Patterns of Diet, Physical Activity, Sitting and Sleep Are Associated with Socio-Demographic, Behavioural, and Health-Risk Indicators in Adults



Abstract
:1. Introduction
2. Methods
2.1. Health Behaviour Measures
2.2. Socio-Demographic, Behavioural, and Health-Risk Indicators
2.3. Statistical Analysis
3. Results
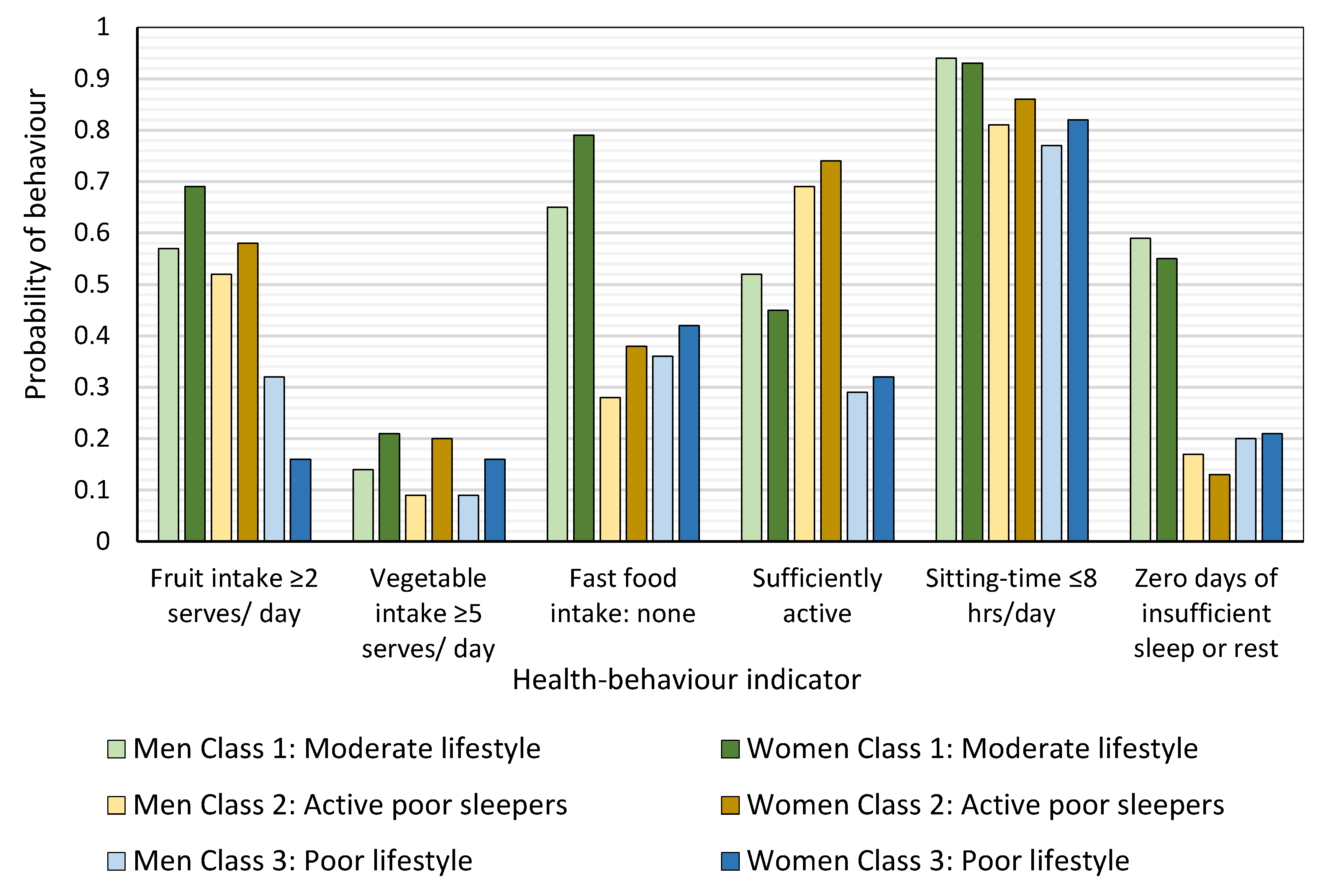
- The ‘moderate lifestyle’ class (43.2% of men and 38.1% of women) had the highest probability of eating ≥2 serves of fruit a day, not eating fast food, and reporting zero days of insufficient sleep or rest per month. They had the highest probability of consuming ≥5 serves of vegetables per day and the second highest probability of meeting physical activity recommendations;
- The ‘active poor sleepers’ class (37.0% of men and 31.4% of women) had the highest probability of meeting physical activity recommendations. Their fruit and vegetable intake was comparable to that of the ‘moderate lifestyle class’ but a third of men (33%) and a fifth of women (18%) ate fast food 2–7 times per week. They had the highest probability of 1–14 days of insufficient sleep or rest in the last month;
- The ‘poor lifestyle’ class (19.9% of men and 30.5% of women) had the highest probability of having no serves of fruit or vegetables per day and reporting 14–30 days of insufficient sleep or rest in the last month. Fast-food consumption frequency was similar to that of the ‘active poor sleepers’. This class was most likely to be insufficiently active or inactive.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical approval
References
- Ding, D.; Rogers, K.; van der Ploeg, H.; Stamatakis, E.; Bauman, A.E. Traditional and Emerging Lifestyle Risk Behaviors and All-Cause Mortality in Middle-Aged and Older Adults: Evidence from a Large Population-Based Australian Cohort. PLoS Med. 2015, 12, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P. Sleep patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Magee, C.A.; Reddy, P.; Robinson, L.; McGregor, A. Sleep quality subtypes and obesity. Health Psychol. 2016, 35, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Uzhova, I.; Woolhead, C.; Timon, C.; O’Sullivan, A.; Brennan, L.; Peñalvo, J.; Gibney, E. Generic Meal Patterns Identified by Latent Class Analysis: Insights from NANS (National Adult Nutrition Survey). Nutrients 2018, 10, 310. [Google Scholar] [CrossRef] [PubMed]
- O’Donovan, G.; Lee, I.; Hamer, M.; Stamatakis, E. Association of “weekend warrior” and other leisure time physical activity patterns with risks for all-cause, cardiovascular disease, and cancer mortality. JAMA Intern. Med. 2017, 177, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Oftedal, S.; Kolt, G.S.; Holliday, E.G.; Stamatakis, E.; Vandelanotte, C.; Brown, W.J.; Duncan, M.J. Associations of health-behavior patterns, mental health and self-rated health. Prev. Med. 2018, 118, 295–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Héroux, M.; Janssen, I.; Lee, D.C.; Sui, X.; Hebert, J.R.; Blair, S.N. Clustering of unhealthy behaviors in the aerobics center longitudinal study. Prev. Sci. 2012, 13, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Haapasalo, V.; de Vries, H.; Vandelanotte, C.; Rosenkranz, R.R.; Duncan, M.J. Cross-sectional associations between multiple lifestyle behaviours and excellent well-being in Australian adults. Prev. Med. 2018, 116, 119–125. [Google Scholar] [CrossRef]
