Metabolic Syndrome Among Primary Health Care Nursing Professionals: A Cross-Sectional Population-Based Study †

 , , ,
, , , 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
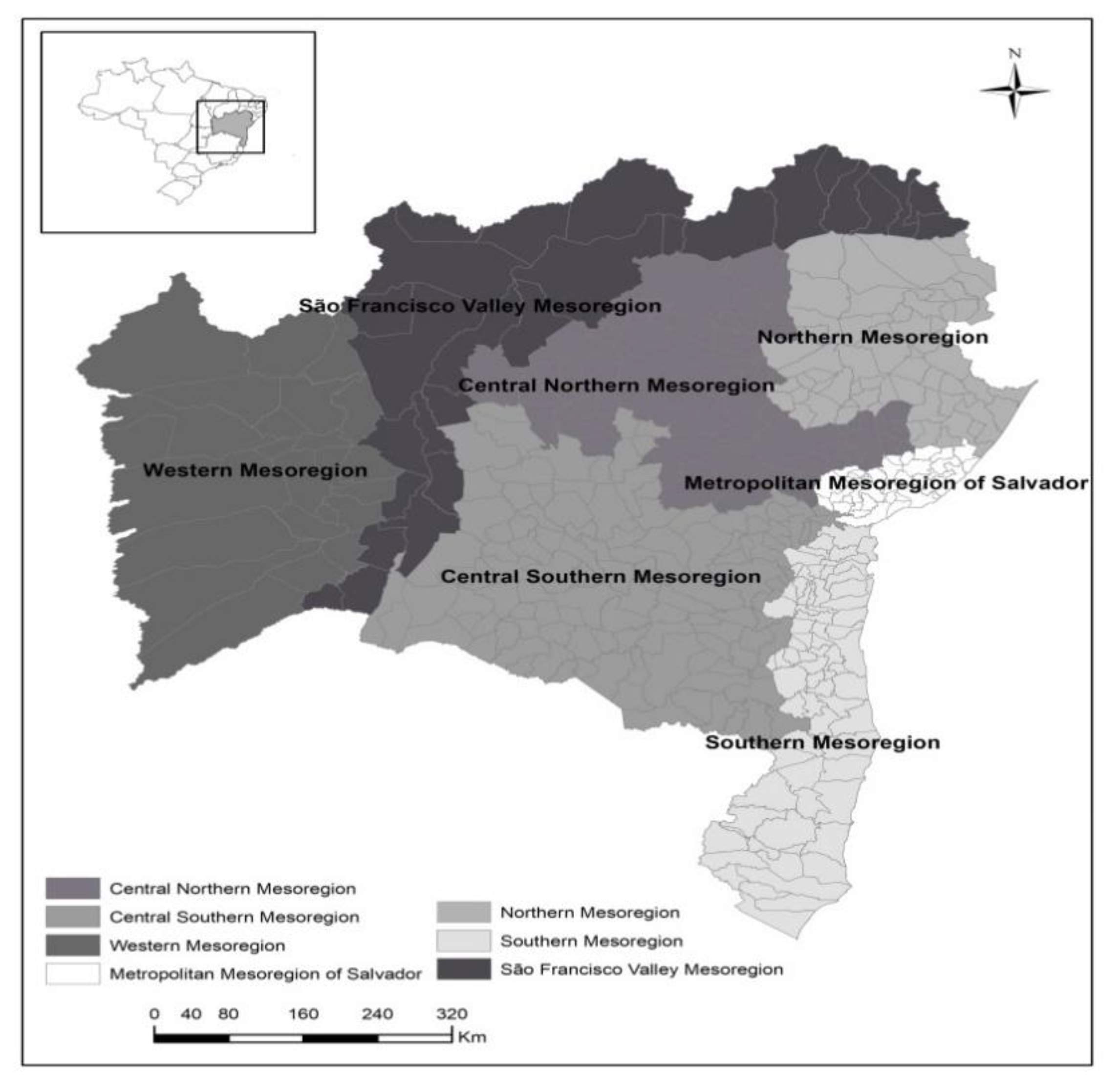
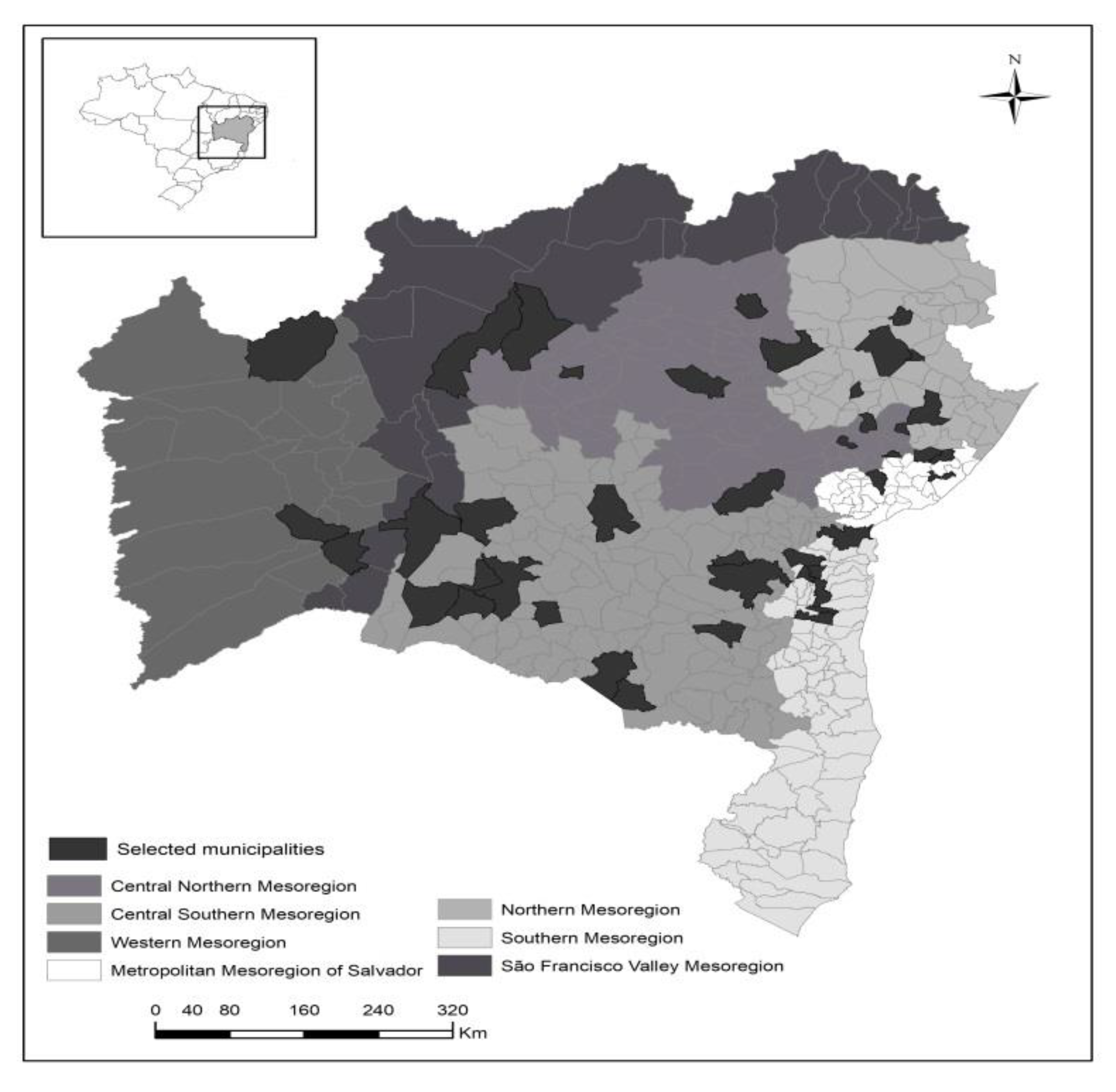
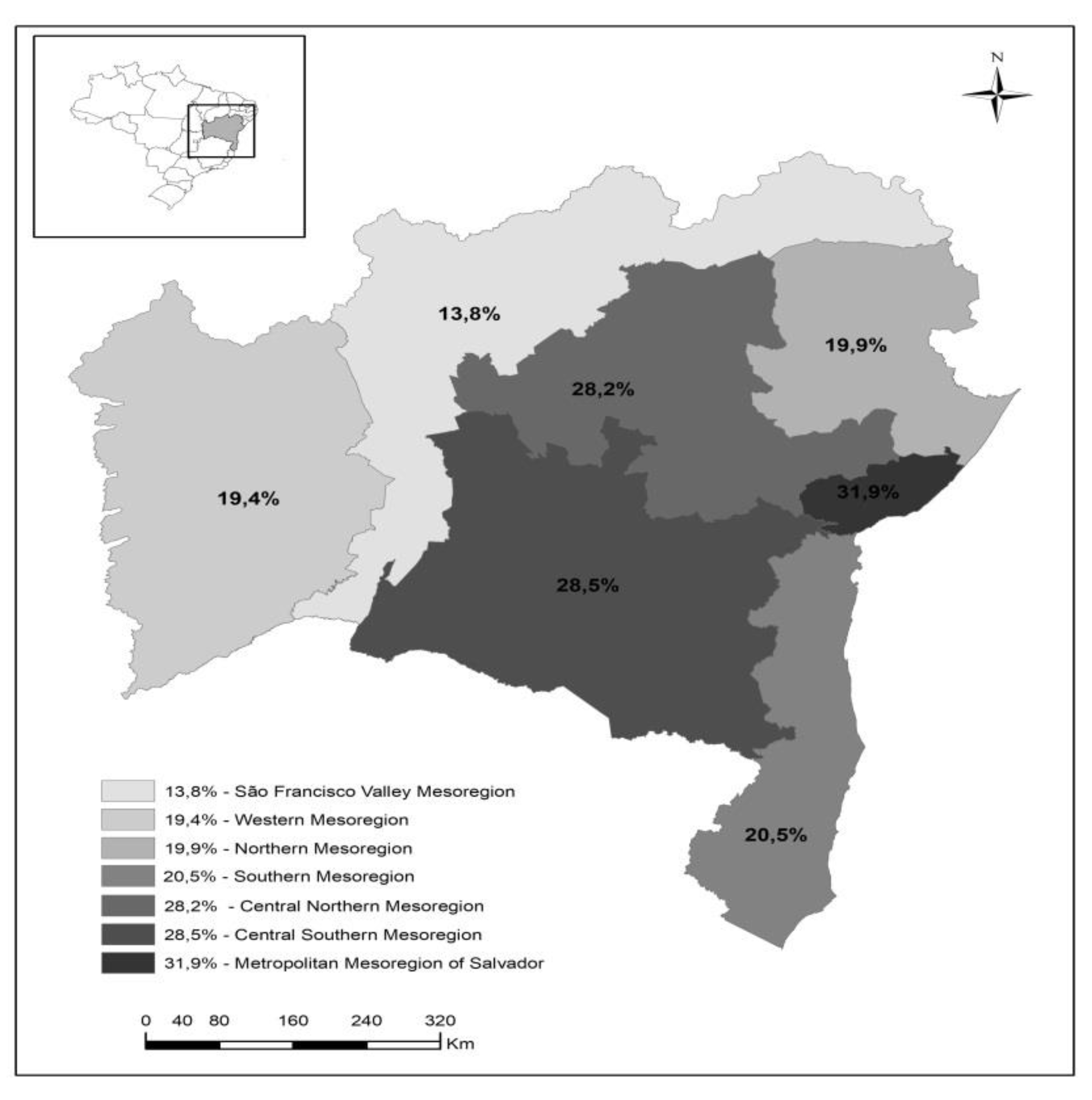
2.1. Study Design, Site and Sample
2.2. Eligibility Criteria
2.3. Data Collection and Variable Definition Procedures
2.4. Data Entry
2.5. Statistical Analyses
2.6. Ethical Aspects
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kumanyika, S.K. Global Calorie Counting: Global Calorie Counting: A Fitting Exercise for Obese Societies. Annu Rev. Public Health 2008, 29, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and metaanalysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed]
