.1. Study Selection
3.2. Study Characteristics and Methodological Quality
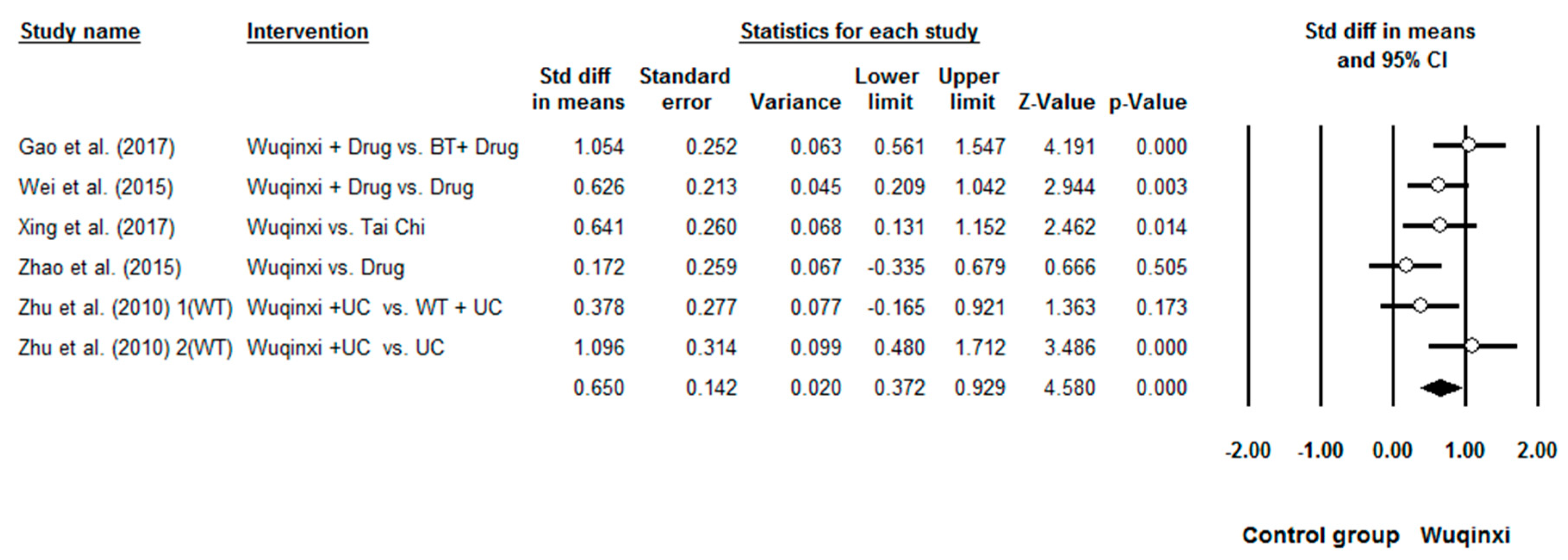
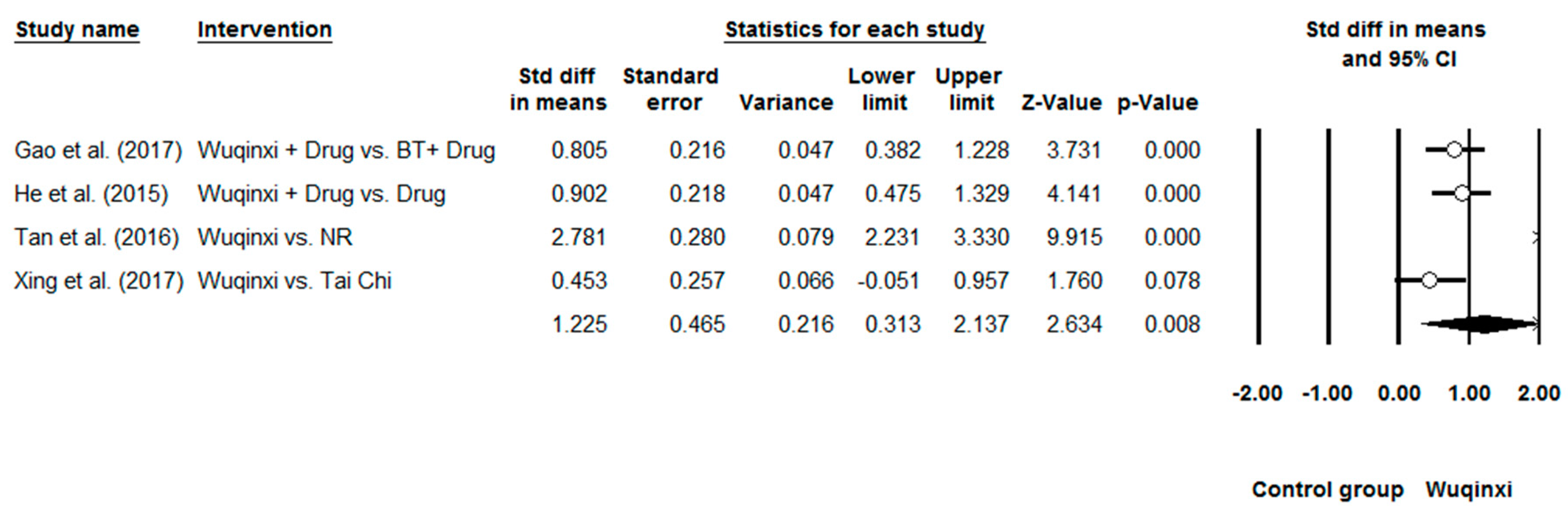
3.3. Meta-Analysis of Outcomes Measured
3.4. Moderator Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Guan, W.J.; Zheng, X.Y.; Chung, K.F.; Zhong, N.S. Impact of air pollution on the burden of chronic respiratory diseases in China: Time for urgent action. Lancet 2016, 388, 1939–1951. [Google Scholar] [CrossRef]
- Lelieveld, J.; Evans, J.S.; Fnais, M.; Giannadaki, D.; Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; MacNee, W.; Agusti, A.; Anzueto, A.; Berg, B.; Buist, A.S.; Buist, A.S.; Calverley, P.M.; Chavannes, N.; Dillard, T.; et al. Standards for the diagnosis and treatment of patients with COPD: A summary of the ATS/ERS position paper. Eur. Respir. J. 2004, 23, 932–946. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.P.; Martinez, C.H. Chronic obstructive pulmonary disease comorbidities. Curr. Opin. Pulm. Med. 2016, 22, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Slok, A.H.M.; Bemelmans, T.C.H.; Kotz, D. The Assessment of Burden of COPD (ABC) Scale: A Reliable and Valid Questionnaire. COPD J. Chron. Obstr. Pulm. Dis. 2016, 13, 8–10. [Google Scholar] [CrossRef]
- Rainer, G.; Blagoi, M.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, L.; Horta, P.; Espinoza, J.; Aguilera, M.; Balmaceda, N.; Castro, A. Pedometers to enhance physical activity in COPD: A randomised controlled trial. Eur. Respir. J. 2015, 45, 347–354. [Google Scholar] [CrossRef]
- Cindy, L.; Mackney, J.; Jenins, S.; Hill, K. Does exercise training change physical activity in people with COPD? A systematic review and meta-analysis. Chron. Respir. Dis. 2012, 9, 17–26. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.E.; Wei, G.X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.C. Effects of Mind-Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.X.; Chen, K.W.; Kinser, P.A.; Chan, J.S.M.; Ren, Z. Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Han, J.; Tsang, W.; Yeung, A. Effects of Tai Chi on lower limb proprioception in adults aged over 55: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2018. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.; Zeng, N.; Wang, C.; Sun, L.A. Systematic Review with Meta-Analysis of Mindful Exercises on Rehabilitative Outcomes among Post-stroke Patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Xu, A.; Yin, Y.; Zhang, R. The potential effect of Wuqinxi exercise for primary osteoporosis: A systematic review and meta-analysis. Maturitas 2015, 82, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xu, M.; Wei, Z.; Hu, Q.; Chen, Y.; Yan, J.; Wei, Y. Beneficial effects of qigong wuqinxi in the improvement of health condition, prevention, and treatment of chronic diseases: Evidence from a systematic review. Evid. Based Complement. Alternat. Med. 2018, 3235950. [Google Scholar] [CrossRef] [PubMed]
- Pikhart, H.; Pikhartova, J. The Relationship between Psychosocial Risk Factors and Health Outcomes of Chronic Diseases: A Review of the Evidence for Cancer and Cardiovascular Diseases; WHO Regional Office for Europe: Copenhagen Ø, Denmark, 2015. [Google Scholar]
- Zhang, F.; Bai, Y.H.; Zhang, J. The Influence of “wuqinxi” exercises on the Lumbosacral Multifidus. J. Phys. Ther. Sci. 2014, 26, 881–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bin, X. Study on the Impact of “Health Qigong.WuQinxi” on the Physical Health of the University Students. In Proceedings of the 2015 International Conference on Social Science and Technology Education, Sanya, China, 11–12 April 2015; Volume 18, pp. 530–536. [Google Scholar] [CrossRef]
- Cheng, Y.F.; Wei, S.S.; He, R. Clinical effect of traditional HuaTuo Wuqinxi on patients with chronic obstructive pulmonary disease at a stable stage. J. Clin. Chin. Med. 2015, 5, 683–685. [Google Scholar] [CrossRef]