- James, E.; Freund, M.; Booth, A.; Duncan, M.J.; Johnson, N.; Short, C.E.; Wolfenden, L.; Stacey, F.G.; Kay-Lambkin, F.; Vandelanotte, C. Comparative efficacy of simultaneous versus sequential multiple health behavior change interventions among adults: A systematic review of randomised trials. Prev. Med. 2016, 89, 211–223. [Google Scholar] [CrossRef]
- Cassidy, S.; Chau, J.Y.; Catt, M.; Bauman, A.; Trenell, M.I. Low physical activity, high television viewing and poor sleep duration cluster in overweight and obese adults; a cross-sectional study of 398,984 participants from the UK Biobank. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 57. [Google Scholar] [CrossRef]
- Rayward, A.T.; Duncan, M.J.; Brown, W.J.; Plotnikoff, R.C.; Burton, N.W. A cross-sectional cluster analysis of the combined association of physical activity and sleep with sociodemographic and health characteristics in mid-aged and older adults. Maturitas 2017, 102, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Vincent, G.E.; Jay, S.M.; Sargent, C.; Vandelanotte, C.; Ridgers, N.D.; Ferguson, S.A. Improving Cardiometabolic Health with Diet, Physical Activity, and Breaking Up Sitting: What about Sleep? Front. Physiol. 2017, 8, 865. [Google Scholar] [CrossRef] [PubMed]
- Vincent, G.E.; Jay, S.M.; Sargent, C.; Kovac, K.; Vandelanotte, C.; Ridgers, N.D.; Ferguson, S.A. The impact of breaking up prolonged sitting on glucose metabolism and cognitive function when sleep is restricted. Neurobiol. Sleep Circadian Rhythm. 2018, 4, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Kwan, Y.H.; Tan, C.S.; Thumboo, J.; Low, L.L. A systematic review of the clinical application of data-driven population segmentation analysis. BMC Med. Res. Methodol. 2018, 18, 121. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.; Vandelanotte, C.; Rayward, A.T.; Murawski, B.; Duncan, M.J. Sociodemographic and behavioral correlates of insufficient sleep in Australian adults. Sleep Health 2018, 5, 12–17. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Australian Institute of Health and Welfare. The Active Australia Survey: A Guide and Manual for Implementation, Analysis and Reporting; AIHW: Canberra, Australia, 2003. [Google Scholar]
- Rosenberg, D.E.; Bull, F.C.; Marshall, A.L.; Sallis, J.F.; Bauman, A.E. Assessment of sedentary behavior with the International Physical Activity Questionnaire. J. Phys. Act. Health 2008, 5, S30–S44. [Google Scholar] [CrossRef] [PubMed]