- Rezende, S.O.; Brune, M.F.S.S. Metabolic syndrome in adult users of the Family Health Care Program, Barra das Garças/MT. Rev. Bras. Anal. Clin. 2011, 43, 106–109. [Google Scholar]
- Costa, L.O.B.F.; Viana, A.O.R.; Oliveira, M. Prevalence of the metabolic syndrome in women with polycystic ovary syndrome. Rev. Bras. Ginecol. Obstet. 2007, 29, 10–17. [Google Scholar] [CrossRef]
- Gomes-Filho, I.S.; Das Merces, M.C.; de Santana Passos-Soares, J.; Seixas da Cruz, S.; Teixeira Ladeia, A.M.; Trindade, S.C.; de Moraes Marcílio Cerqueira, E.; Freitas Coelho, J.M.; Marques Monetiro, F.M.; Barreto, M.L.; et al. Severity of Periodontitis and Metabolic Syndrome: Is There an Association? J. Periodontol. 2016, 87, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Das Merces, M.C.; Cordeiro, T.M.S.C.; Santana, A.I.C.; Lua, I.; De Souza e Silva, D.; Luz, M.S.; D’Oliveira Júnior, A. Burnout syndrome in nursing workers of the primary health care. Rev. Baian. Enferm. 2016, 30, 1–9. [Google Scholar] [CrossRef]
- Carneiro, A.S.; Bordallo, A.P.N.; Carvalho, C.N.M.; Medeiros, C.B.; Monteiro, C.B.; Gilban, D.L.S.; Gazolla, F.M.; Madeira, I.R.; Borges, M.A.; Bordallo, A.N.; et al. Association of metabolic syndrome with acanthosis nigricans in prepubertal children. Rev. Ped. SOPERJ. 2016, 16, 8–14. [Google Scholar]
- Ribeiro, R.P.; Marziale, M.H.P.; Martins, J.T.; Ribeiro, P.H.V.; Robazzi, M.L.C.C.; Dalmas, J.C. Prevalence of Metabolic Syndrome among nursing personnel and its association with occupational stress, anxiety and depression. Rev. Latino Am. Enferm. 2015, 23, 435–440. [Google Scholar] [CrossRef]
- Ribeiro, R.P.; Ribeiro, P.H.V.; Marziale, M.H.P.; Martins, M.B.; dos Santos, M.R. Obesity and stress among workers from different sectors of production: An integrative review. Acta. Paul. Enferm. 2011, 24, 577–581. [Google Scholar] [CrossRef]
- Brazilian Office of Geography and Statistics (IBGE). Regional Department for Brazilian Mesoregional and Microregional Geography. 1990. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv2269_1.pdf (accessed on 1 March 2019).
