Reevaluation of Historical Exposures to Ethylene Oxide Among U.S. Sterilization Workers in the National Institute of Occupational Safety and Health (NIOSH) Study Cohort

Abstract
:1. Introduction
2. Materials and Methods
2.1. E/IH Model Focus
- (1)
- Implanting efficacy test samples into selected boxes of materials on pallets to be sterilized
- (2)
- Loading pallets of materials to be sterilized into a chamber
- (3)
- Adding EO as a mixed or pure gas to the chamber to the desired level (kill concentration)
- (4)
- Running the chamber under the desired temperature and relative humidity conditions for a duration to achieve the desired level of microbial mortality
- (5)
- Exhausting some EO gas from chambers to in-room water traps (inefficient traps released EO into work room air)
- (6)
- In some cases, implementing air/nitrogen washes to reduce remaining EO concentrations in chamber air and residue levels in sterilized materials before unloading the chamber (no or few washes were used during the time frame of interest)
- (7)
- Unloading the processed materials from the chamber (released EO into work room air)
- (8)
- Removing test samples from boxes for efficacy analysis (operators in close contact with off-gassing packaging and materials emitting EO into work room air)
- (9)
- Transporting the sterilized materials to a storage area in or separate from the work room, and working in the storage area where materials remained until returned to customers (sterilized packaging and materials continue to off-gas during storage contributing additional EO to work room or storage room air)