- van der Ploeg, H.P.; Chey, T.; Korda, R.J.; Banks, E.; Bauman, A. Sitting time and all-cause mortality risk in 222 497 Australian adults. Arch. Intern. Med. 2012, 172, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Jungquist, C.R.; Mund, J.; Aquilina, A.T.; Klingman, K.; Pender, J.; Ochs-Balcom, H.; van Wijngaarden, E.; Dickerson, S.S. Validation of the Behavioral Risk Factor Surveillance System Sleep Questions. J. Clin. Sleep Med. 2016, 12, 301–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Bureau of Statistics. Socio-Economic Indicator For Areas by Postal Aera Code (POA)–Index of Relative Socio-Economic Advantage and Disadvantage; Australian Bureasu of Statistics: Canberra, Australia, 2011. [Google Scholar]
- National Health and Medical Research Council. Australian Guidelines to Reduce Health Risk from Drinking Alcohol; National Health and Medical Research Council: Canberra, Australia, 2009; p. 179. [Google Scholar]
- Centers for Disease Control and Prevention. Measuring Healthy Days; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2000. [Google Scholar]
- Lanza, S.T.; Collins, L.M.; Lemmon, D.R.; Schafer, J.L. PROC LCA: A SAS Procedure for Latent Class Analysis. Struct. Equ. Model. Multidiscip. J. 2007, 14, 671–694. [Google Scholar] [CrossRef]
- Bray, B.C.; Lanza, S.T.; Tan, X. Eliminating Bias in Classify-Analyze Approaches for Latent Class Analysis. Struct. Equ. Model. Multidiscip. J. 2015, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Keeter, S.; Kennedy, C.; Dimock, M.; Best, J.; Craighill, P. Gauging the Impact of Growing Nonresponse on Estimates from a National RDD Telephone Survey. Int. J. Public Opin. Q. 2006, 70, 759–779. [Google Scholar] [CrossRef]
- Hendrie, G.; Noakes, M. Fruit, Vegetables and Diet Score; Commonwealth Scientific and Industrial Research Organisation: Canberra, Australia, 2017. [Google Scholar]
- Kino, S.; Bernabé, E.; Sabbah, W. Socioeconomic inequality in clusters of health-related behaviours in Europe: Latent class analysis of a cross-sectional European survey. BMC Public Health 2017, 17, 497. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Do, A.; Schmidt, H.-M.; Bauman, A.E. A Widening Gap? Changes in Multiple Lifestyle Risk Behaviours by Socioeconomic Status in New South Wales, Australia, 2002–2012. PLoS ONE 2015, 10, e0135338. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Adams, J.; Heywood, P. How and why do interventions that increase health overall widen inequalities within populations? In Health, Inequality and Society; Babones, S., Ed.; Policy Press: Bristol, UK, 2009. [Google Scholar]
- Conry, M.C.; Morgan, K.; Curry, P.; McGee, H.; Harrington, J.; Ward, M.; Shelley, E. The clustering of health behaviours in Ireland and their relationship with mental health, self-rated health and quality of life. BMC Public Health 2011, 11, 692. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Croft, J.B.; Wheaton, A.G.; Perry, G.S.; Chapman, D.P.; Strine, T.W.; McKnight-Eily, L.R.; Presley-Cantrell, L. Association between perceived insufficient sleep, frequent mental distress, obesity and chronic diseases among US adults, 2009 behavioral risk factor surveillance system. BMC Public Health 2013, 13, 84. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Fernandez-Mendoza, J.; Miksiewicz, T.; Kritikou, I.; Shaffer, M.L.; Liao, D.; Basta, M.; Bixler, E.O. Unveiling the Longitudinal Association between Short Sleep Duration and the Incidence of Obesity: The Penn State Cohort. Int. J. Obes. 2014, 38, 825–832. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia; NHMRC: Melbourne, Australia, 2013. [Google Scholar]
- Matheson, E.M.; King, D.E.; Everett, C.J. Healthy lifestyle habits and mortality in overweight and obese individuals. J. Am. Board Fam. Med. 2012, 25, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, A.C.; Wandell, P.E.; Gigante, B.; Leander, K.; Hellenius, M.L.; de Faire, U. Seven modifiable lifestyle factors predict reduced risk for ischemic cardiovascular disease and all-cause mortality regardless of body mass index: A cohort study. Int. J. Cardiol. 2013, 168, 946–952. [Google Scholar] [CrossRef]
- Balducci, S.; Zanuso, S.; Cardelli, P.; Salvi, L.; Mazzitelli, G.; Bazuro, A.; Iacobini, C.; Nicolucci, A.; Pugliese, G. Changes in physical fitness predict improvements in modifiable cardiovascular risk factors independently of body weight loss in subjects with type 2 diabetes participating in the Italian Diabetes and Exercise Study (IDES). Diabetes Care 2012, 35, 1347–1354. [Google Scholar] [CrossRef]
- Hillman, D.; Mitchell, S.; Streatfeild, J.; Burns, C.; Bruck, D.; Pezzullo, L. The economic cost of inadequate sleep. Sleep 2018, 41, 1–13. [Google Scholar] [CrossRef]
- Cheung, J.M.Y.; Bartlett, D.J.; Armour, C.L.; Glozier, N.; Saini, B. Insomnia Patients’ Help-Seeking Experiences. Behav. Sleep Med. 2014, 12, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Cunnington, D.; Junge, M.F.; Fernando, A.T. Insomnia: Prevalence, consequences and effective treatment. Med. J. Aust. 2013, 199, S36–S40. [Google Scholar] [CrossRef] [PubMed]
- Baffour, B.; Roselli, T.; Haynes, M.; Bon, J.J.; Western, M.; Clemens, S. Including mobile-only telephone users in a statewide preventive health survey—Differences in the prevalence of health risk factors and impact on trends. Prev. Med. Rep. 2017, 7, 91–98. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Male (n = 1640) | Female (n = 1734) | Total (n = 3374) | ||
|---|---|---|---|---|
| Mean (SD) | ||||
| Age | Years | 52.9 (18.2) | 53.2 (17.4) | 53.1 (17.8) |
| SEIFA decile | Out of 10 | 6.2 (2.8) | 6.1 (2.8) | 6.1 (2.8) |
| Mental distress | Days per last 30 days | 3.1 (7.2) | 3.8 (7.7) | 3.5 (7.5) |
| Count (%) | ||||
| Marital status | Partnered | 1129 (69.2) | 1114 (64.4) | 2243 (66.7) |
| Single, widowed, divorced | 503 (30.8) | 615 (35.6) | 1118 (33.3) | |
| Education | University | 732 (44.6) | 823 (47.5) | 1555 (46.1) |
| TAFE or trade college | 387 (23.6) | 353 (20.4) | 740 (21.9) | |
| Primary/Secondary | 521 (31.8) | 558 (32.2) | 1079 (32.0) | |
