Public Health Messages Associated with Low UV Index Values Need Reconsideration

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
3.1. Dataset Description
3.2. Erythemal Doses and Proportion of Days Exceeding MEDs for Certain Time Intervals
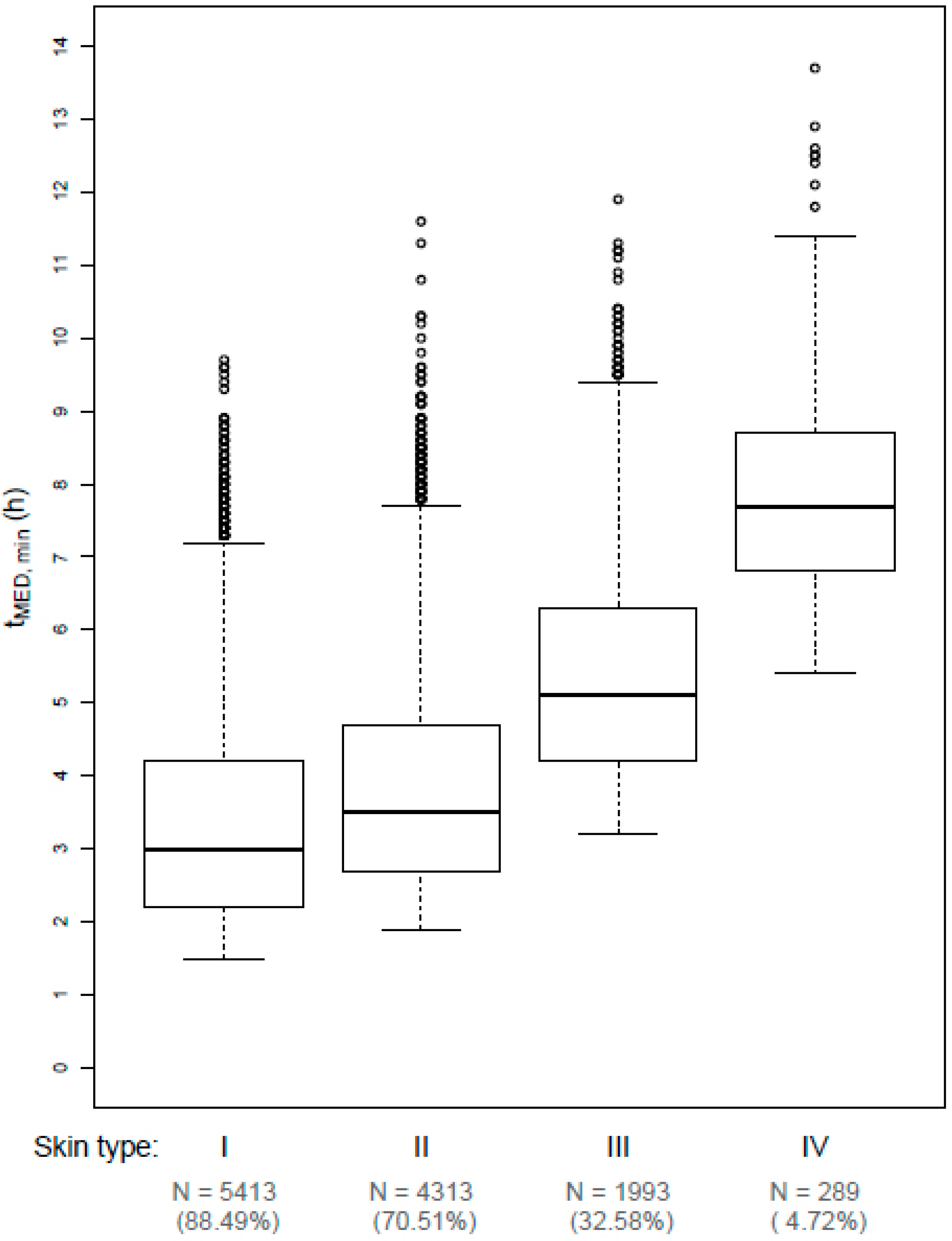
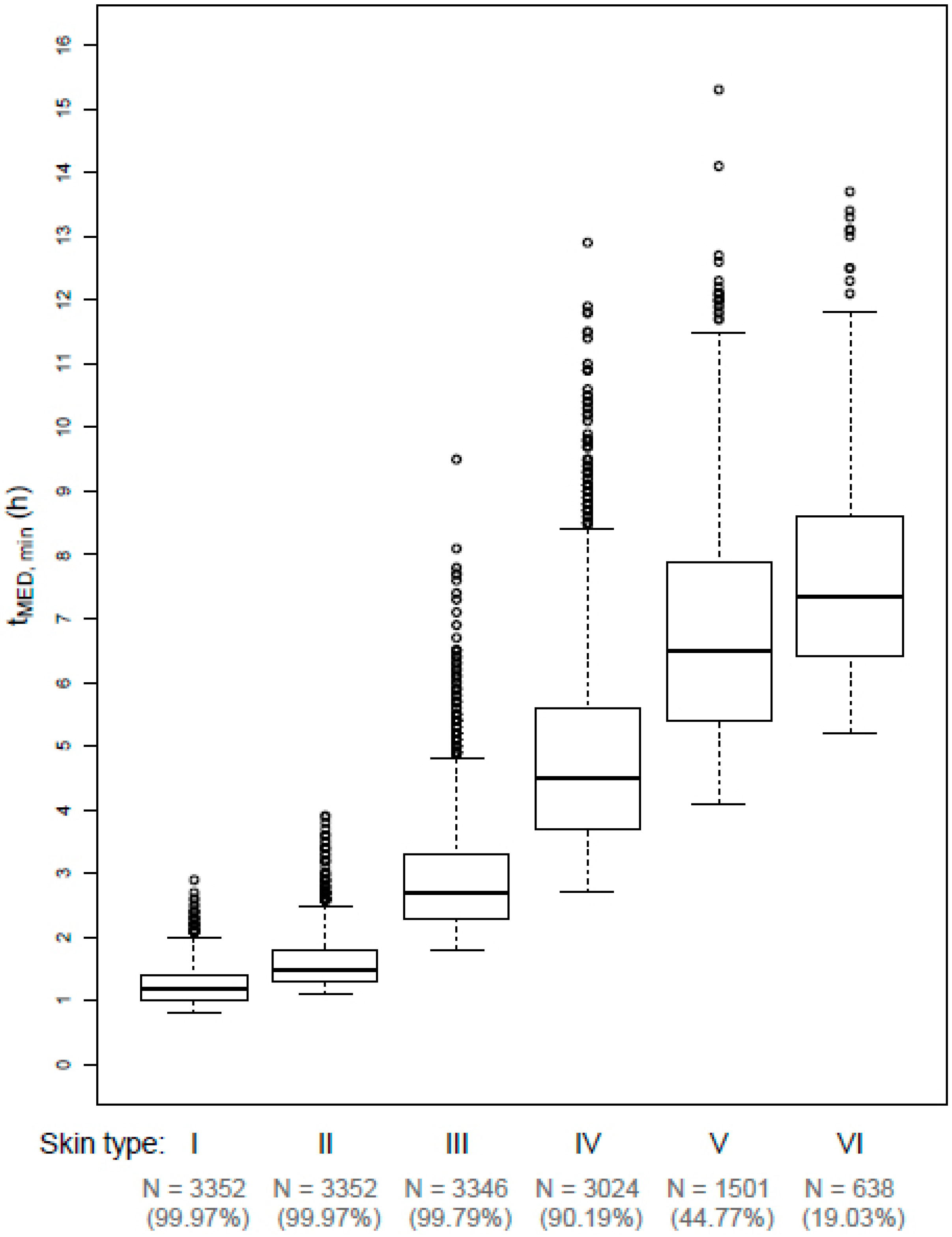
3.3. Minimal Exposure Durations to Receive one MED
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Agency for Research on Cancer. IARC working group on the evaluation of carcinogenic risk to humans. Radiation. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, no. 100d.; IARC: Lyon, France, 2012. [Google Scholar]
- Lucas, R.M.; McMichael, A.J.; Armstrong, B.K.; Smith, W.T. Estimating the global disease burden due to ultraviolet radiation exposure. Int. J. Epidemiol. 2008, 37, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Erdmann, F.; Lortet-Tieulent, J.; Schuz, J.; Zeeb, H.; Greinert, R.; Breitbart, E.W.; Bray, F. International trends in the incidence of malignant melanoma 1953-2008--are recent generations at higher or lower risk? Int. J. Cancer 2013, 132, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Leiter, U.; Eigentler, T.; Garbe, C. Epidemiology of skin cancer. Adv. Exp. Med. Biol. 2014, 810, 120–140. [Google Scholar] [PubMed]
- Gefeller, O.; Uter, W.; Pfahlberg, A.B. Protection from ultraviolet radiation during childhood: The parental perspective in Bavaria. Int. J. Environ. Res. Public Health 2016, 13, 1011. [Google Scholar] [CrossRef]
- Kasparian, N.A.; McLoone, J.K.; Meiser, B. Skin cancer-related prevention and screening behaviors: A review of the literature. J. Behav. Med. 2009, 32, 406–428. [Google Scholar] [CrossRef]
- Narayanan, D.L.; Saladi, R.N.; Fox, J.L. Review: Ultraviolet radiation and skin cancer. Int. J. Dermatol. 2010, 49, 978–986. [Google Scholar] [CrossRef]
