The Quality of Caregivers for the Elderly in Long-Term Care Institutions in Zhejiang Province, China

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Data Collection
2.3. Statistical Analyses
3. Results
3.1. Socio-Demographic Characteristics
3.2. Knowledge on Elderly Care
3.3. Attitude towards Elderly Care
3.4. Practice Regarding Elderly Care
3.5. Factors Influencing Knowledge, Attitude and Practice
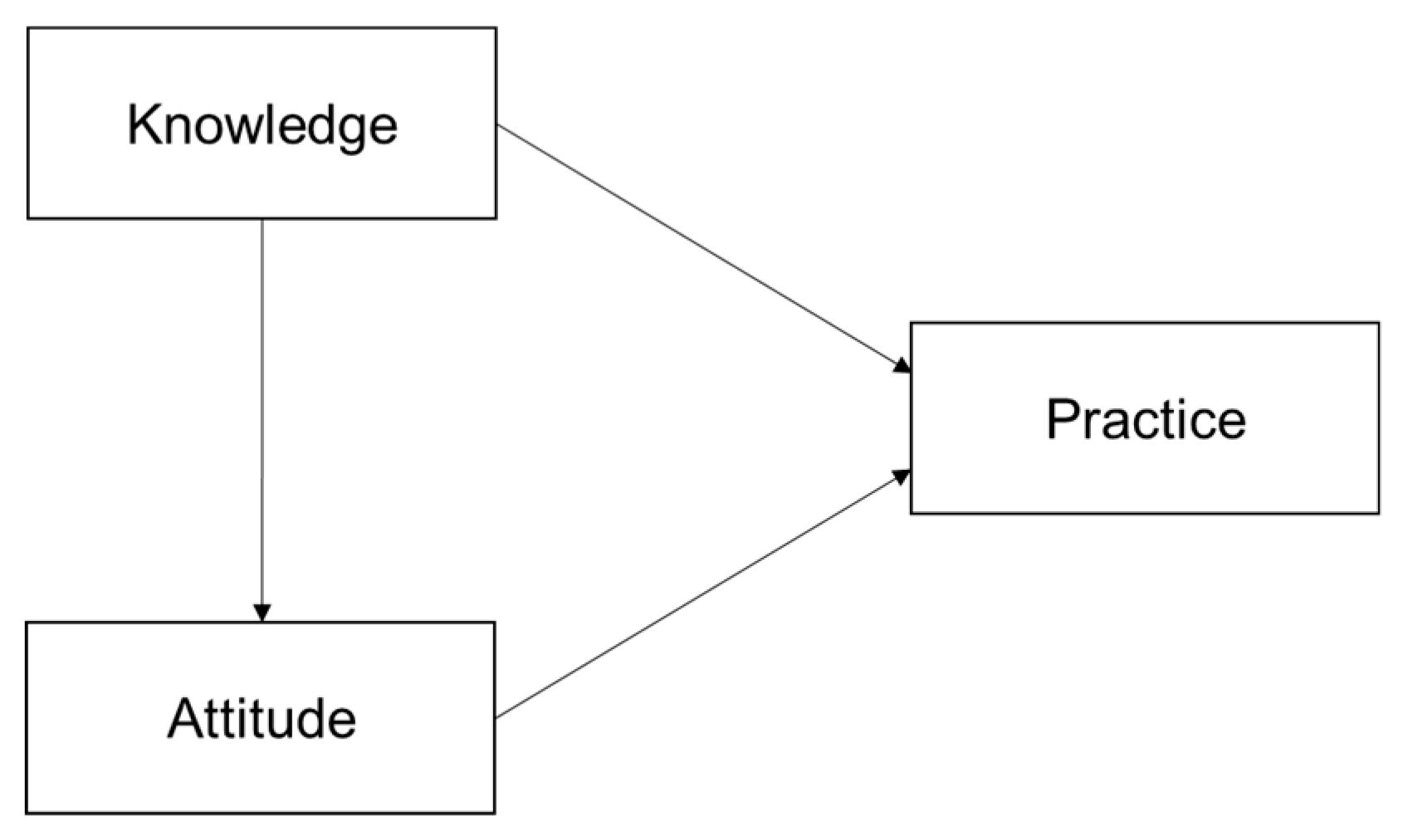
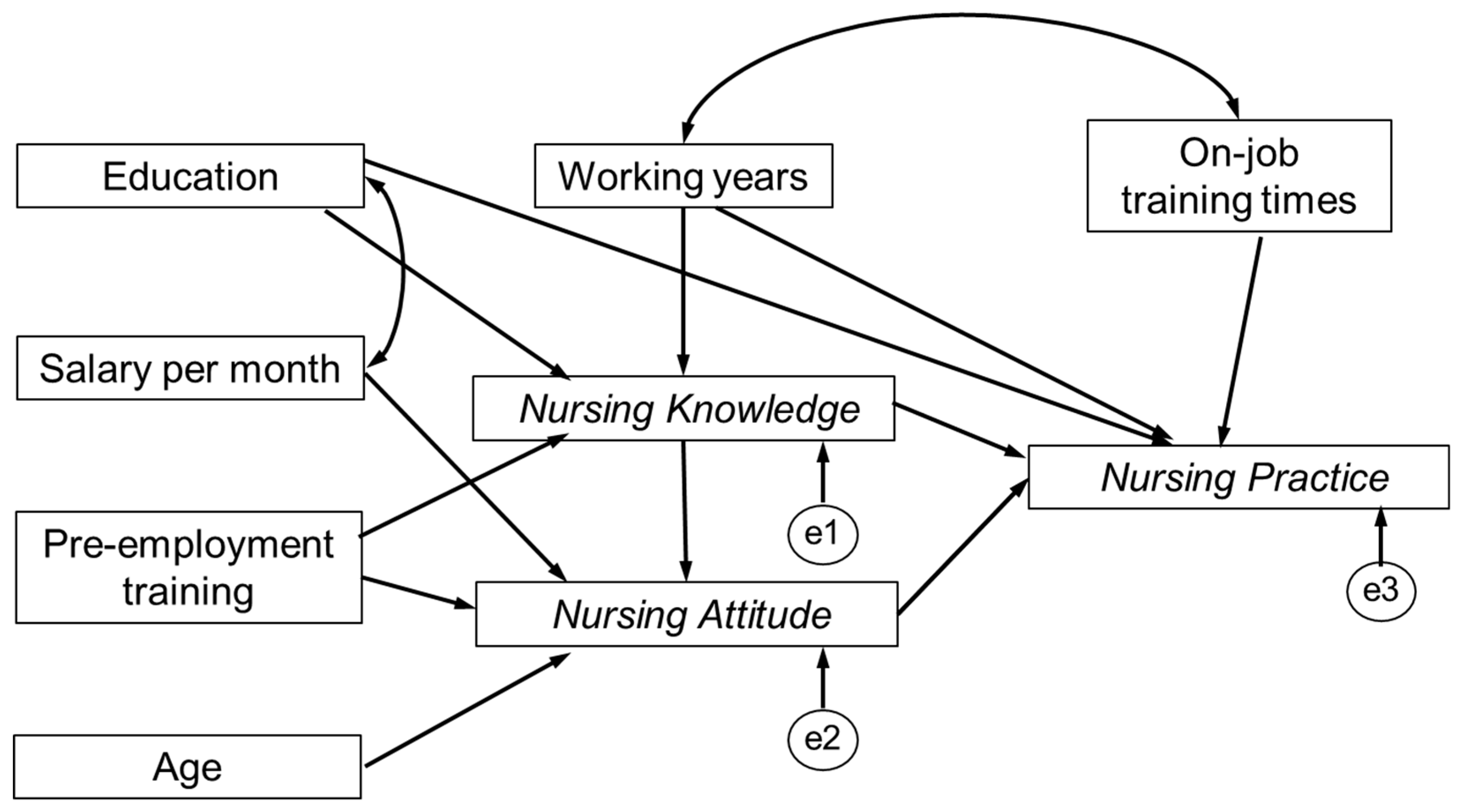
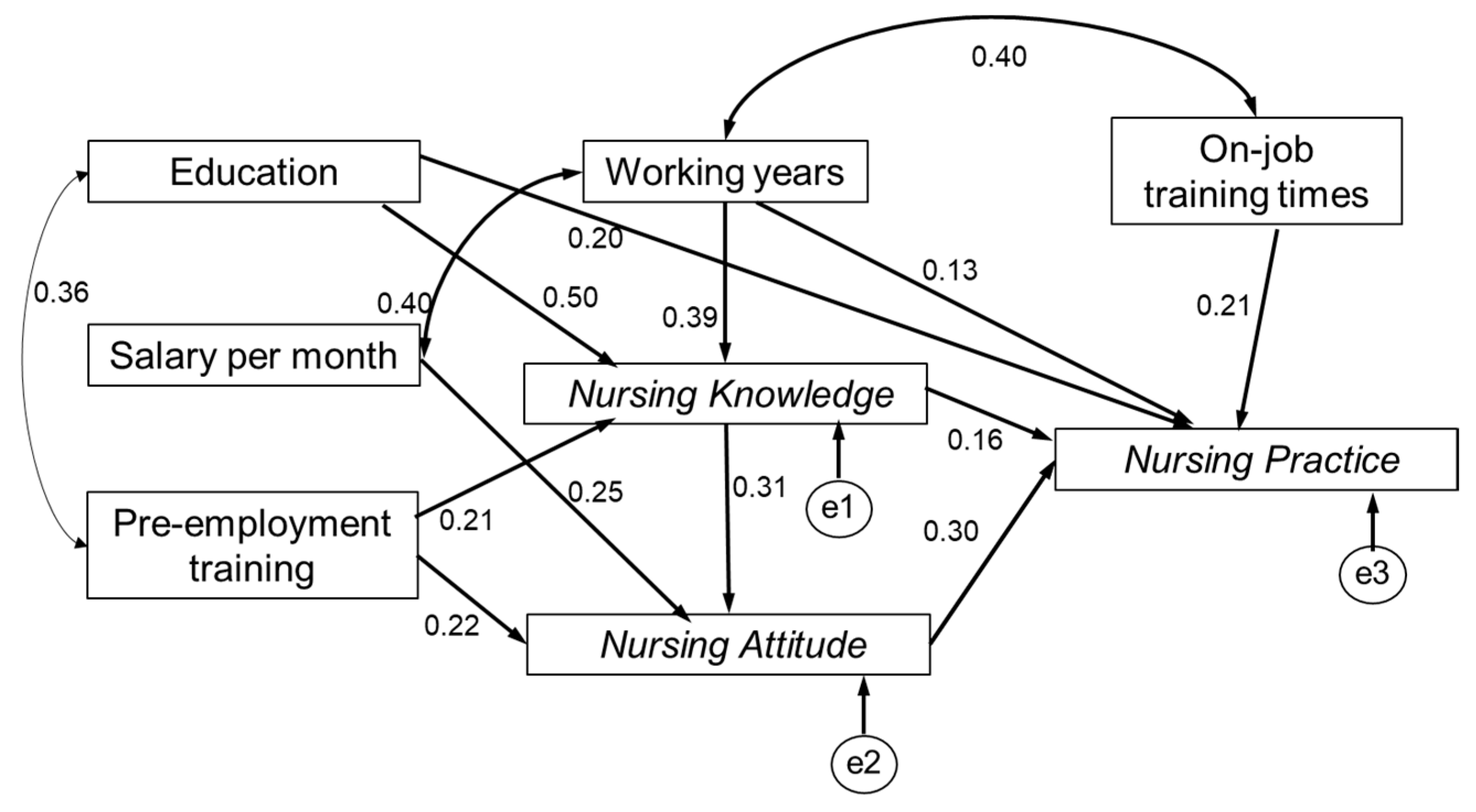
3.6. Pathways among Knowledge, Attitude and Practice
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fang, E.F.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.; Zhu, X.; Preedy, V.; Lu, H.; Bohr, V.A.; et al. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations, Department of Economic and Social Affairs. World Population Prospects: The 2017 Revision. Available online: https://esa.un.org/unpd/wpp/Download/Standard/Population/ (accessed on 20 December 2018).