| Work status | Currently working | 1028 (62.7) | 954 (55.0) | 1982 (58.7) |
| Not in workforce/ retired | 612 (37.3) | 780 (45.0) | 1392 (41.3) | |
| Geographical location | City | 878 (53.5) | 875 (50.5) | 1753 (52.0) |
| Town | 349 (21.3) | 403 (23.2) | 752 (22.3) | |
| Rural | 413 (25.2) | 456 (26.3) | 869 (25.8) | |
| Smoking | Current smoker | 238 (14.5) | 212 (12.2) | 450 (13.3) |
| Non-smoker | 1402 (85.5) | 1522 (87.8) | 2924 (86.7) | |
| Alcohol | High risk drinking | 849 (51.8) | 799 (46.1) | 1648 (48.8) |
| Low risk drinking | 791 (48.2) | 935 (53.9) | 1726 (51.2) | |
| Body mass index a | <18.5 kg/m2 | 17 (1.0) | 50 (2.9) | 67 (2.0) |
| 18.5–24.9 kg/m2 | 541 (33.0) | 769 (44.4) | 1310 (38.8) | |
| 25.0–29.9 kg/m2 | 727 (44.3) | 491 (28.3) | 1218 (36.1) | |
| ≥30 kg/m2 | 355 (21.7) | 424 (24.5) | 779 (23.1) | |
| Fruit intake | None | 229 (14.0) | 196 (11.3) | 425 (12.6) |
| 1 serve/ day | 585 (35.7) | 549 (31.7) | 1134 (33.6) | |
| ≥2 serves/ day | 825 (50.3) | 989 (57.0) | 1814 (53.8) | |
| Vegetable intake | None | 47 (2.9) | 27 (1.6) | 74 (2.2) |
| 1–4 serves/ day | 1411 (86.1) | 1370 (79.1) | 2781 (82.5) | |
| ≥5 serves/ day | 181 (11.0) | 336 (19.4) | 517 (15.3) | |
| Fast food frequency | 2–7 times/week | 354 (21.6) | 205 (11.8) | 559 (16.6) |
| 1 times/week | 541 (33.0) | 572 (33.0) | 1113 (33.0) | |
| Never | 744 (45.4) | 956 (55.2) | 1700 (50.4) | |
| Physical activity level b | Inactive | 191 (11.7) | 218 (12.6) | 409 (12.2) |
| Insufficiently active | 559 (34.3) | 656 (38.0) | 1215 (36.2) | |
| Sufficiently active | 881 (54.0) | 853 (49.4) | 1734 (51.6) | |
| Sitting-time | >11 hrs/day | 70 (4.3) | 61 (3.5) | 131 (3.9) |
| 8–11 hrs/day | 166 (10.1) | 157 (9.1) | 323 (9.6) | |
| ≤8 hrs/day | 1404 (85.6) | 1516 (87.4) | 2920 (86.5) | |
| Insufficient sleep in last 30 days | 14–30 days | 358 (21.9) | 499 (28.8) | 857 (25.5) |
| 1–13 days | 697 (42.6) | 681 (39.3) | 1378 (40.9) | |
| None/ zero | 581 (35.5) | 551 (31.8) | 1132 (33.6) | |
| Men (n = 1640) | Women (n = 1734) | ||||||
|---|---|---|---|---|---|---|---|
| Moderate Lifestyle | Active Poor Sleepers | Poor Lifestyle | Moderate Lifestyle | Active Poor Sleepers | Poor Lifestyle | ||
| Latent class membership (%) | 43.2 | 37.0 | 19.9 | 38.1 | 31.4 | 30.5 | |
| Fruit intake | None | 0.07 | 0.09 | 0.40 | 0.06 | 0.05 | 0.23 |
| 1 serve/ day | 0.36 | 0.39 | 0.28 | 0.25 | 0.36 | 0.36 | |
| ≥2 serves/ day | 0.57 | 0.52 | 0.32 | 0.69 | 0.58 | 0.16 | |
| Vegetable intake | None | 0.01 | 0.01 | 0.12 | 0.00 | 0.00 | 0.05 |
| 1–4 serves/ day | 0.86 | 0.90 | 0.79 | 0.79 | 0.80 | 0.79 | |
| ≥5 serves/ day | 0.14 | 0.09 | 0.09 | 0.21 | 0.20 | 0.16 | |
| Fast food frequency | 2–7 times/week | 0.06 | 0.33 | 0.32 | 0.01 | 0.18 | 0.19 |
| 1 time/week | 0.28 | 0.39 | 0.32 | 0.20 | 0.45 | 0.39 | |
| Never | 0.65 | 0.28 | 0.36 | 0.79 | 0.38 | 0.42 | |
| Physical activity level | Inactive | 0.13 | 0.03 | 0.28 | 0.13 | 0.01 | 0.24 |
| Insufficiently active | 0.36 | 0.28 | 0.43 | 0.43 | 0.25 | 0.44 | |
