Acute and Cumulative Effects of Haze Fine Particles on Mortality and the Seasonal Characteristics in Beijing, China, 2005–2013: A Time-Stratified Case-Crossover Study


Abstract
:1. Introduction
2. Materials and Methods
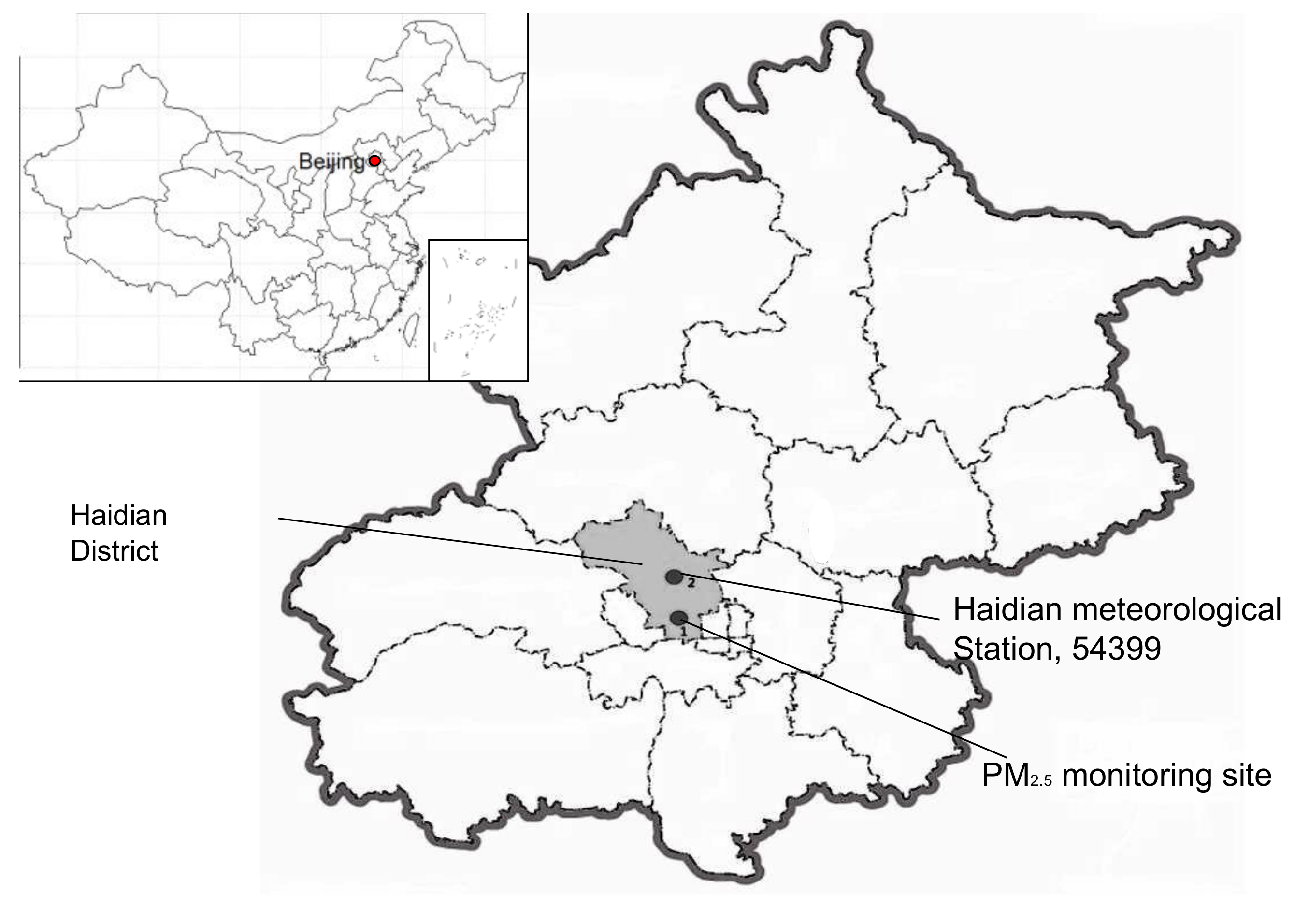
2.1. Study Area
2.2. Data Collection
2.3. Statistical Methods
2.4. Sensitivity Analysis
3. Results
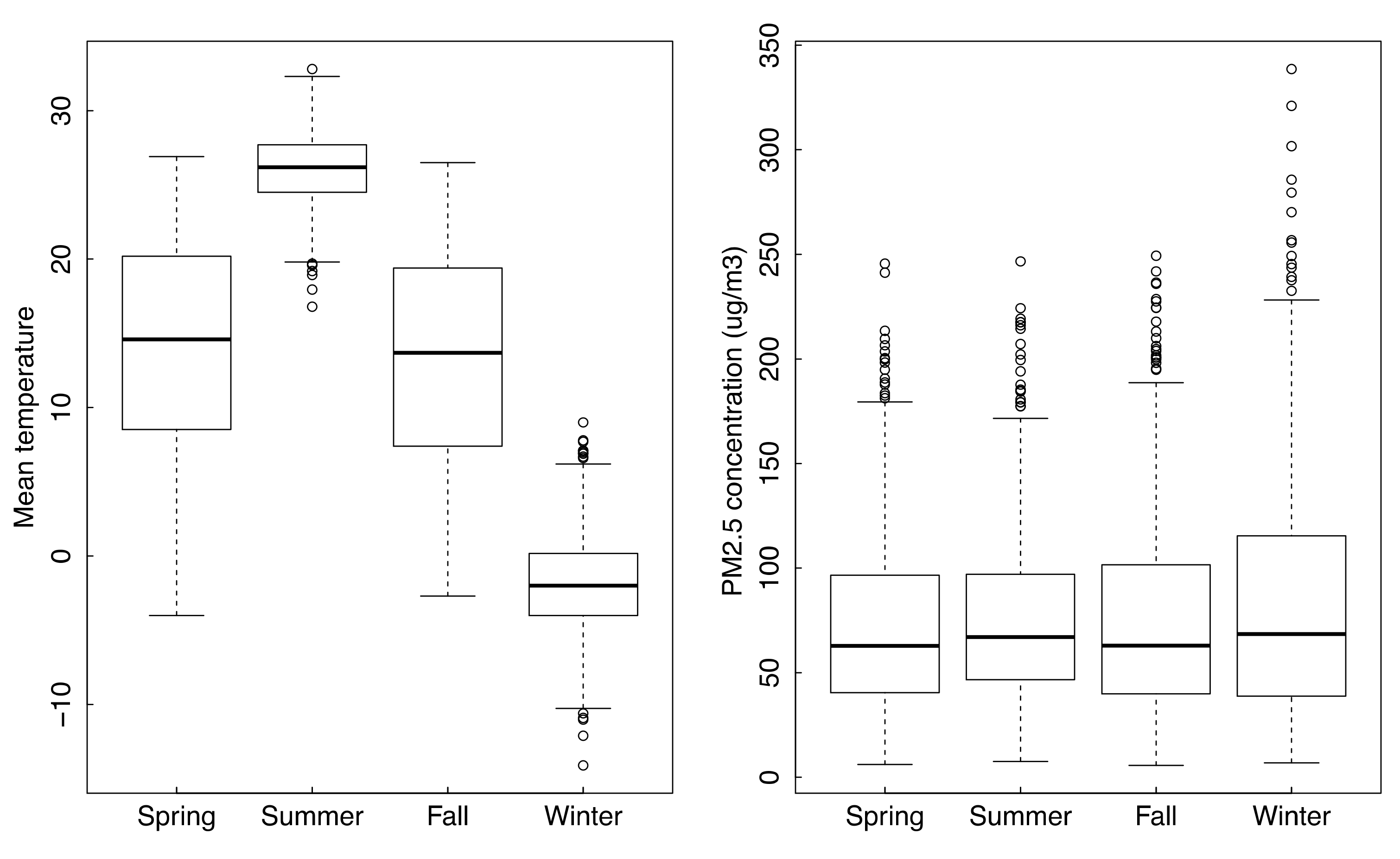
3.1. Descriptive Statistics of Data
3.2. Estimated Effects of PM2.5
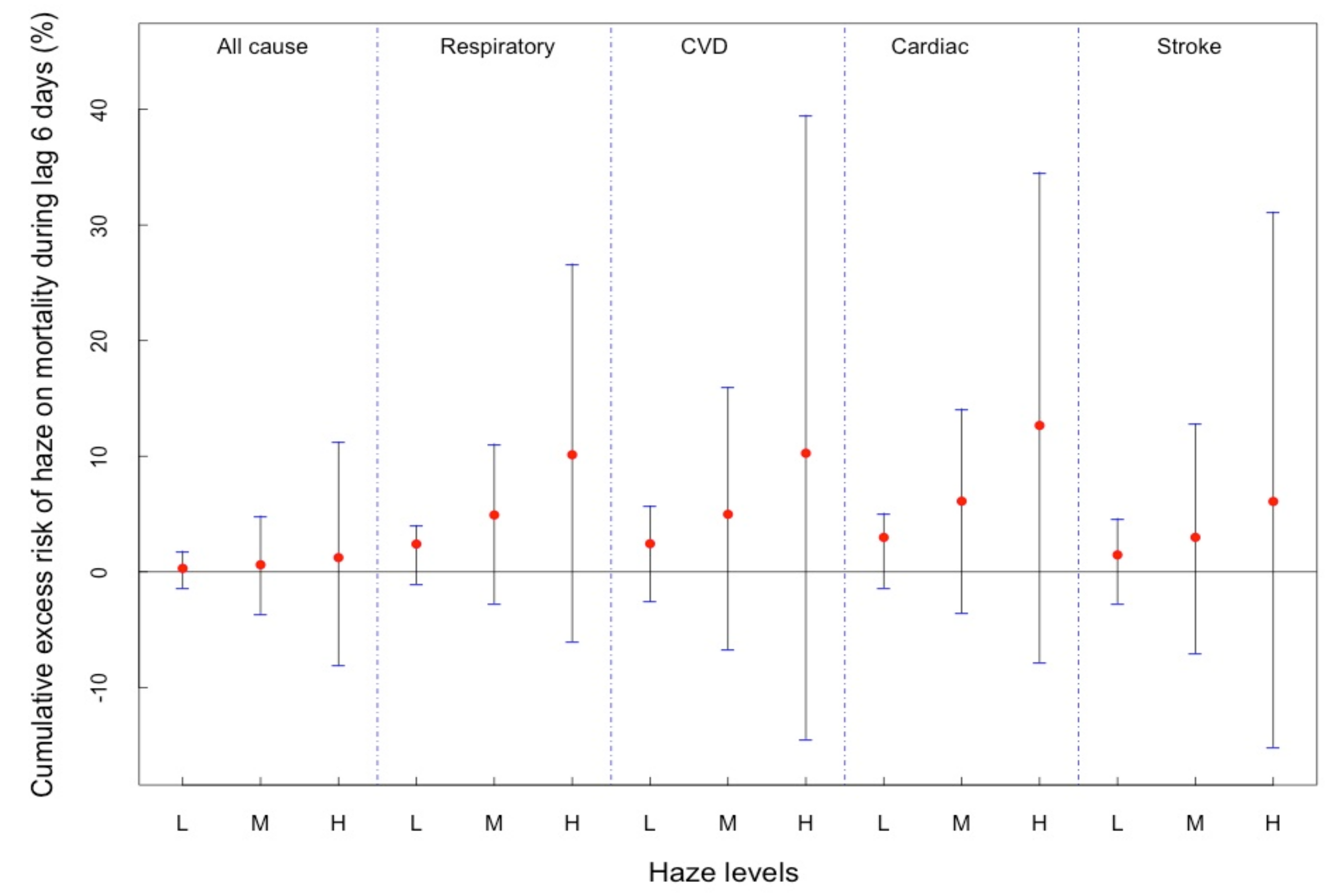
3.3. Cumulative Effects
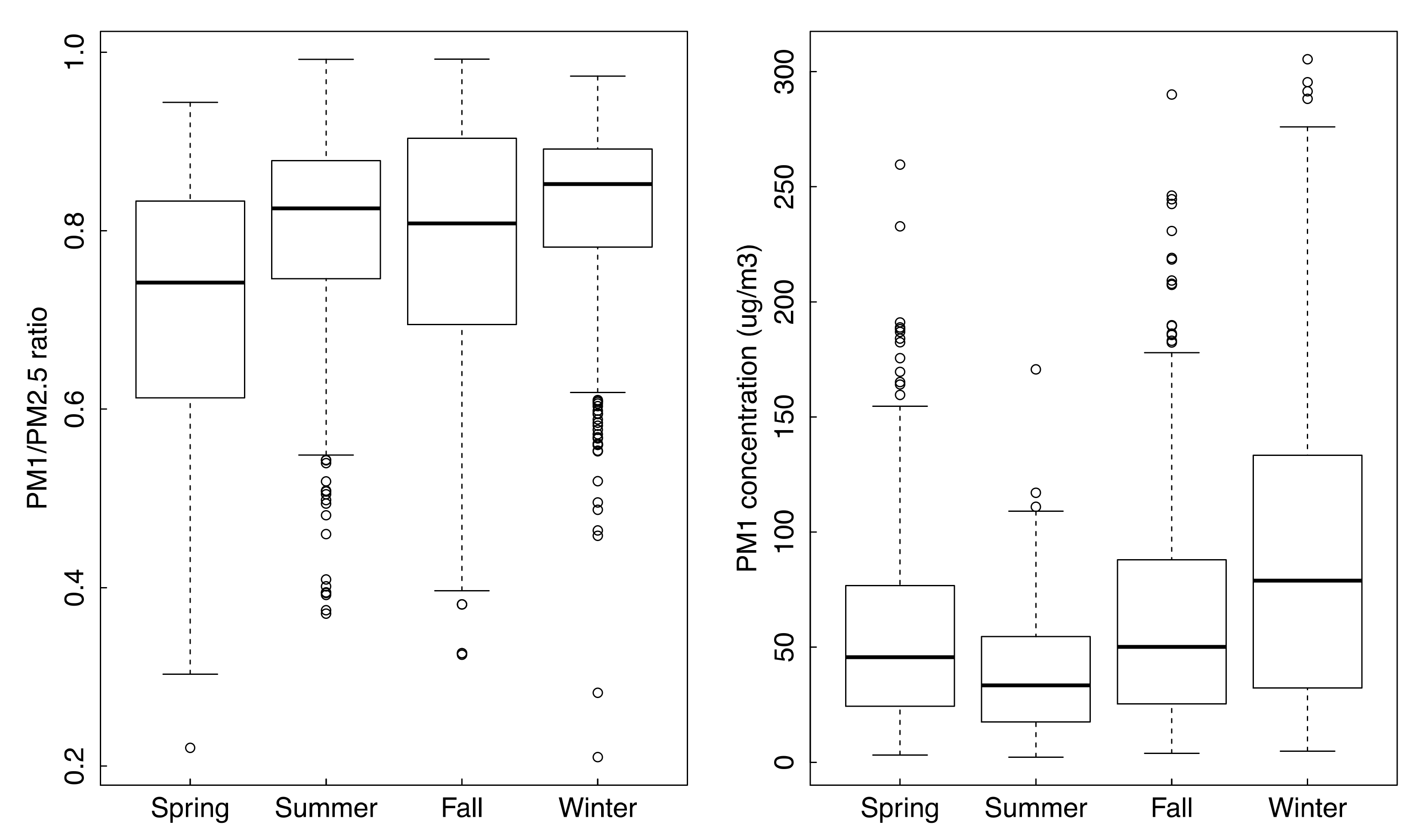
3.4. Seasonal Characteristics of PM2.5
3.5. Direct Effects of Temperature
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yang, W.; Li, L. Efficiency evaluation of industrial waste gas control in China: A study based on data envelopment analysis (DEA) model. J. Clean. Prod. 2018, 179, 1–11. [Google Scholar] [CrossRef]
- Su, C.; Hampel, R.; Franck, U.; Wiedensohler, A.; Cyrys, J.; Pan, X.; Wichmann, H.; Peters, A.; Schneider, A.; Breitner, S. Spatio-temporal variation of haze days and atmospheric circulation pattern in China (1961–2013). Quat. Int. 2015, 380, 14–21. [Google Scholar] [CrossRef]
- Tao, M.; Chen, L.; Wang, Z.; Ma, P.; Tao, J.; Jia, S. A study of urban pollution and haze clouds over northern China during the dusty season based on satellite and surface observations. Atmos. Environ. 2014, 82, 183–192. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, L.; Wang, W.; Cao, D.; Wang, X.; Ye, D. Long-term trend and spatiotemporal variations of haze over China by satellite observations from 1979 to 2013. Atmos. Environ. 