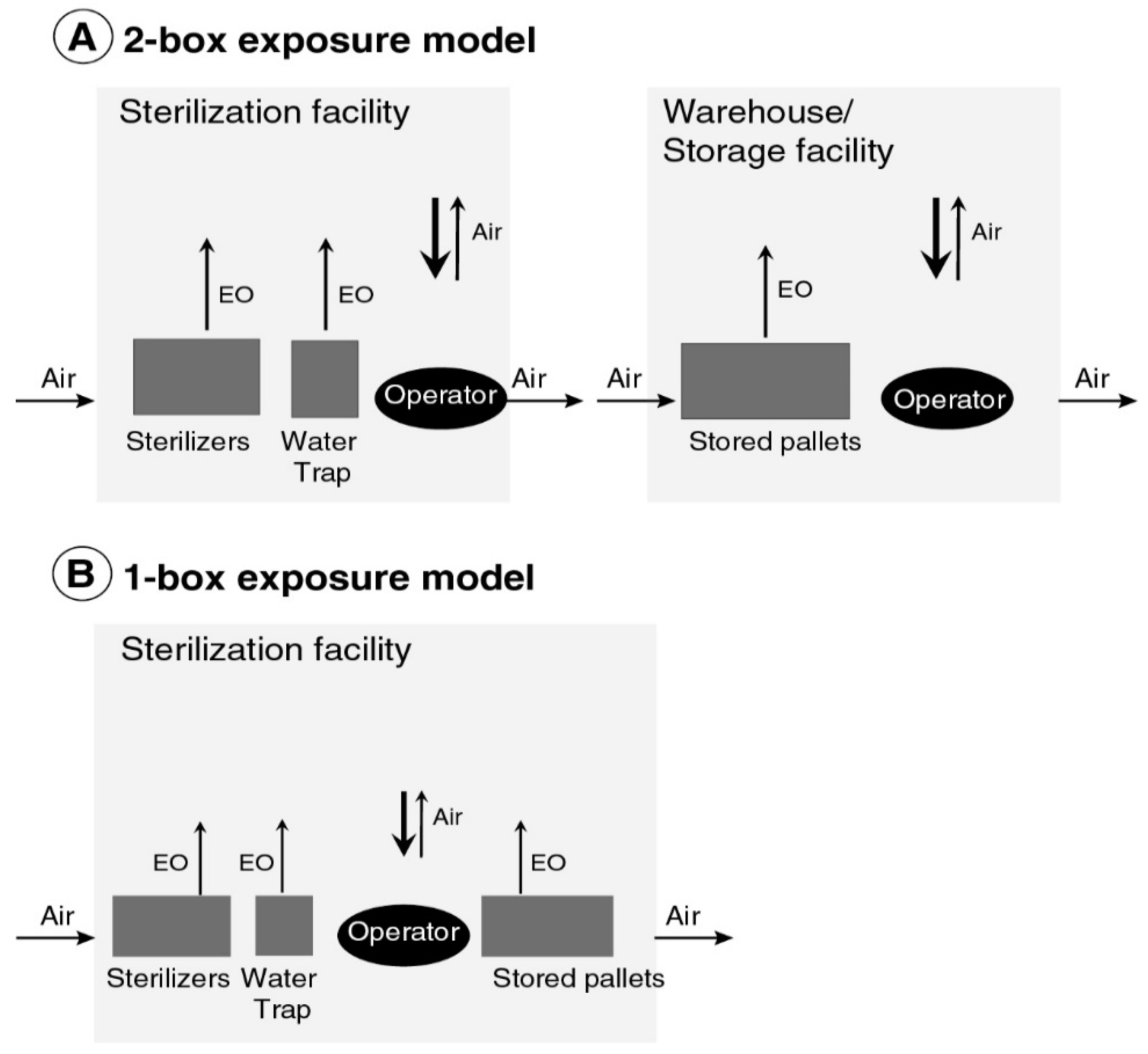
2.2. E/IH Model Structure and Parameters
- accumulation of EO in a room in which sterilization operations occurred, resulting from emissions from chambers and water traps for exhausted gas;
2.2.1. Compartment Volumes
2.2.2. Air Exchange Rate
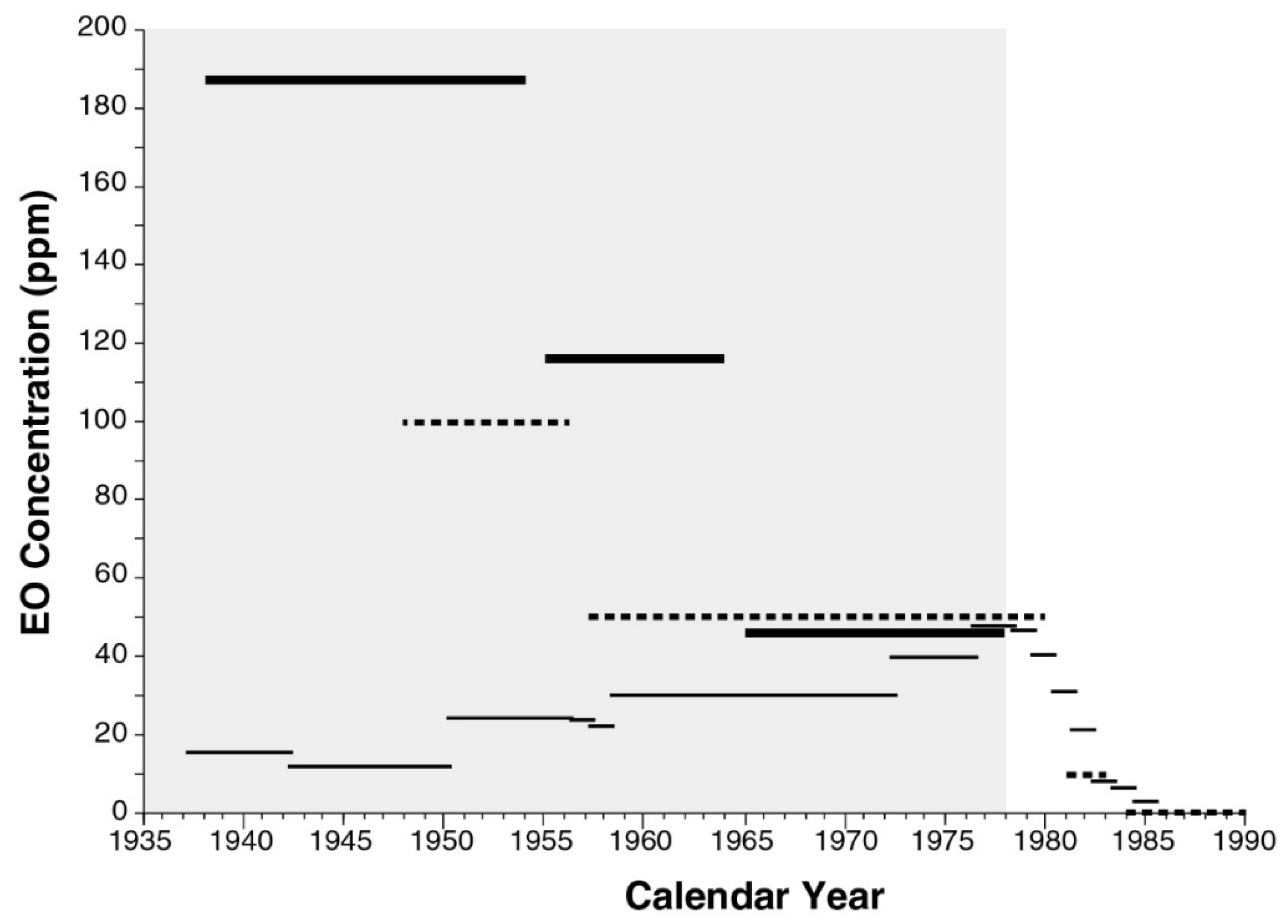
2.2.3. EO Concentration in Sterilization Chambers
2.2.4. Wash Cycles
2.2.5. Storage of Sterilized Materials
2.2.6. Rate of EO De-Gassing
2.2.7. Fraction (Fch) of Mair Attributable to EO in Chamber Void
2.2.8. EO Concentration in Worker Breathing Zone Due to EO Density
2.3. E/IH Model Calibration
2.4. Model Prediction Uncertainty
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- USEPA. Evaluation of the Inhalation Carcinogenicity of Ethylene Oxide (CASRN 75-21-8) in Support of Summary Information on the Integrated Risk Information System; EPA/635/R-16/350Fa; U.S. Environmental Protection Agency, Office of Research and Development: Washington, DC, USA, 2016.
- Steenland, K.; Stayner, L.; Greife, A.; Halperin, W.; Hayes, R.; Hornung, R.; Nowlin, S. Mortality among workers exposed to ethylene oxide. N. Engl. J. Med. 1991, 324, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Steenland, K.; Whelan, E.; Deddens, J.; Stayner, L.; Ward, E. Ethylene oxide and breast cancer incidence in a cohort study