- Stanton, W.R.; Janda, M.; Baade, P.D.; Anderson, P. Primary prevention of skin cancer: A review of sun protection in Australia and internationally. Health Promot. Int. 2004, 19, 369–378. [Google Scholar] [CrossRef]
- Stratton, S.P. Prevention of non-melanoma skin cancer. Curr. Oncol. Rep. 2001, 3, 295–300. [Google Scholar] [CrossRef]
- Beck, N.; Balanay, J.A.G.; Johnson, T. Assessment of occupational exposure to heat stress and solar ultraviolet radiation among groundskeepers in an eastern north carolina university setting. J. Occup. Environ. Hyg. 2018, 15, 105–116. [Google Scholar] [CrossRef]
- Morabito, M.; Grifoni, D.; Crisci, A.; Fibbi, L.; Orlandini, S.; Gensini, G.F.; Zipoli, G. Might outdoor heat stress be considered a proxy for the unperceivable effect of the ultraviolet-induced risk of erythema in florence? J. Photochem. Photobiol. B-Biol. 2014, 130, 338–348. [Google Scholar] [CrossRef]
- International Commission on Non-Ionizing Radiation Protection. Global Solar UV Index—A Joint Recommendation of the WHO, WMO, UNEP and the ICNIRP; International Commission on Non-Ionizing Radiation Protection: Oberschleissheim, Germany, 1995. [Google Scholar]
- Fioletov, V.; Kerr, J.B.; Fergusson, A. The UV index: Definition, distribution and factors affecting it. Can. J. Public Health. 2010, 101, I5–I9. [Google Scholar] [PubMed]
- Commission Internationale de l’Eclairage (CIE). Erythema reference action spectrum and standard erythema dose. In ISO 17166:1999(E)/CIE S 007/E-1998; CIE Central Bureau: Vienna, Austria, 1998.
- Webb, A.R.; Slaper, H.; Koepke, P.; Schmalwieser, A.W. Know your standard: Clarifying the cie erythema action spectrum. Photochem. Photobiol. 2011, 87, 483–486. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Solar UV Index: A Practical Guide; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Allinson, S.; Asmuss, M.; Baldermann, C.; Bentzen, J.; Buller, D.; Gerber, N.; Green, A.C.; Greinert, R.; Kimlin, M.; Kunrath, J.; et al. Validity and use of the UV index: Report from the UVI working group, Schloss Hohenkammer, Germany, 5–7 December 2011. Health Phys. 2012, 103, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Sandmann, H. Das solare UV-Messnetz des BfS/UBA. In StrahlenschutzPRAXIS; TÜV Media GmbH: Cologne, Germany, 2015; pp. 38–40. [Google Scholar]