2015, 119, 362–373. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, W. Does Whistleblowing Work for Air Pollution Control in China? A Study Based on Three-party Evolutionary Game Model under Incomplete Information. Sustainablility 2019, 11, 324. [Google Scholar] [CrossRef]
- Thondoo, M.; Rojas-Rueda, D.; Gupta, J.; De Vries, D.H.; Nieuwenhuijsen, M.J. Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries. Int. J. Environ. Res. Public Health. 2019, 16, 11. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Guttikunda, S.K.; Carmichael, G.R.; Wang, Y.; Liu, Z.; Stanier, C.O.; Saide, P.E.; Yu, M. Health impacts and economic losses assessment of the 2013 severe haze event in Beijing area. Sci. Total Environ. 2015, 511, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhang, Y.H.; Xu, Y.J.; Lin, H.L.; Xu, X.J.; Luo, Y.; Xiao, J.; Zeng, W.L.; Zhang, W.F.; Chu, C.; et al. The effects of dust–haze on mortality are modified by seasons and individual characteristics in Guangzhou, China. Environ. Pollut. 2014, 187, 116–123. [Google Scholar] [CrossRef]
- Chen, R.; Zhang, Y.; Yang, C.; Zhao, Z.; Xu, X.; Kan, H. Acute Effect of Ambient Air Pollution on Stroke Mortality in the China Air Pollution and Health Effects Study. Stroke 2013, 44, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Su, C.; Hampel, R.; Franck, U.; Wiedensohler, A.; Cyrys, J.; Pan, X.; Wichmann, H.-E.; Peters, A.; Schneider, A.; Breitner, S. Assessing responses of cardiovascular mortality to particulate matter air pollution for pre-, during- and post-2008 Olympics periods. Environ. Res. 2015, 142, 112–122. [Google Scholar] [CrossRef]