of 7576 women (United States). Cancer Causes Control 2003, 14, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Stayner, L.; Steenland, K.; Greife, A.; Hornung, R.; Hayes, R.B.; Nowlin, S.; Morawetz, J.; Ringenburg, V.; Elliot, L.; Halperin, W. Exposure-response analysis of cancer mortality in a cohort of workers exposed to ethylene oxide. Am. J. Epidemiol. 1993, 138, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Steenland, K.; Stayner, L.; Deddens, J. Mortality analyses in a cohort of 18,235 ethylene oxide exposed workers: Follow up extended from 1987 to 1998. Occup. Environ. Med. 2004, 61, 2–7. [Google Scholar] [PubMed]
- Greife, A.L.; Hornung, R.W.; Stayner, L.G.; Steenland, K.N. Development of a model for use in estimating exposure to ethylene oxide in a retrospective cohort mortality study. Scand. J. Work Environ. Health 1988, 14 (Suppl. 1), 29–30. [Google Scholar]
- Hornung, R.W.; Greife, A.L.; Stayner, L.T.; Steenland, N.K.; Herrick, R.F.; Elliott, L.J.; Ringenburg, V.L.; Morawetz, J. Statistical model for prediction of retrospective exposure to ethylene oxide in an occupational mortality study. Am. J. Ind. Med. 1994, 25, 825–836. [Google Scholar] [CrossRef] [PubMed]
- USEPA. Science Advisory Board Review of the EPA’s Evaluation of the Inhalation Carcinogenicity of Ethylene Oxide (Revised External Review Draft—August 2014); EPA-SAB-15-012 (2015 SAB Review); U.S. Environmental Protection Agency: Washington, DC, USA, 2015; p. 18.