- He, R.; Cheng, Y.F.; Wei, S.S. Clinical study on improving the quality of life of patients with chronic obstructive pulmonary disease (COPD) with traditional Wuqinxi. J. Clin. Chin. Med. 2015, 7, 966–968. [Google Scholar] [CrossRef]
- Gao, Y.F.; Qu, Y.Y.; Chen, S.Y. Effects of wuqinxi exercise on pulmonary function and exercise tolerance in patients with transitional chronic obstructive pulmonary disease. Chin. J. Clin. Pathol. 2017, 37, 975–980. [Google Scholar] [CrossRef]
- Tan, P.H.; Liu, F.Y.; Zhang, J.H. Observation and study on the quality of life of patients with chronic obstructive pulmonary disease at a stable stage. J. Emerg. Med. Lingnan 2016, 21, 1671. [Google Scholar] [CrossRef]
- Wei, S.S.; Cheng, Y.F.; He, R. Effect of traditional Wuqinxi on lung function of patients with chronic obstructive pulmonary disease at a stable stage. J. Clin. Chin. Med. 2015, 6, 793–795. [Google Scholar] [CrossRef]
- Xing, Y.P.; Xing, J.; Xiao, L. Effect of taijiquan combined with wuqinxi on exercise endurance and CCQ score of patients with COPD stabilit. J. Tradit. Chin. Med. 2017, 18, 83–86. [Google Scholar]
- Zhao, Q. Clinical study on the prevention and treatment of community stable chronic obstructive pulmonary disease by Wuqinxi. Chin. J. Tradit. Chin. Med. 2015, 30, 801–803. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, N.; Jin, H.Z. Effect of early intervention of wuqinxi on patients with stable chronic obstructive pulmonary disease. J. Liaoning Univ. Tradit. Chin. Med. 2010, 6, 107–110. [Google Scholar]
- Zhang, B.; Ru, L.; Lin, H.; Liang, J.; Lao, C.; Peng, D.; Cheng, C. Dissemination and Development of Wuqinxi in Singapore. Open J. Soc. Sci. 2016, 4, 264–271. [Google Scholar] [CrossRef]