- Yang, Y.; Li, R.; Li, W.; Wang, M.; Cao, Y.; Wu, Z.; Xu, Q. The Association between Ambient Air Pollution and Daily Mortality in Beijing after the 2008 Olympics: A Time Series Study. PLoS ONE 2013, 8, e76759. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, Y.; Li, G.; Zhou, J.; Jin, X.; Wang, W.; Pan, X. The spatial characteristics of ambientparticulate matter and daily mortality in the urban area of Beijing, China. Sci. Total Environ. 2012, 435, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ma, Z.; Zheng, C.; Shang, Y. Ambient temperature enhanced acute cardiovascular-respiratory mortality effects of PM2.5 in Beijing, China. Int. J. Biometeorol. 2015, 59, 1761–1770. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wu, Y.; Gu, B. Characterization of haze episodes and factors contributing to their formation using a panel model. Chemosphere 2016, 149, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Stylianou, M.; Nicolich, M.J. Cumulative effects and threshold levels in air pollution mortality: Data analysis of nine la rge US cities using the NMMAPS dataset. Environ. Pollut. 2009, 157, 2216–2223. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Negri, E.; Gallus, S.; Boffetta, P.; Tramacere, I.; La Vecchia, C. Long-term particulate matter exposure and mortality: A review of European epidemiological studies. BMC Public Health 2009, 9, 453. [Google Scholar] [CrossRef] [PubMed]
- Janes, H.; Dominici, F.; Zeger, S.L. Trends in air pollution and mortality—An approach to the assessment of unmeasured confounding. Epidemiology 2007, 18, 416–423. [Google Scholar] [CrossRef]