- Schmalwieser, A.W.; Grobner, J.; Blumthaler, M.; Klotz, B.; De Backer, H.; Bolsee, D.; Werner, R.; Tomsic, D.; Metelka, L.; Eriksen, P.; et al. UV index monitoring in Europe. Photochem. Photobiol. Sci. 2017, 16, 1349–1370. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, M.; Sandmann, H.; Pfahlberg, A.B.; Uter, W.; Gefeller, O. Erythemal UV radiation on days with low UV index values—An analysis of data from the German solar UV monitoring network over a ten-year period. Photochem. Photobiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Feister, U.; Laschewski, G.; Grewe, R.D. UV index forecasts and measurements of health-effective radiation. J. Photochem. Photobiol. B 2011, 102, 55–68. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- International Commission on Non-Ionizing Radiation Protection. Guidelines on limits of exposure to ultraviolet radiation of wavelengths between 180 nm and 400 nm (incoherent optical radiation). Health Phys. 2004, 87, 171–186. [Google Scholar] [CrossRef]
- International Commission on Non-Ionizing Radiation Protection. Protection of workers against ultraviolet radiation. Health Phys. 2010, 99, 66–87. [Google Scholar] [CrossRef] [PubMed]
- Trenberth, K.E. What are the seasons. Bull. Am. Meteorol. Soc. 1983, 64, 1276–1282. [Google Scholar] [CrossRef]
- Repacholi, M.H. Global solar UV index. Radiat. Prot. Dosim. 2000, 91, 307–311. [Google Scholar] [CrossRef]
- Matthes, R. Global Solar UV-Index, Environmental UV-Radiation, Risk of Skin Cancer and Primary Prevention, Hamburg, Germany, 1996; Federal Ministry of the Environment, Nature Conservation and Nuclear Safety: Hamburg, Germany, 1996.