- Wang, J.; Wu, B. Domestic helpers as frontline workers in China’s home-based elder care: A systematic review. J. Women Aging 2017, 29, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Gao, L.; Chen, S.; Dong, H. Care services for elderly people with dementia in rural China: A case study. Bull. World Health Organ. 2016, 94, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Zhan, H.J.; Feng, Z.; Chen, Z.; Feng, X. The role of the family in institutional long-term care: Cultural management of filial piety in China. Int. J. Soc. Welf. 2011, 20, S121–S134. [Google Scholar] [CrossRef]
- Chou, R.J. Willingness to live in eldercare institutions among older adults in urban and rural China: A nationwide study. Ageing Soc. 2010, 30, 583–608. [Google Scholar] [CrossRef]
- Feng, Z.; Zhan, H.J.; Feng, X.; Liu, C.; Sun, M.; Mor, V. An Industry in the Making: The Emergence of Institutional Elder Care in Urban China. J. Am. Geriatr. Soc. 2011, 59, 738–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Feng, Z.; Mor, V. Case-Mix and Quality Indicators in Chinese Elder Care Homes: Are There Differences Between Government-Owned and Private-Sector Facilities? J. Am. Geriatr. Soc. 2014, 62, 371–377. [Google Scholar] [CrossRef]
- Song, Y.; Scales, K.; Anderson, R.A.; Wu, B.; Corazzini, K.N. Resident challenges with daily life in Chinese long-term care facilities: A qualitative pilot study. Geriatr. Nurs. 2018, 39, 18–23. [Google Scholar] [CrossRef]
- Peng, R.; Wu, B. Changes of Health Status and Institutionalization among Older Adults in China. J. Aging Health 2015, 27, 1223–1246. [Google Scholar] [CrossRef]
- Feng, Z.; Liu, C.; Guan, X.; Mor, V. China’s Rapidly Aging Population Creates Policy Challenges in Shaping A Viable Long-Term Care System. Health Affair. 2012, 31, 2764–2773. [Google Scholar] [CrossRef]
- Ministry of Civil Affairs of the People’s Republic of China. China Civil Affairs Statistical Yearbook (2017); China Statistical Press: Beijing, China, 2017.
- Zhang, N.J.; Guo, M.; Zheng, X. China: Awakening giant developing solutions to population aging. Gerontologist 2012, 52, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Bharucha, A.J.; Pandav, R.; Shen, C.; Dodge, H.H.; Ganguli, M. Predictors of Nursing Facility Admission: A 12-Year Epidemiological Study in the United States. J. Am. Geriatr. Soc. 2004, 52, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Zhai, X.; Qiu, R.Z. Perceptions of long-term care, autonomy, and dignity, by residents, family and caregivers: The Beijing experience. J. Med. Philos. 2007, 32, 425–445. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Anderson, R.A.; Corazzini, K.N.; Wu, B. Staff characteristics and care in Chinese nursing homes: A systematic literature review. Int. J. Nurs. Sci. 2014, 1, 423–436. [Google Scholar] [CrossRef] [Green Version]
- Hao, Q.; Wu, S.; Ying, L.; Luo, L.; Dong, D.; Dong, B. Current Dilemmas of Nursing Homes in Chengdu: A Cross-Sectional Survey. J. Am. Med. Dir. Assoc. 2012, 13, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef]
- Stanton, B.F.; Clemens, J.D.; Aziz, K.M.; Rahman, M. Twenty-four-hour recall, knowledge-attitude-practice questionnaires, and direct observations of sanitary practices: A comparative study. Bull. World Health Organ. 1987, 65, 217–222. [Google Scholar]
- Engström, M.; Skytt, B.; Nilsson, A. Working life and stress symptoms among caregivers in elderly care with formal and no formal competence: Working life for caregivers with formal and no formal competence. J. Nurs. Manag. 2011, 19, 732–741. [Google Scholar] [CrossRef]