- Alperovitch, A.; Lacombe, J.; Hanon, O.; Dartigures, J.F.; Ritchie, K.; Ducimetiere, P.; Tzourio, C. Relationship Between Blood Pressure and Outdoor Temperature in a Large Sample of Elderly Individuals the Three-City Study. Arch. Int. Med. 2009, 169, 75–80. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 2 July 2018).
- Barnett, A.G.; Baker, P.; Dobson, A.J. Analysing Seasonal Data. Available online: https://journal.r-project.org/archive/2012/RJ-2012-001/RJ-2012-001.pdf (accessed on 30 June 2012).
- Barnett, A.G.; Dobson, A.J. Analyzing Seasonal Data; Springer: Berlin, Germany, 2010. [Google Scholar]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1. [Google Scholar] [CrossRef]
- Qian, Z.; He, Q.; Lin, H.-M.; Kong, L.; Bentley, C.M.; Liu, W.; Zhou, D. High Temperatures Enhanced Acute Mortality Effects of Ambient Particle Pollution in the “Oven” City of Wuhan, China. Environ. Health Perspect. 2008, 116, 1172–1178. [Google Scholar] [CrossRef]
- Meng, X.; Zhang, Y.; Zhao, Z.; Duan, X.; Xu, X.; Kan, H. Temperature modifies the acute effect of particulate air pollution on mortality in eight Chinese cities. Sci. Total Environ. 2012, 435, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Samet, J.M.; Zeger, S.L. Combining evidence on air pollution and daily mortality from the 20 largest US cities: a hierarchical modelling strategy. J. R. Stat. Soc. Ser. A (Stat. Soc.) 2000, 163, 263–302. [Google Scholar] [CrossRef]
- Xu, W.; Chen, H.; Li, D.; Zhao, F.; Yang, Y. A Case Study of Aerosol Characteristics During a Haze Episode Over Beijing. Procedia Environ. Sci. 2013, 18, 404–411. [Google Scholar] [CrossRef] [Green Version]