- Von Grote, J.H.M. Occupational Exposure Assessment in Metal Degreasing and Dry Cleaning—Influences of Technology Innovation and Legislation. Ph.D. Dissertation, Swiss Federal Institute of Technology, Zürich, Switzerland, 2003. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.628.1123&rep=rep1&type=pdf (accessed on 3 January 2019).
- Von Grote, J.; Hürlimann, C.; Scheringer, M.; Hungerbühler, K. Reduction of occupational exposure to perchloroethylene and trichloroethylene in metal degreasing over the last 30 years: Influences of technology innovation and legislation. J Expo Anal. Environ. Epidemiol. 2003, 13, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Von Grote, J.; Hürlimann, C.; Scheringer, M.; Hunger, K. Assessing occupational exposure to perchloroethylene in dry cleaning. J. Occup. Environ. Hyg. 2006, 3, 606–619. [Google Scholar] [CrossRef] [PubMed]
- ACGIH. Documentation of the TLVs and BEIs: Ethylene Oxide; American Conference of Governmental Industrial Hygienists: Cincinnati, OH, USA, 2015.
- FDA. Ethylene Oxide, Ethlyene Chlorohydrin, and Ethylene Glycol: Proposed Maximum Residue Limits and Maximum Levels of Exposure; 43 FR 27474; Food and Drug Administration: Washington, DC, USA, 1978.
- OSHA. Ethylene Oxide (EtO) Standard; 29 CFR 1910.1047; The Occupational Safety and Health Administration: Washington, DC, USA, 1984.
- SCOEL. Recommendation from the Scientific Committee on Occupational Exposure Limits for Ethylene Oxide; SCOEL/SUM/160; European Commission, Employment, Social Affairs & Inclusion: Brussels, Belgium, June 2012. [Google Scholar]
- Goldgraben, R.; Zank, N. Mitigation of Worker Exposure to Ethylene Oxide; Report Prepared for the U.S. Environmental Protection Agency; MTR-80 W333; Appendix C-10: Practices Relevant to Worker Exposure at Spice Industry Sites; The Mitre Corp.: McLean, VA, USA, March 1981; pp. C153–C175. [Google Scholar]
- Vollrath. General Specification, Corrugated Containers & Components for Purchased Products; Vollrath: Sheboygan, WI, USA, 2010; Available online: https://vollrath.com/Vollrath-Files/Suppliers/MIS_GeneralSpecificationCorrugatedContainersComponents_en_2010-04-30.pdf (accessed on 3 January 2019).
- Andersen, L.; Delvers, M.; Hu, E. An Introduction to Gas Diffusion Sterilization. MD&DI Magazine, 1 May 1997; 1–8. [Google Scholar]
- Perkins, J.J. Principles and Methods of Sterilization in Health Sciences, 1st ed.; Charles C. Thomas Publisher: Springfield, IL, USA, 1956; pp. 325–334. [Google Scholar]
- Perkins, J.J. Principles and Methods of Sterilization in Health Sciences, 2nd ed.; Charles C. Thomas Publisher: Springfield, IL, USA, 1969; pp. 501–530. [Google Scholar]
- Bruch, C.W. Gaseous sterilization. Annu. Rev. Microbiol. 1961, 15, 245–262. [Google Scholar] [CrossRef]
- Bruch, C.W. Sterilization of plastics: Toxicity of ethylene oxide residues. In Industrial Sterilization, Proceedings of the International Symposium, Amsterdam, The Netherlands, 2–4 May 1972; Phillips, G.B., Miller, W.S., Eds.; Duke University Press: Durham, NC, USA, 1972; pp. 49–78. [Google Scholar]
- Buonicore, A.J.; Desai, P.R.; Mangone, M.A. Post Evacuation Cycle Modifications to Reduce Ethylene Oxide Residual Levels and Worker Exposure. Presented at the Medical Device and Diagnostic Industries (MD & DI) East, New York, NY, USA, 14–17 May 1984; Chemrox Inc.: Bridgeport, CT, USA, 1984. [Google Scholar]