- You, K. Study on the movement of new Qigong “WuQinXi” exercise for lumbar spinal disease: Based on 20 Mode, 30 Mode, 40 Mode. J. Physiol. Pathol. Korean Med. 2014, 28, 129–136. [Google Scholar] [CrossRef]
- Henz, D.; Schöllhorn, W. EEG Brain Activity in Dynamic Health Qigong Training: Same Effects for Mental Practice and Physical Training? Front. Psychol. 2017, 7, 154. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, 336–341. [Google Scholar] [CrossRef]
- Elkins, R.; Moseley, M.; Sherrington, C. Growth in the Physiotherapy Evidence Database (PEDro) and use of the PEDro scale. Br. J. Sports Med. 2013, 47, 188–189. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Quan, X.; Hui, S.C.; Hu, X.; Chan, J.S.M.; Wang, C.; Boyden, S.D.; Sun, L.; Wang, H. Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Quan, X.; Boyden, S.D.; Wang, H. A Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 600. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.A.; Wang, H. Effects of Mind-Body Exercises for Mood and Functional Capabilities in Patients with Stroke: An Analytical Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 721. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Chiou, S.Y.; Zeng, N.; Tzeng, H.-M.; Wang, L.; Ren, Z.; Dean, T.; Thomas, G.A. Effects of Mind–Body Movements on Balance Function in Stroke Survivors: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 1292. [Google Scholar] [CrossRef] [PubMed]
- Higgins, P.; Thompson, G.; Deeks, J.; Altman, G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.L.; Lin, Z.K.; Weng, H.D.; Qi, Q.F.; Lu, J.; Liu, K.X. Effectiveness of meditative movement on COPD: A systematic review and meta-analysis. Int. J. Chron. Obstr. Pulm. Dis. 2018, 13, 1239–1250. [Google Scholar] [CrossRef] [PubMed]