- Sun, Z.; Mu, Y.; Liu, Y.; Shao, L. A comparison study on airborne particles during haze days and non-haze days in Beijing. Sci. Total Environ. 2013, 456, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Liu, X.; Gu, J.; Li, Y.; Qu, Y.; An, J.; Wang, J.; Zhang, Y.; Hu, M.; Zhang, F. Chemical characterization of size-resolved aerosols in four seasons and hazy days in the megacity Beijing of China. J. Environ. Sci. 2015, 32, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, G.; Ren, Y.; Wang, J.; Wu, C.; Han, Y.; Zhang, L.; Cheng, C.; Meng, J. Identification of chemical compositions and sources of atmospheric aerosols in Xi’an, inland China during two types of haze events. Sci. Total Environ. 2016, 566, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Y.; Yan, C.; Patterson, R.F.; Zhu, Y.; Yao, X.; Zhu, Y.; Ma, S.; Qiu, X.; Zhu, T.; Zheng, M. Modeled deposition of fine particles in human airway in Beijing, China. Atmos. Environ. 2016, 124, 387–395. [Google Scholar] [CrossRef]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung Cancer, Cardiopulmonary Mortality, and Long-term Exposure to Fine Particulate Air Pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Yang, H.; Guo, S.; Wang, Z.; Xu, X.; Duan, X.; Kan, H. Alternative ozone metrics and daily mortality in Suzhou: The China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2012, 426, 83–89. [Google Scholar] [CrossRef]