- Stetson, J.B.; Whitbourne, J.E.; Eastman, C. Ethylene oxide degassing of rubber and plastic materials. Anesthesiol 1976, 44, 174–180. [Google Scholar] [CrossRef]
- White, J.D. Standard aeration for gas-sterilized plastics. J. Hyg. 1977, 79, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, T.; Schellhaas, H. Computation of the percentage points and the power for the two-sided Kolmogorov-Smirnov one sample test. Stat. Pap. 1998, 39, 361–375. [Google Scholar] [CrossRef]
- Burgess, D.F.; Reich, R.R. Industrial ethylene oxide sterilization in sterilization technology. In Sterilization Technology: A Practical Guide to Manufacturers and Users of Health Care Products, 1st ed.; Morrissey, R.F., Phillips, G.B., Eds.; Van Nostrand Reinhold: New York, NY, USA, 1993; pp. 153–194. [Google Scholar]
- USEPA. Ethylene Oxide Emissions from Commercial Sterilization/Fumigation Operations—Background Information for Proposed Standards; Final EPA-453/D-93-016; U.S. Environmental Protection Agency, Office of Air Quality Planning and Standards: Research Triangle Park, NC, USA, March 1993. Available online: http://nepis.epa.gov/Exe/ZyPDF.cgi?Dockey=00002URQ.PDF (accessed on 3 January 2019).
- Lehman, E.; (Industry Studies Branch, NIOSH, Cincinnati, OH, USA). Personal communication, 5 January 2005.
- NIOSH. Data File of NIOSH Regression-Model-Based Summary (De-Identified) Estimates of Annual, Facility- and Job-Code-Specific EO Exposure for the NIOSH Sterilization Worker Cohort; National Institute of Occupational Safety and Health: Cincinnati, OH, USA, 2004.
- Wolfram Research. Wolfram Language and System Documentation Center; Wolfram Research, Inc.: Champaign, IL, USA, 2019; Available online: http://reference.wolfram.com/language/ (accessed on 15 November 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date Range | Source a | Acceptable EO Concentration (ppm) |
|---|---|---|
| 1948–1956 | ACGIH TLV-TWA | 100 |
| 1957–1980 | ACGIH TLV-TWA | 50 |
| 1978 (proposed) | FDA Maximum Residue Level | 5–250 |
| 1981–1983 | ACGIH TLV-TWA | 10 |
| 1984–present | ACGIH TLV-TWA, A2 suspected human carcinogen | 1 |
| 1984–present | OSHA PEL-TWA | 1 |
| 2012–present | EC SCOEL implied 10−6 risk | 0.0015 |
| 2016–present | EPA IRIS estimated 10−6 risk | 0.0000001 |
| Model Parameter a | Sterilized Product Type | |
|---|---|---|
| Medical/Health | Spices | |
| Chamber, pallet volume per pallet | 3.0, 2.0 m3/pallet a | 18, 12 m3/chamber a |
| Void fraction | 1/3 a | 1/3 a |
| Air exchange rate (AER) b | 0.25–4.0/h | 0.25–4.0/h |
| Container/packaging mass | 1.5 kg/box a,c | 0.5 kg/bag a |
| Total container/packaging mass | 24 kg/pallet d | 48 kg/chamber |
| EO ad/absorbed in packaging, and in TM | 10%, 2% w/w e | 10%, 2% w/w e |
| TM mass | 300 kg/pallet f | 4,800 kg/chamber f |
| E/IH Model Assumption a | Early Period (1938–1954) | Middle Period (1955–1964) | Late Period (1965–1978) | |
|---|---|---|---|---|
| Medical/Health | Medical/Health | Medical/Health | Spices | |
| Commercial operation | Starting (small rooms for chambers and material storage) | Expanding (larger rooms for chambers and material storage) | Further expanding (large rooms for chambers) | Further expanding (large rooms for chambers) |