- Ngai, S.P.; Jones, A.Y.; Tam, W.W. Tai Chi for Chronic Obstructive Pulmonary Disease (COPD). Cochrane Database Syst. Rev. 2016, CD009953. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.C.; Pan, L.; Hu, Q.; Dong, W.P.; Yan, J.H.; Dong, L. Effects of yoga training in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Thorac. Dis. 2014, 6, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.J.; Ren, Z.; Wang, L.; Wei, G.-X.; Zou, L. Mind-Body (Baduanjin) Exercise Prescription for Chronic Obstructive Pulmonary Disease: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1830. [Google Scholar] [CrossRef] [PubMed]
- Oga, T.; Nishimura, K.; Tsukino, M.; Sato, S.; Hajiro, T.; Mishima, M. Exercise capacity deterioration in patients with COPD: Longitudinal evaluation over 5 years. Chest 2005, 128, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Burtin, C.; Boever, P. COPD and exercise: Does it make a difference? Breathe 2016, 12, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Tantucci, C.; Modina, D. Lung function decline in COPD. Int. J. Chron. Obstr. Pulm. Dis. 2012, 7, 95–99. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Location (Language) | Participant Characteristics | Intervention Program | Wuqinxi Training | Outcome Measured | Adverse Event; Follow-Up | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size (AT) | Mean Age or Age Range | Course of Disease (year) | Frequency (weekly) | Time (min) | Duration (week) | |||||
| Chen, et al. (2015) [19] | Anhui, China (Chinese) | 100 (10.34%) | WQ: 58.66 (7.56) CG: 58.64(7.52) | 14.52 (5.96) | WQ: Wuqinxi CG: Usual Care | 4 | 30 | 24 | Quality of life (CAT) | No; No |
| He et al. (2015) [20] | Anhui, China (Chinese) | 93 (7.00%) | WQ: 58.66 (7.56) CG: 58.64 (7.52) | 14.52 (5.96) | WQ: Wuqinxi + Drug Therapy CG: Drug Therapy | 4 | 30 | 24 | Quality of life (ZSH) | No; No |
| Gao et al. (2016) [21] | Guangdong, China (Chinese) | 74 (2.70%) | WQ: 67.14 (9.08) CG: 66.03 (8.18) | WQ: 13.69 (5.67) CG: 14.78 (9.24) | WQ: Wuqinxi + Drug Therapy CG: Breathing training + Drug Therapy | 14 | 30 | 24 | Lung function (FEV1, FEV1%, FEV1/FVC) Exercise Capacity (6-MWT) | No; No |