- Goldberg, M.S.; Burnett, R.T.; Yale, Y.J.; Valois, M.F.; Brook, J.R. The association between daily mortality and ambient air particle pollution in Montreal, Quebec 1. Nonaccidental mortality. Environ. Res. 2001, 86, 12–25. [Google Scholar] [CrossRef]
- Jaenicke, R. Abundance of Cellular Material and Proteins in the Atmosphere. Science 2005, 308, 73. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Jiang, W.; Wang, B.; Fang, J.; Lang, J.; Tian, G.; Jiang, J.; Zhu, T.F. Inhalable Microorganisms in Beijing’s PM2.5 and PM10 Pollutants during a Severe Smog Event. Environ. Sci. Technol. 2014, 48, 1499–1507. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Z.; Xin, J.; Zheng, H.; Meng, X.; Wang, X. Species composition, distribution and phonological characters of pollen-allergenic plants in Beijing urban area. Chin. J. Appl. Ecol. 2007, 18, 1953–1958. (In Chinese) [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | Minimum | 25th | 50th | 75th | Max |
|---|---|---|---|---|---|---|
| PM2.5 (µg/m3) | 78.01 | 20.02 | 42.6 | 65.94 | 103 | 301.7 |
| Temperature (°C) | 12.93 | −14.1 | 2 | 14.3 | 23.5 | 32.8 |
| Relative humidity | 55.5 | 7 | 39 | 57 | 71.75 | 100 |
| Respiratory diseases | 2.47 | 0 | 1 | 2 | 3 | 11 |
| Endocrine and metabolic | 1.49 | 1 | 1 | 4.27 | 2 | 9 |
| Cardiovascular diseases | 9.58 | 1 | 7 | 9 | 12 | 24 |
| Genitourinary | 1.14 | 1 | 1 | 1 | 1 | 4 |
| Total death | 21.64 | 4 | 17 | 21 | 26 | 49 |
| Season | All-Cause | Cardiovascular | Respiratory | Cardiac | Stroke | |
|---|---|---|---|---|---|---|
| Whole year Spring | lag 0 | 1.005 (1.001, 1.008) ** | 1.006 (1.002, 1.010) ** | 0.996 (0.988, 1.004) | 1.002 (0.997, 1.007) | 1.008 (1.001, 1.014) * |