| Sterilizer operation | Manual | Manual | Manual and automated | Manual and automated |
| Chamber size | Small (self-manufactured) | Small or mixed | Mixed size or large | Mixed size or large |
| Chamber operation | Under pressure | Under pressure | Under pressure or vacuum | Under pressure or vacuum |
| Loading/unloading | Hand | Pallet jack | Pallet jack | Pallet jack |
| Separate rooms for sterilization versus storage | No | No | Yes (no aeration) | No |
| Vacuum/wash cycles per treatment | 0 a | 1 a | 1–2 a | 2 b |
| Final EO concentration in sterilizer chamber air c | 17,800 ppm | 17,200 ppm | 11,500 ppm c | 5560 ppm |
| Sterilizer size and number: a #sterilizers/#palettes | 4/2 | 9/2 | 2/2 + 3/3 + 1/6 | 2/6 |
| Sterilization (warehouse/storage) room volume | 4800 (NA) m3 d | 11,600 (NA) m3 d | 11,000 (8500) m3 a | 3100 (NA) m3 b |
| Hours per shift | 8 | 8 | 8 | 8 |
| Min/day in sterilization (warehouse/store) room | 480 (NA) | 480 (NA) | 280 (180) a | 480 (NA) b |
| Residual EO in sterilizer chamber air (Mair) | 32.0 g | 31.0 g | 20.4 g | 59.4 g |
| Total packaging mass | 24 kg/pallet | 24 kg/pallet | 24 kg/pallet c | 48 kg/chamber |
| % EO retained post-cycle by packaging and TM e | 21% w/w | 14% w/w | 10.5% w/w | 7% w/w |
| EO retained by packaging (Mpack) | 504 g/pallet | 336 g/pallet | 252 g/pallet | 67.2 g/chamber |
| EO retained by TM (Mprod) | 1260 g/pallet | 840 g/pallet | 630 g/pallet | 14.4 kg/chamber |
| Scenario | Products Sterilized | Period | Model | ||||
|---|---|---|---|---|---|---|---|
| NSR | E/IH | ||||||
| 90th Percentile 8-h TWA EO Concentration, C90 a (ppm) | C90/(C90 Scenario 3) (ppm) | 90th Percentile 8-h TWA EO Concentration, C90 a (ppm) | C90/(C90 Scenario 3) (ppm) | Fraction Due to Storage | |||
| 1 | Medical/health | Early | 11.9 (7.90, 14.3) | 0.33 | 187 (124, 224) | 3.9 | 0.97 |
| 2 | Medical/health | Middle | 30.0 (19.9, 36.0) | 0.58 | 118 (78.2, 141) | 2.5 | 0.96 |
| 3 | Medical/health | Late | 47.4 (31.4, 56.8) | 1.0 | 47.8 (31.7, 57.3) | 1.0 | 0.95 |
| 4 | Spices | Late | – | – | 46.7 (31.0, 56.0) | 0.98 | 0.92 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogen, K.T.; Sheehan, P.J.; Valdez-Flores, C.; Li, A.A. Reevaluation of Historical Exposures to Ethylene Oxide Among U.S. Sterilization Workers in the National Institute of Occupational Safety and Health (NIOSH) Study Cohort. Int. J. Environ. Res. Public Health 2019, 16, 1738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101738
Bogen KT, Sheehan PJ, Valdez-Flores C, Li AA. Reevaluation of Historical Exposures to Ethylene Oxide Among U.S. Sterilization Workers in the National Institute of Occupational Safety and Health (NIOSH) Study Cohort. International Journal of Environmental Research and Public Health. 2019; 16(10):1738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101738
Chicago/Turabian StyleBogen, Kenneth T., Patrick J. Sheehan, Ciriaco Valdez-Flores, and Abby A. Li. 2019. "Reevaluation of Historical Exposures to Ethylene Oxide Among U.S. Sterilization Workers in the National Institute of Occupational Safety and Health (NIOSH) Study Cohort" International Journal of Environmental Research and Public Health 16, no. 10: 1738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101738