| Tan et al. (2017) [22] | Guangdong, China (Chinese) | 100 (0%) | WQ: 67.72 (9.26) CG: 74.24 (9.10) | NR | WQ: Wuqinxi CG: NR | 7 | 45 | 24 | Quality of life (CCQ) | No; No |
| Wei et al. (2015) [23] | Anhui, China (Chinese) | 93 (7.00%) | WQ: 58.66 (7.56) CG: 58.64 (7.52) | 14.52 (5.96) | WQ: Wuqinxi + Drug Therapy CG: Drug Therapy | 4 | 30 | 24 | Lung function (FEV1%, FEV1/FVC) | No; No |
| Xing et al. (2017) [24] | Tainting, China (Chinese) | 93 (0%) | WQ: 57.58 (7.47) TC: 59.00 (7.84) | WQ: 7.96 (1.36) TC: 7.25 (1.58) | WQ: Wuqinxi TC: Tai chi | 4 | 45 | 12 | Exercise Capacity (6-MWT) Lung function (FEV1%, FEV1/FVC), Quality of life (CCQ) | No; No |
| Zhao et al. (2015) [25] | Zhengzhou, China (Chinese) | 60 (0%) | WQ: 58.91 (5.86) CG: 56.66 (6. 43) | WQ: 6.81 (2.34) CG: 6.52 (2.42) | WQ: Wuqinxi CG: Drug Therapy | 3 | 40 | 12 | Lung function (FEV1, FEV1%, FEV1/FVC), Exercise Capacity (6-MWT) | No; No |
| Zhu et al. (2010) [26] | Nanjing, China (Chinese) | 74 (5.12%) | WQ: 53.53 (10.05) WT: 55.12 (11.41) CG: 55.46 (9.87) | NR | WQ: Wuqinxi + Usual Care WT: Walking training + Usual Care CG: Usual Care | 7 | 45 | 12 | Lung function (FEV1, FEV1%, FEV1/FVC) Exercise Capacity (6-MWT) | No; No |
| Author [Reference] | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Chen, et al. (2015) [19] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| He, et al. (2015) [20] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Gao, et al. (2017) [21] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 8 |
| Tan, et al. (2016) [22] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Wei, et al. (2015) [23] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 7 |
| Xing, et al. (2017) [24] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Zhao, et al. (2015) [25] | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Zhu, et al. (2010) [26] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Outcomes | Number of Comparisons | Meta-Analysis | Heterogeneity | Publication Bias | ||||