- Sloane, P.D.; Zimmerman, S.; Chen, X.; Barrick, A.L.; Poole, P.; Reed, D.; Mitchell, M.; Cohen, L.W. Effect of a person-centered mouth care intervention on care processes and outcomes in three nursing homes. J. Am. Geriatr. Soc. 2013, 61, 1158–1163. [Google Scholar] [CrossRef]
- Li, X.; Lu, L. Investigation and analysis the KABP of nursing staff on old-age care institutions. Unrs. Pract. Res. 2013, 10, 3–5. [Google Scholar]
- Lin, P.; Hsieh, M.; Lin, L. Hospital nurse knowledge of and approach to dementia care. J. Nurs. Res. 2012, 20, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y. Study of Quality of Life, Social Support, Knowledge, Attitude, Practice and Interventions of Senile Dementia Caregivers of Fujian Province; Fujian Medical University: Fuzhou, China, 2015. [Google Scholar]
- Ministry of Civil Affairs of the People’s Republic of China. National Occupational Standards for Old-Age Caregivers. Available online: http://jnjd.mca.gov.cn/article/zyjd/ylhly/201003/20100300063434.shtml (accessed on 4 Janary 2019).
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Soon, J.M. Food allergen knowledge, attitude and practices among UK consumers: A structural modelling approach. Food Res. Int. 2019, 120, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Ge, J.; Meng, H.; Chen, Z.; Liu, D. The Influence of Social Support and Care Burden on Depression among Caregivers of Patients with Severe Mental Illness in Rural Areas of Sichuan, China. Int. J. Environ. Res. Public Health 2019, 16, 1961. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Pang, B.; Chen, J.; Li, Y.; Xie, X. Assessing the Impact of Lifestyle Interventions on Diabetes Prevention in China: A Modeling Approach. Int. J. Environ. Res. Public Health 2019, 16, 1677. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Beaubien, J.M. Structural Equation Modeling with LISREL, PRELIS, and SIMPLIS: Basic Concepts, Applications, and Programming. Pers. Psychol. 1999, 52, 827. [Google Scholar]
- Chen, H.; Yang, H.; Song, P.; Wang, L. An Ambiguous Sense of Professional Identity: Community-Based Caregivers for Older Adults in China. Ageing Int. 2017, 42, 236–250. [Google Scholar] [CrossRef]
- Aggar, C. Caring burden. Aust. Nurs. J. 2012, 20, 35. [Google Scholar]
- Hasson, H.; Arnetz, J.E. Nursing staff competence, work strain, stress and satisfaction in elderly care: A comparison of home-based care and nursing homes. J. Clin. Nurs. 2008, 17, 468–481. [Google Scholar] [CrossRef]
- King, D.; Wei, Z.; Howe, A. Work satisfaction and intention to leave among direct care workers in community and residential aged care in Australia. J. Aging Soc. Policy 2013, 25, 301–319. [Google Scholar] [CrossRef] [PubMed]
- Bostick, J.E.; Rantz, M.J.; Flesner, M.K.; Riggs, C.J. Systematic review of studies of staffing and quality in nursing homes. J. Am. Med. Dir. Assoc. 2006, 7, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Tyler, D.A.; Jung, H.Y.; Feng, Z.; Mor, V. Prevalence of Nursing Assistant Training and Certification Programs Within Nursing Homes, 1997-2007. Gerontologist 2010, 50, 550–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, F.; Llena-Nozal, A.; Mercier, J.; Tjadens, F. Help wanted? Providing and paying for long-term care. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/social-issues-migration-health/help-wanted_9789264097759-en (accessed on 24 December 2018).