- Commission on Radiological Protection. Die neue Klassifikation des Solaren UV-Index (UVI)—Anpassung an Die Internationale Empfehlung der WHO; Commission on Radiological Protection: Bonn, Germany, 2004. [Google Scholar]
- Gies, P.; van Deventer, E.; Green, A.C.; Sinclair, C.; Tinker, R. Review of the global solar UV index 2015 workshop report. Health Phys. 2018, 114, 84–90. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. UV Index Scale. Available online: https://www.epa.gov/sunsafety/uv-index-scale-0 (accessed on 15 March 2019).
- United States Environmental Protection Agency. A Guide to the UV Index; United States Environmental Protection Agency: Washington, DC, USA, 2004.
- Australian Government Bureau of Meteorology. About UV and Sun Protection Times. Available online: http://www.bom.gov.au/uv/ (accessed on 15 March 2019).
- Lehmann, M.; Pfahlberg, A.B.; Sandmann, H.; Uter, W.; Gefeller, O. Implications of low levels of the UV index for sun protection. Stud. Health Technol. Inform. 2017, 243, 25–29. [Google Scholar] [PubMed]
- Lucas, R.M.; Neale, R.E.; Madronich, S.; McKenzie, R.L. Are current guidelines for sun protection optimal for health? Exploring the evidence. Photochem. Photobiol. Sci. 2018, 17, 1956–1963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, R.L.; Lucas, R.M. Reassessing impacts of extended daily exposure to low level solar UV radiation. Sci. Rep. 2018, 8, 13805. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Opinion on Biological Effects of Ultraviolet Radiation Relevant to Health with Particular Reference to Sunbeds for Cosmetic Purposes; Scientific Committee on Health, Environmental and Emerging Risks: Luxembourg, 2016. [Google Scholar]
- Eilers, S.; Bach, D.Q.; Gaber, R.; Blatt, H.; Guevara, Y.; Nitsche, K.; Kundu, R.V.; Robinson, J.K. Accuracy of self-report in assessing fitzpatrick skin phototypes i through viassessing fitzpatrick skin phototypes i-viassessing fitzpatrick skin phototypes i-vi. JAMA Dermatol. 2013, 149, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Zaratti, F.; Piacentini, R.D.; Guillen, H.A.; Cabrera, S.H.; Liley, J.B.; McKenzie, R.L. Proposal for a modification of the UVI risk scale. Photochem. Photobiol. Sci. 2014, 13, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Bunsen, R.; Roscoe, H. Photochemische untersuchungen. Annalen der Physik 1857, 176, 43–88. [Google Scholar] [CrossRef]
- Schindl, A.; Rosado-Schlosser, B.; Trautinger, F. The reciprocity rule in photobiology. A review. Hautarzt 2001, 52, 779. [Google Scholar] [CrossRef]
- Martin, J.W.; Chin, J.W.; Nguyen, T. Reciprocity law experiments in polymeric photodegradation: A critical review. Prog. Organ. Coat. 2003, 47, 292–311. [Google Scholar] [CrossRef]
- McKenzie, R.L.; Paulin, K.J.; Kotkamp, M. Erythemal UV irradiances at lauder, new zealand: Relationship between horizontal and normal incidence. Photochem. Photobiol. 1997, 66, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Sandmann, H.; Stick, C. Spectral and spatial UV sky radiance measurements at a seaside resort under clear sky and slightly overcast conditions. Photochem. Photobiol. 2014, 90, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Vernez, D.; Milon, A.; Vuilleumier, L.; Bulliard, J.L.; Koechlin, A.; Boniol, M.; Dore, J.F. A general model to predict individual exposure to solar UV by using ambient irradiance data. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Siani, A.M.; Casale, G.R.; Sisto, R.; Colosimo, A.; Lang, C.A.; Kimlin, M.G. Occupational exposures to solar ultraviolet radiation of vineyard workers in tuscany (italy). Photochem. Photobiol. 2011, 87, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.K.R.; Stewart, A.W.; McKenzie, R.L.; Reeder, A.I.; Liley, J.B.; Allen, M.W. Sun exposure and 25-hydroxyvitamin D3 levels in a community sample: Quantifying the association with electronic dosimeters. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Gefeller, O. The garment protection factor: Further advances in labelling sun-protective clothing. Br. J. Dermatol. 2018, 178, 835–836. [Google Scholar] [CrossRef] [PubMed]
- Gies, P. Photoprotection by clothing. Photodermatol. Photoimmunol. Photomed. 2007, 23, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Stanienda-Sokol, K.; Salwowska, N.; Slawinska, M.; Wicherska-Pawlowska, K.; Lorenc, A.; Wcislo-Dziadecka, D.; Wydmanski, J.; Majewski, W. Primary locations of malignant melanoma lesions depending on patients’ gender and age. Asian Pac. J. Cancer Prev. 2017, 18, 3081–3086. [Google Scholar] [PubMed]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80, 1678S–1688S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeeb, H.; Greinert, R. The role of vitamin D in cancer prevention: Does UV protection conflict with the need to raise low levels of vitamin D? Deutsches Arzteblatt Int. 2010, 107, 638–643. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skin Type | Skin Response to Sun Exposure | Classes of Individuals | MED (in SED) |
|---|---|---|---|
| I | Burns easily and severely (painful burn); tans little or none and peels | Melano-compromised | 2.0 |
| II | Usually burns easily and severely (painful burn); tans minimally or lightly, also peels | 2.5 | |
| III | Burns moderately and tans | Melano-competent | 4.0 |
| IV | Burns minimally, tans easily | 6.0 | |
| V | Rarely burns, tans easily and substantially | Melano-protected | 8.5 |
| VI | Never buns and tans profusely | 10.0 |
| Year | UVI 0 | UVI 1 | UVI 2 | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| 2007 | 526 | 10.6 | 616 | 10.1 | 343 | 10.2 |
| 2008 | 509 | 10.3 | 585 | 9.6 | 427 | 12.7 |
| 2009 | 570 | 11.5 | 534 | 8.7 | 258 | 7.7 |
| 2010 | 533 | 10.7 | 694 | 11.3 | 361 | 10.8 |
| 2011 | 482 | 9.7 | 618 | 10.1 | 307 | 9.2 |
| 2012 | 486 | 9.8 | 650 | 10.6 | 332 | 9.9 |
| 2013 | 488 | 9.8 | 632 | 10.3 | 322 | 9.6 |
| 2014 | 447 | 9.0 | 532 | 8.7 | 324 | 9.7 |
| 2015 | 453 | 9.1 | 604 | 9.9 | 340 | 10.1 |
| 2016 | 467 | 9.4 | 652 | 10.7 | 339 | 10.1 |
| Total | 4961 | 100.0 | 6117 | 100.0 | 3353 | 100.0 |
| Month | UVI 0 | UVI 1 | UVI 2 | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Jan | 1515 | 30.5 | 742 | 12.1 | 1 | 0.0 |
| Feb | 396 | 8.0 | 1526 | 24.9 | 249 | 7.4 |
| Mar | 54 | 1.1 | 674 | 11.0 | 1061 | 31.6 |
| Apr | 3 | 0.1 | 92 | 1.5 | 300 | 8.9 |
| May | 1 | 0.0 | 69 | 1.1 | 136 | 4.1 |
| Jun | 0 | 0.0 | 29 | 0.5 | 78 | 2.3 |
| Jul | 6 | 0.1 | 28 | 0.5 | 71 | 2.1 |
| Aug | 0 | 0.0 | 44 | 0.7 | 105 | 3.1 |
| Sep | 10 | 0.2 | 145 | 2.4 | 377 | 11.2 |
| Oct | 88 | 1.8 | 1047 | 17.1 | 913 | 27.2 |
| Nov | 939 | 18.9 | 1281 | 20.9 | 62 | 1.8 |
| Dec | 1949 | 39.3 | 440 | 7.2 | 0 | 0.0 |
| Total | 4961 | 100.0 | 6117 | 100.0 | 3353 | 100.0 |
| Time Interval (Local Solar Time, Duration) | Her (in SED); Median (p10, p90 Percentile) | Proportion of Days Exceeding one MED for Skin Type (in %) | |||||