| Sufficiently active | 0.52 | 0.69 | 0.29 | 0.45 | 0.74 | 0.32 | |
| Sitting-time | >11 hrs/day | 0.02 | 0.04 | 0.10 | 0.02 | 0.01 | 0.08 |
| 8–11 hrs/day | 0.04 | 0.15 | 0.14 | 0.13 | 0.13 | 0.10 | |
| ≤8 hrs/day | 0.94 | 0.81 | 0.77 | 0.93 | 0.86 | 0.82 | |
| Insufficient sleep or rest in last 30 days | 14–30 days | 0.11 | 0.19 | 0.54 | 0.11 | 0.27 | 0.53 |
| 1–13 days | 0.30 | 0.64 | 0.26 | 0.24 | 0.60 | 0.25 | |
| None/zero | 0.59 | 0.17 | 0.20 | 0.55 | 0.13 | 0.21 | |
| Men (n = 1644) | Women (n = 1737) | |||||
|---|---|---|---|---|---|---|
| Moderate Lifestyle OR (95%CI) | Active Poor Sleepers OR (95%CI) | Poor Lifestyle OR (95%CI) | Moderate LifestyleOR (95%CI) | Active Poor SleepersOR (95%CI) | Poor Lifestyle OR (95%CI) | |
| Age a | Ref | 0.88 (0.85–0.91) | 0.92 (0.89–0.96) | Ref | 0.88 (0.84–0.91) | 0.88 (0.85–0.92) |
| Single, widowed or divorced b | Ref | 1.31 (0.55–3.13) | 2.13 (1.06–4.29) | Ref | 1.84 (0.81–4.20) | 1.67 (0.78–3.61) |
| Primary or secondary school education only c | Ref | 0.57 (0.25–1.35) | 1.88 (0.84–4.20) | Ref | 0.84 (0.33–2.12) | 2.98 (1.29–6.88) |
| TAFE or trade college education c | Ref | 0.80 (0.32–1.99) | 1.95 (0.87–4.37) | Ref | 0.95 (0.38–2.39) | 2.01 (0.84–4.81) |
| Retired or not in workforce d | Ref | 0.37 (0.13–1.05) | 1.00 (0.48–2.08) | Ref | 0.37 (0.16–0.91) | 0.76 (0.36–1.59) |
| SEIFA score (z-score) e | Ref | 1.23 (0.83–1.84) | 0.91 (0.64–1.30) | Ref | 1.14 (0.77–1.70) | 0.70 (0.49–0.99) |
| Geographic location: town f | Ref | 0.57 (0.22–1.42) | 0.57 (0.26–1.26) | Ref | 1.13 (0.48–2.64) | 0.84 (0.37–1.89) |
| Geographic location: rural f | Ref | 0.81 (0.33–1.97) | 0.65 (0.29–1.47) | Ref | 0.67 (0.27–1.69) | 0.76 (0.33–1.77) |
| Current smoker g | Ref | 0.83 (0.29–2.38) | 5.12 (2.15–12.19) | Ref | 0.90 (0.29–2.73) | 3.46 (1.22–9.78) |
| High-risk alcohol consumption h | Ref | 1.45 (0.67–3.17) | 0.87 (0.45–1.67) | Ref | 1.42 (0.70–2.88) | 0.90 (0.46–1.75) |
| BMI 25–29.9 kg/m2 i | Ref | 1.19 (0.52–2.66) | 1.41 (0.63–3.14) | Ref | 1.54 (0.68–3.48) | 2.61 (1.11–6.16) |
| BMI ≥ 30 kg/m2 i | Ref | 0.66 (0.21–2.01) | 4.81 (1.91–12.12) | Ref | 1.21 (0.43–3.41) | 8.16 (3.38–19.69) |
| Frequency of mental health distress (z-score) j | Ref | 2.43 (0.76–7.72) | 4.73 (1.49–15.05) | Ref | 8.29 (1.86–36.84) | 11.88 (2.69–46.69) |
| Men | Women | |||||
|---|---|---|---|---|---|---|
| Moderate Lifestyle (n = 726) | Active Poor Sleepers (n = 614) | Poor Lifestyle (n = 292) | Moderate Lifestyle (n = 687) | Active Poor Sleepers (n = 540) | Poor Lifestyle (n = 502) | |
| Age, mean (SD) | 67.1 (10.2) | 37.0 (12.8) | 51.2 (14.2) | 67.2 (10.4) | 39.3 (12.9) | 49.2 (14.8) |
| Mental distress, mean (SD) | 0.6 (2.3) | 2.7 (5.6) | 10.5 (12.0) | 0.5 (1.6) | 3.3 (5.9) | 8.8 (11.1) |
| SEIFA decile, mean (SD) | 5.8 (2.7) | 6.9 (2.7) | 5.5 (2.7) | 6.0 (2.8) | 7.1 (2.6) | 5.1 (2.7) |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Marital status | ||||||