- Chan, T.; Luk, J.K.; Chu, L.; Chan, F.H. Low Education Level of Nursing Home Staff in Chinese Nursing Homes. J. Am. Med. Dir. Assoc. 2013, 14, 849–850. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Number |
|---|---|
| Sociodemographic | |
| Age | |
| <40 | 7 (8.3) |
| 40–49 | 21 (25.0) |
| 50–59 | 46 (54.8) |
| >60 | 10 (11.9) |
| Gender | |
| Male | 6 (7.1) |
| Female | 78 (92.9) |
| Residence | |
| Native | 74 (88.1) |
| Non-native | 10 (11.9) |
| Education | |
| Illiterate | 21 (25.0) |
| Primary school | 20 (23.8) |
| Middle school | 30 (35.7) |
| High school or higher | 13 (15.5) |
| Monthly salary (¥) | |
| ≤2500 | 11 (13.1) |
| 2501~3000 | 26 (31.0) |
| 3001~4000 | 45 (53.6) |
| 4001~5000 | 2 (2.4) |
| ≥5001 | 0 |
| Working situation | |
| Working years | |
| <1 year | 17 (20.2) |
| 1~3 years | 28 (33.3) |
| 3~5 years | 20 (23.8) |
| > 5 years | 19 (22.6) |
| Pre-employment training | |
| Yes | 29 (34.5) |
| No | 55 (65.5) |
| On-job training times | |
| 0 | 14 (16.7) |
| 1 | 7 (8.3) |
| 2~4 | 38 (45.2) |
| 5~8 | 18 (21.4) |
| >9 | 7 (8.4) |
| Average working hours per day | 14.96 ± 5.77 |
| Category | Question or Statement | Correct Response, n (%) |
|---|---|---|
| Diet | Do the elderly need adequate water between meals? | 81 (96.4) |
| It is better for the elderly to have more meals and eat less at every meal. | 75 (89.3) | |
| The elderly should drink lots of water quickly at once. | 78 (92.9) | |
| Dementia | The elderly with dementia would not exhibit consistent memory loss or forget their family members. | 21 (25.0) |
| The elderly with dementia would not exhibit incontinence. | 78 (92.9) | |
| The elderly with dementia would experience hallucinations in the early stage of the disease. | 54 (64.3) | |
| The elderly with dementia should not be allowed to walk around casually. | 37 (44.0) | |
| We should often communicate with the elderly with dementia to help alleviate their symptoms. | 80 (95.2) | |
| Diabetes | When the elderly with diabetes suffer from dizziness, fatigue and other conditions when they go out, we should immediately hold them steady to avoid them falling down. | 69 (82.1) |
| It is normal for the elderly with diabetes to suffer from dizziness and fatigue, we do not need to undertake any action. | 64 (76.2) | |
| We should do foot care for the elderly with diabetes every week to prevent foot complications. | 37 (44.0) | |
| Elderly with diabetes need no special treatment in terms of diet, just be consistent with other elderly people. | 33 (39.3) | |
| Chronic bronchitis | We should change the clothes of the elderly with chronic bronchitis according to the temperature to prevent the disease from getting worse. | 72 (85.7) |
| In the more severe smog weather, the elderly with chronic bronchitis should be urged to exercise normally and stay healthy. | 50 (59.5) | |
| High blood pressure | For the elderly with high blood pressure, they should remain seated for long periods. | 55 (65.5) |
| Do the elderly with high blood pressure need to avoid salty, spicy food in their diets? | 74 (88.1) | |
| For the elderly with high blood pressure, they should ensure reasonable rest time and appropriate physical exercise. | 79 (94.0) | |
| Bedsore | Bedsores occur mainly because of long-term bed rest. | 68 (81.0) |
| For the long-term bedridden elderly, they should be turned over every 2 h to observe whether their skin is red or not. | 79 (94.0) | |
| Medication | In the process of assisting the elderly to take medicine, they should be helped to a comfortable position and then given medicine. | 79 (94.0) |
| We can leave immediately after helping the elderly take medicine. | 62 (73.8) | |
| Psychological problems | It is normal for the elderly to have psychological problems, so no intervention is needed. | 32 (38.1) |