| lag 1 | 0.997 (0.994, 1.000) | 0.998 (0.995, 1.002) | 0.999 (0.992, 1.006) | 0.995 (0.990, 1.000) | 1.005 (0.999, 1.010) * | |
| lag 1 | 0.999 (0.981, 1.017) | 1.001 (0.979, 1.023) | 1.039 (1.000, 1.078) * | 1.000 (0.970, 1.030) | 1.000 (0.965, 1.034) | |
| Summer | lag 0 | 0.993 (0.980, 1.005) | 0.992 (0.977, 1.007) | 1.012 (0.974, 1.051) | 1.009 (0.984, 1.035) | 1.033 (1.001, 1.066) * |
| lag 1 | 0.989 (0.976, 1.001) | 0.996 (0.981, 1.011) | 1.005 (0.969, 1.042) | 1.022 (0.997, 1.048) * | 1.016 (0.985, 1.047) | |
| Fall | lag 0 | 0.997 (0.986, 1.008) | 0.998 (0.985, 1.011) | 1.044 (1.015, 1.075) ** | 1.001 (0.986, 1.017) | 1.004 (0.983, 1.025) |
| lag 3 | 0.997 (0.986, 1.007) | 0.989 (0.977, 1.002) | 1.028 (1.001, 1.056) * | 0.996 (0.980, 1.013) | 1.014 (0.991, 1.036) | |
| Winter | lag 0 | 1.026 (1.011, 1.042) ** | 1.031 (1.013, 1.050) ** | 0.996 (0.966, 1.027) | 1.028 (1.003, 1.052) * | 1.004 (0.975, 1.034) |
| lag 1 | 1.017 (1.002, 1.032) * | 1.025 (1.007, 1.044) ** | 0.975 (0.946, 1.005) | 1.015 (0.992, 1.039) | 1.017 (0.989, 1.046) | |
| lag 3 | 1.021 (1.005, 1.036) ** | 1.014 (0.995, 1.032) | 1.004 (0.974, 1.036) | 1.011 (0.987, 1.035) | 1.001 (0.972, 1.030) | |
| lag 4 | 1.030 (1.015, 1.044) ** | 1.037 (1.019, 1.055) ** | 1.006 (0.976, 1.038) | 1.040 (1.016, 1.065) ** | 1.016 (0.986, 1.046) |
| Health Outcomes | Season | OR | Confidence Interval | p-Value | |
|---|---|---|---|---|---|
| 2.50% | 97.50% | ||||
| All-cause mortality | spring | 1.00 | 1.00 | 1.05 | 0.88 |
| summer | 1.00 | 0.99 | 1.01 | 0.13 | |
| winter | 0.98 * | 0.97 | 0.89 | <0.01 | |
| Cardiovascular mortality | spring | 1.00 | 0.99 | 1.05 | 0.66 |