|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | ||
| Before noon | |||||||
| 8:00–10:00, 2 h | |||||||
| UVI 0 | 0.12 (0.05, 0.23) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 0.42 (0.20, 0.86) | 0.07 | 0 | 0 | 0 | 0 | 0 |
| UVI 2 | 1.24 (0.69, 1.92) | 7.87 | 2.09 | 0 | 0 | 0 | 0 |
| 7:30–10:30, 3 h | |||||||
| UVI 0 | 0.19 (0.09, 0.36) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 0.67 (0.34, 1.31) | 1.03 | 0.15 | 0 | 0 | 0 | 0 |
| UVI 2 | 1.90 (1.11, 2.85) | 44.32 | 19.92 | 0.89 | 0 | 0 | 0 |
| Around noon | |||||||
| 11:45–12:15, 0.5 h | |||||||
| UVI 0 | 0.11 (0.05, 0.19) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 0.32 (0.20, 0.54) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 2 | 0.74 (0.43, 1.00) | 0 | 0 | 0 | 0 | 0 | 0 |
| 11:30–12:30, 1 h | |||||||
| UVI 0 | 0.23 (0.11, 0.37) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 0.64 (0.40, 1.05) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 2 | 1.46 (0.93, 1.96) | 7.75 | 0 | 0 | 0 | 0 | 0 |
| 11:00–13:00, 2 h | |||||||
| UVI 0 | 0.44 (0.21, 0.70) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 1.24 (0.80, 2.03) | 10.99 | 0.49 | 0 | 0 | 0 | 0 |
| UVI 2 | 2.83 (1.92, 3.80) | 87.89 | 68.65 | 5.37 | 0 | 0 | 0 |
| 10:30–13:30, 3 h | |||||||
| UVI 0 | 0.63 (0.31, 0.99) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 1.78 (1.15, 2.90) | 39.28 | 20.08 | 0 | 0 | 0 | 0 |
| UVI 2 | 4.08 (2.86, 5.45) | 98.39 | 95.38 | 52.82 | 2.42 | 0 | 0 |
| 10:00–14:00, 4 h | |||||||
| UVI 0 | 0.79 (0.39, 1.23) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 2.24 (1.43, 3.64) | 60.72 | 39.82 | 4.51 | 0 | 0 | 0 |
| UVI 2 | 5.14 (3.71, 6.88) | 99.79 | 99.14 | 84.01 | 26.39 | 0 | 0 |
| After noon | |||||||
| 14:00–16:00, 2 h | |||||||
| UVI 0 | 0.12 (0.05, 0.22) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 0.42 (0.20, 0.86) | 0.08 | 0 | 0 | 0 | 0 | 0 |
| UVI 2 | 1.24 (0.72, 1.92) | 7.99 | 2.42 | 0 | 0 | 0 | 0 |
| 13:30–16:30, 3 h | |||||||
| UVI 0 | 0.19 (0.08, 0.36) | 0 | 0 | 0 | 0 | 0 | 0 |
| UVI 1 | 0.67 (0.33, 1.32) | 1.32 | 0.25 | 0 | 0 | 0 | 0 |
| UVI 2 | 1.92 (1.16, 2.85) | 44.68 | 20.34 | 0.95 | 0 | 0 | 0 |
| Total day | |||||||
| Sunrise–Sunset | |||||||
| UVI 0 | 1.04 (0.52, 1.65) | 1.23 | 0.04 | 0 | 0 | 0 | 0 |
| UVI 1 | 3.21 (1.95, 5.46) | 88.49 | 70.51 | 32.58 | 4.72 | 0.07 | 0.02 |
| UVI 2 | 8.17 (6.01, 10.87) | 99.97 | 99.97 | 99.79 | 90.19 | 44.77 | 19.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehmann, M.; Pfahlberg, A.B.; Sandmann, H.; Uter, W.; Gefeller, O. Public Health Messages Associated with Low UV Index Values Need Reconsideration. Int. J. Environ. Res. Public Health 2019, 16, 2067. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122067
Lehmann M, Pfahlberg AB, Sandmann H, Uter W, Gefeller O. Public Health Messages Associated with Low UV Index Values Need Reconsideration. International Journal of Environmental Research and Public Health. 2019; 16(12):2067. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122067
Chicago/Turabian StyleLehmann, Maria, Annette B. Pfahlberg, Henner Sandmann, Wolfgang Uter, and Olaf Gefeller. 2019. "Public Health Messages Associated with Low UV Index Values Need Reconsideration" International Journal of Environmental Research and Public Health 16, no. 12: 2067. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122067