| We should properly communicate with the elderly for psychological care. | 80 (95.2) |
| Category | Question | Average Score (± SD) |
|---|---|---|
| Job satisfaction | Would you like to receive further knowledge and skills training? | 3.36 ± 0.93 |
| Are you satisfied with your current working hours? | 3.17 ± 0.69 | |
| Are you satisfied with your current salary? | 3.07 ± 0.77 | |
| Disease care | Are you confident that you can take care of the elderly with dementia? | 3.94 ± 0.39 |
| Are you confident that you can take care of the elderly with diabetes? | 3.78 ± 0.52 | |
| Are you confident that you can take care of the elderly with chronic bronchitis? | 3.92 ± 0.35 | |
| Are you confident that you can take care of the elderly with high blood pressure? | 4.00 ± 0.27 | |
| Are you confident that you can take care of bedridden elderly? | 3.92 ± 0.44 | |
| Do you think it is important to supervise the elderly to take their medicine on time? | 4.19 ± 0.42 | |
| Do you think that the psychological care of the elderly is important? | 4.12 ± 0.50 | |
| Job willingness | Do you care what other people think of your work in elderly care? | 3.36 ± 0.87 |
| Are you willing to work in elderly care for a long time? | 3.75 ± 0.58 | |
| Do you like the current work in elderly care? | 3.60 ± 0.58 |
| Question | Practice Rate, n (%) |
|---|---|
| Have you made any suggestions to the canteen in the nursing home about proper diets for the elderly? | 30 (35.7) |
| Do you often clean the living environment of the elderly? | 83 (98.8) |
| Are you concerned about the disease situation of the elderly? | 77 (91.7) |
| Do you often pay attention to the behavior and activity of the elderly? | 66 (78.6) |
| Have you supervised the elderly to take medicine on time? | 78 (92.9) |
| Have you paid attention to the emotional changes of the elderly? | 67 (79.8) |
| Do you often communicate with the elderly and provide psychological help? | 68 (81.0) |
| Variables | b | SE | b’ | p-Value |
|---|---|---|---|---|
| Knowledge | ||||
| Intercept | 9.305 | 1.081 | - | <0.001 |
| Education | 1.275 | 0.219 | 0.521 | <0.001 |
| Working years | 0.944 | 0.188 | 0.418 | <0.001 |
| Pre-employment training | 1.528 | 0.608 | 0.219 | 0.014 |
| R2 = 0.482 | ||||
| Attitude | ||||
| Intercept | 43.529 | 2.938 | - | <0.001 |
| Pre-employment training | 2.033 | 0.801 | 0.262 | 0.013 |
| Salary per month | 1.571 | 0.440 | 0.355 | 0.001 |
| Age | −0.090 | 0.045 | −0.211 | 0.048 |
| R2 = 0.262 | ||||
| Practice | ||||
| Intercept | 2.75 | 0.533 | - | <0.001 |
| On-job training times | 0.263 | 0.119 | 0.237 | 0.031 |
| Education | 0.358 | 0.097 | 0.361 | <0.001 |
| Working years | 0.266 | 0.101 | 0.290 | 0.010 |
| R2 = 0.279 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, Y.; Hu, X.; Li, Y.; Zhen, X.; Gu, Y.; Sun, X.; Dong, H. The Quality of Caregivers for the Elderly in Long-Term Care Institutions in Zhejiang Province, China. Int. J. Environ. Res. Public Health 2019, 16, 2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122164
Zeng Y, Hu X, Li Y, Zhen X, Gu Y, Sun X, Dong H. The Quality of Caregivers for the Elderly in Long-Term Care Institutions in Zhejiang Province, China. International Journal of Environmental Research and Public Health. 2019; 16(12):2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122164
Chicago/Turabian StyleZeng, Yuhang, Xiaoqian Hu, Yuanyuan Li, Xuemei Zhen, Yuxuan Gu, Xueshan Sun, and Hengjin Dong. 2019. "The Quality of Caregivers for the Elderly in Long-Term Care Institutions in Zhejiang Province, China" International Journal of Environmental Research and Public Health 16, no. 12: 2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16122164