| summer | 1.00 | 0.99 | 1.00 | 0.04 | |
| winter | 0.98 * | 0.97 | 0.94 | <0.01 | |
| Respiratory mortality | spring | 1.00 | 0.99 | 1.17 | 0.860 |
| summer | 1.00 | 0.99 | 1.08 | 0.670 | |
| winter | 0.97 * | 0.94 | 0.97 | 0.030 | |
| Cardiac | spring | 1.00 | 0.99 | 1.11 | 0.65 |
| summer | 1.00 | 0.99 | 1.04 | 0.54 | |
| winter | 0.98 * | 0.96 | 0.92 | <0.01 | |
| Stroke | spring | 1.00 | 0.99 | 1.08 | 0.64 |
| summer | 1.00 | 0.99 | 1.05 | 0.36 | |
| winter | 0.98 * | 0.96 | 0.98 | 0.03 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Zheng, C.; Ma, Z.; Quan, W. Acute and Cumulative Effects of Haze Fine Particles on Mortality and the Seasonal Characteristics in Beijing, China, 2005–2013: A Time-Stratified Case-Crossover Study. Int. J. Environ. Res. Public Health 2019, 16, 2383. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132383
Li Y, Zheng C, Ma Z, Quan W. Acute and Cumulative Effects of Haze Fine Particles on Mortality and the Seasonal Characteristics in Beijing, China, 2005–2013: A Time-Stratified Case-Crossover Study. International Journal of Environmental Research and Public Health. 2019; 16(13):2383. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132383
Chicago/Turabian StyleLi, Yi, Canjun Zheng, Zhiqiang Ma, and Weijun Quan. 2019. "Acute and Cumulative Effects of Haze Fine Particles on Mortality and the Seasonal Characteristics in Beijing, China, 2005–2013: A Time-Stratified Case-Crossover Study" International Journal of Environmental Research and Public Health 16, no. 13: 2383. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132383