| Married or de-factor | 580 (51.4) | 390 (34.5) | 159 (14.1) | 476 (42.7) | 330 (29.6) | 308 (27.7) |
| Single, divorced, widowed | 146 (28.0) | 224 (44.5) | 133 (26.4) | 210 (34.2) | 210 (34.3) | 194 (31.5) |
| Education | ||||||
| Primary or secondary school | 296 (56.8) | 99 (19.0) | 126 (24.2) | 277 (49.6) | 57 (10.2) | 224 (40.1) |
| TAFE or trade college | 168 (43.4) | 118 (30.5) | 101 (26.1) | 147 (41.6) | 75 (21.3) | 131 (37.1) |
| University degree | 266 (36.4) | 400 (54.9) | 66 (9.0) | 265 (32.2) | 409 (49.7) | 149 (18.1) |
| Geographical location | ||||||
| City | 333 (37.9) | 395 (45.0) | 150 (17.1) | 327 (37.4) | 330 (37.7) | 218 (24.9) |
| Town | 168 (48.1) | 114 (32.7) | 67 (19.2) | 162 (40.2) | 121 (30.0) | 120 (29.8) |
| Rural | 229 (55.9) | 108 (26.2) | 76 (18.4) | 200 (43.9) | 90 (19.7) | 166 (36.4) |
| Smoking status | ||||||
| Non-smoker | 679 (48.4) | 543 (38.7) | 180 (12.8) | 651 (42.8) | 510 (33.5) | 361 (23.7) |
| Current smoker | 51 (21.4) | 74 (31.1) | 113 (47.5) | 38 (17.9) | 31 (14.6) | 143 (67.5) |
| Alcohol use | ||||||
| Low risk alcohol use | 358 (45.3) | 278 (35.2) | 155 (19.6) | 392 (41.9) | 237 (25.4) | 306 (32.7) |
| High risk alcohol use | 372 (43.8) | 339 (39.9) | 138 (16.3) | 297 (37.2) | 304 (38.1) | 198 (24.8) |
| BMI category | ||||||
| <18.5 kg/m2 | 6 (35.3) | 8 (47.1) | 3 (17.7) | 20 (40.0) | 23 (46.0) | 7 (14.0) |
| 18.5–25 kg/m2 | 206 (38.0) | 269 (49.7) | 66 (12.2) | 301 (39.1) | 335 (43.6) | 133 (17.3) |
| 25.0–29.9 kg/m2 | 368 (50.6) | 266 (36.6) | 93 (12.8) | 229 (46.6) | 135 (27.5) | 127 (25.9) |
| ≥30 kg/m2 | 150 (42.3) | 74 (20.9) | 131 (36.9) | 139 (32.8) | 48 (11.3) | 237 (55.9) |
| Mental distress (in last 30 days) | ||||||
| None/zero | 638 (57.1) | 361 (32.3) | 119 (10.6) | 573 (55.3) | 263 (25.4) | 201 (19.4) |
| 1–13 days | 87 (23.5) | 220 (59.3) | 64 (17.3) | 115 (22.0) | 244 (46.6) | 165 (31.5) |
| 14–30 days | 5 (3.3) | 36 (23.8) | 110 (72.9) | 1 (0.6) | 34 (19.7) | 138 (79.8) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oftedal, S.; Vandelanotte, C.; Duncan, M.J. Patterns of Diet, Physical Activity, Sitting and Sleep Are Associated with Socio-Demographic, Behavioural, and Health-Risk Indicators in Adults. Int. J. Environ. Res. Public Health 2019, 16, 2375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132375
Oftedal S, Vandelanotte C, Duncan MJ. Patterns of Diet, Physical Activity, Sitting and Sleep Are Associated with Socio-Demographic, Behavioural, and Health-Risk Indicators in Adults. International Journal of Environmental Research and Public Health. 2019; 16(13):2375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132375
Chicago/Turabian StyleOftedal, Stina, Corneel Vandelanotte, and Mitch J. Duncan. 2019. "Patterns of Diet, Physical Activity, Sitting and Sleep Are Associated with Socio-Demographic, Behavioural, and Health-Risk Indicators in Adults" International Journal of Environmental Research and Public Health 16, no. 13: 2375. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132375