|---|---|---|---|---|---|---|---|---|
| SMD | 95% CI | p-Value | I2 % | Q-Value | df (Q) | Egger’s Test (e) | ||
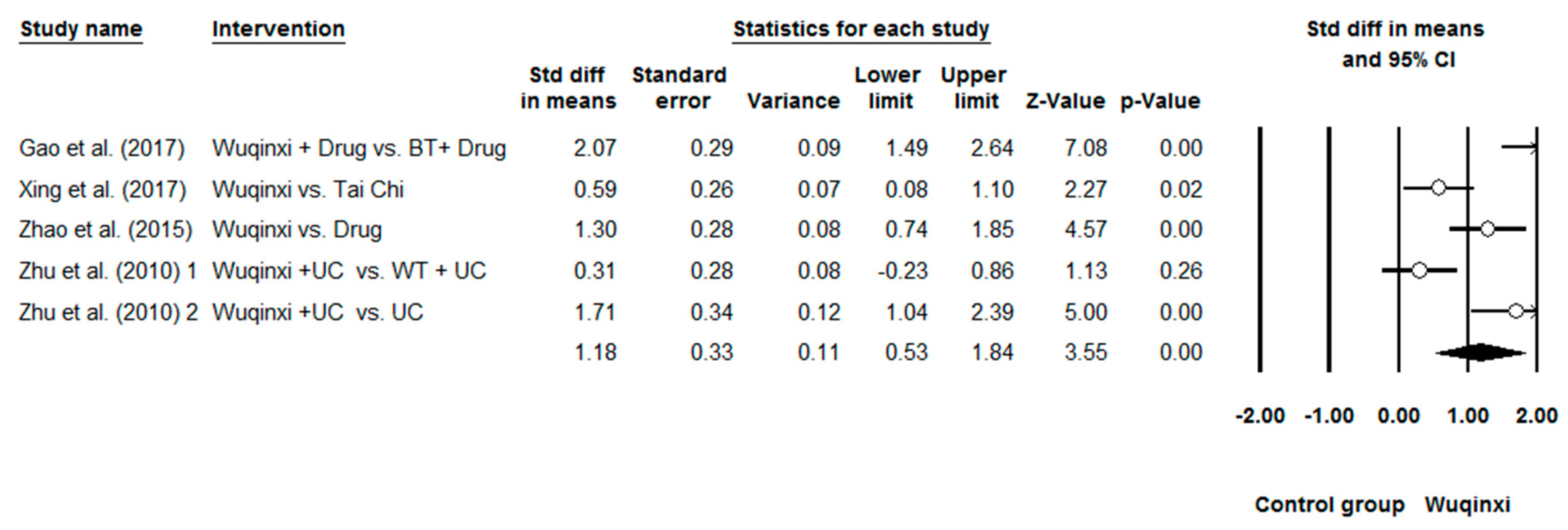
| 6MW | 5 | 1.18 | 0.530 to 1.84 | 0.00 | 84.97% | 26.61 | 4 | 0.24 |
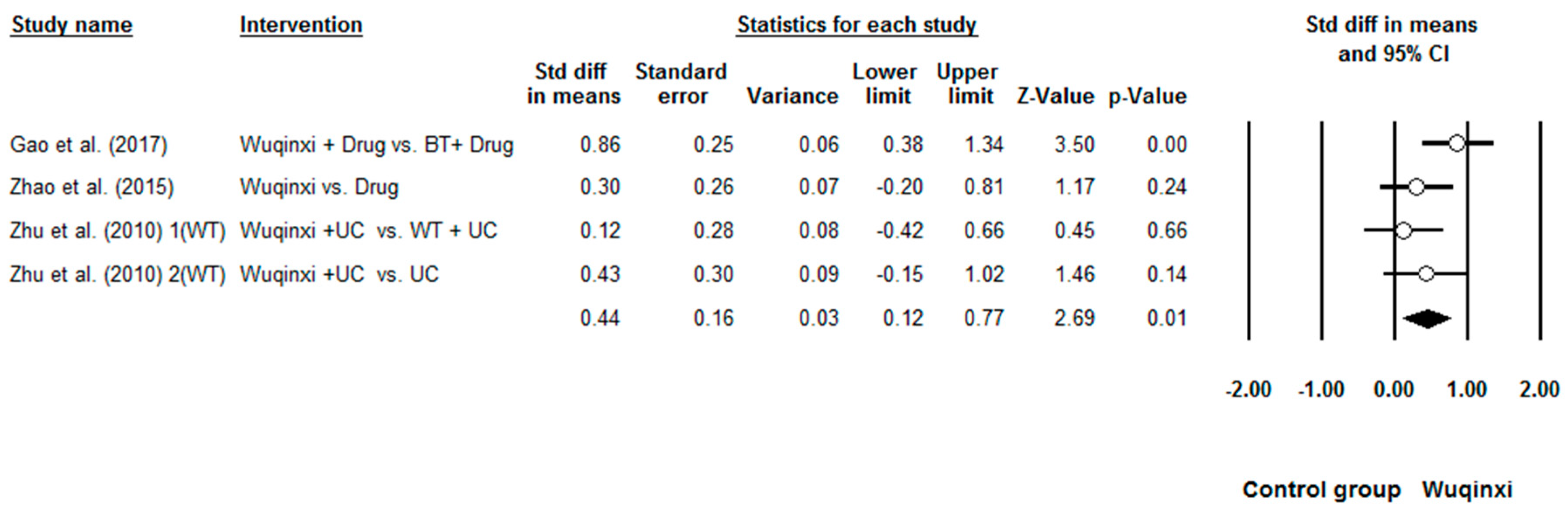
| FEV1 | 4 | 0.44 | 0.12 to 0.77 | 0.00 | 33.77% | 4.53 | 3 | 0.44 |
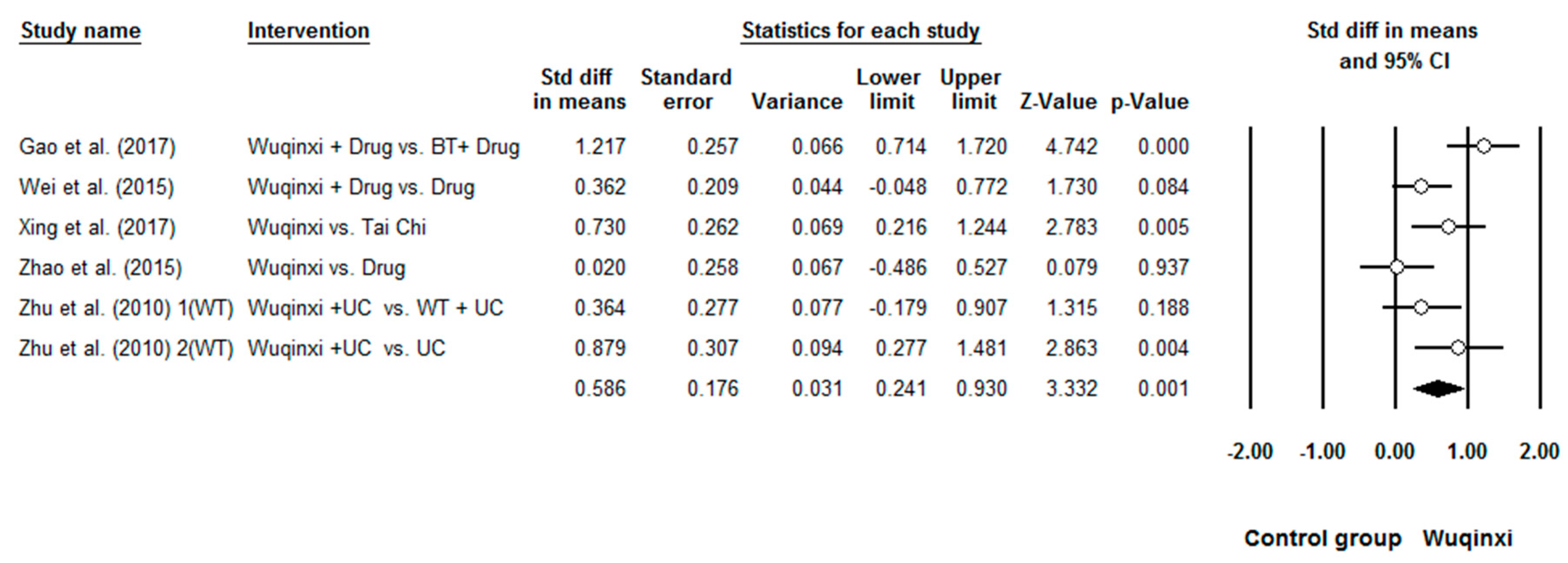
| FEV1% | 6 | 0.59 | 0.24 to 0.93 | 0.00 | 63.79% | 13.81 | 5 | 0.55 |
| FEV1/FVC | 6 | 0.65 | 0.37 to 0.93 | 0.00 | 44.32% | 8.90 | 5 | 0.72 |
| CCQ | 4 | 1.23 | 0.31 to 2.14 | 0.01 | 93.32% | 44.92 | 3 | 0.35 |
| Outcomes | Continuous Predictors | Number of Comparisons | β | 95% CI | Q-Value | df (Q) | p-Value |
|---|---|---|---|---|---|---|---|
| 6MW | Total training time | 5 | 0.00014 | 0.00005 to 0.00022 | 10.66 | 1 | 0.001 |
| FEV1 | Total training time | 4 | 0.00007 | −0.00000 to 0.00015 | 3.50 | 1 | 0.06 |
| FEV1% | Total training time | 6 | 0.00011 | 0.00004 to 0.00008 | 9.04 | 1 | 0.003 |
| FEV1FVC | Total training time | 6 | 0.00008 | 0.00001 to 0.00015 | 4.38 | 1 | 0.036 |
| CCQ | Total training time | 3 | 0.00007 | 0.00000 to 0.00014 | 4.18 | 1 | 0.04 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, K.; Liu, S.; Kong, Z.; Zhang, Y.; Liu, J. Mind-Body Exercise (Wuqinxi) for Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010072
Wang K, Liu S, Kong Z, Zhang Y, Liu J. Mind-Body Exercise (Wuqinxi) for Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2019; 16(1):72. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010072
Chicago/Turabian StyleWang, Ke, Shijie Liu, Zhaowei Kong, Yanjie Zhang, and Jing Liu. 2019. "Mind-Body Exercise (Wuqinxi) for Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 16, no. 1: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010072