- Seigel, D.G.; Podgor, M.J.; Remaley, N.A. Acceptable values of kappa for comparison of two groups. Am. J. Epidemiol. 1992, 135, 571–578. [Google Scholar] [CrossRef]
- Brazilian Hypertension Association; Brazilian Cardiology Association; Brazilian Endocrinology and Metabology Association; Brazilian Diabetes Association; Brazilian Association for Obesity Studies. 1st Brazilian Guideline for Metabolic Syndrome. Arq. Bras. Cardiol. 2005, 84, 1–28. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High BloodCholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; Schlesinger, S.; Norat, T.; Janszky, I.; Romundstad, P.; Tonstad, S.; Riboli, E.; Vatten, L.J. Body mass index, abdominal fatness, fat mass and the risk of atrial fibrillation: A systematic review and dose–response meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Habicht, J.P.; Butz, W.P. Measurement of health and nutrition effects of large-scale nutrition intervention projects. In Evaluation of the Impact of Nutrition and Health Programs; Klein, R.E., Ed.; Plenum Press: New York, NY, USA, 1979; pp. 133–189. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentration in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Stern, S.E.; Williams, K.; Ferrannini, E.; DeFronzo, R.A.; Bogardus, C.; Sterm, M.P. Idetenfication of individuals with insulin resistence using routine clinical measurement. Diabetes 2005, 54, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. Maslach Burnout Inventory, 2nd ed.; Consulting Psychologist Press: Palo Alto, CA, USA, 1986. [Google Scholar]
- Tamayo, M.R. Relation between burnout syndrome and organizational values in the nursing staff of two public hospitals. Master’s Thesis, Post-Graduation Program in Psychology, University of Brasília, Brasília, Brazil, 1997. [Google Scholar]
- Ramirez, A.J.; Graham, J.; Richards, M.A.; Cull, A.; Gregory, W.M. Mental health of hospital consultants: The effects of stress and satisfaction at work. Lancet 1996, 347, 724–728. [Google Scholar] [CrossRef]
- Coutinho, L.M.S.; Scazufca, M.; Menezes, P.R. Methods for estimating prevalence ratios in crosssectional studies. Rev. Saúde Pública 2008, 42, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Francisco, P.; Donalisio, M.; Barros, M.; Cesar, C.; Carandina, L.; Goldbaum, M. Association measures in cross-sectional studies with complex samplings: Odds ratio and prevalence ratio. Rev. Bras. Epidemiol. 2008, 11, 347–355. [Google Scholar] [CrossRef]
- Tsai, T.Y.; Cheng, J.F.; Lai, Y.M. Prevalence of metabolic syndrome and related factors in Taiwanese high-tech industry workers. Clinics 2011, 66, 1531–1535. [Google Scholar] [CrossRef] [Green Version]
- Felipe-de-Melo, E.R.T.; da Silva, R.C.R.; Assis, A.M.O.; Pinto, E.J. Factors associated with metabolic syndrome in administrative workers in the oil industry. Cien. Saude. Colet. 2011, 16, 3443–3452. [Google Scholar] [CrossRef]
- Alegria, E.; Cordero, A.; Laclaustra, M.; Grima, A.; León, M.; Casasnovas, J.A.; Luengo, E.; del Río, A.; Ferreira, I. Prevalence of metabolic syndrome in the Spanish working population: MESYAS registry. Rev. Esp. Cardiol. 2005, 58, 797–806. [Google Scholar] [CrossRef]
- Bortoletto, M.S.S.; de Souza, R.K.T.; Cabrera, M.A.S.; González, A.D. Metabolic syndrome, components and associated factors in adults aged 40 years or older from a city in southern Brazil. Cad. Saúde. Colet. 2016, 24, 32–40. [Google Scholar] [CrossRef]
- Nair, C.V. Metabolic Syndrome: An Occupational Perspective. Indian J. Community Med. 2010, 35, 122–124. [Google Scholar] [CrossRef]
- Chini, L.S.N.; Greffin, S.; Lugon, J.R. Prevalence of metabolic syndrome among workers from the Company of Generation and Distribution of Energy in Rio de Janeiro, Brazil. Cad. Saúde. Colet. 2014, 22, 359–364. [Google Scholar] [CrossRef]
- Hu, G.; Qiao, Q.; Tuomilehto, J.; Balkau, B.; Borch-Johnsen, K.; Pyorala, K. Prevalence of the metabolic syndrome and its relation to all-cause and cardiovascular mortality in nondiabetic European men and women. Arch. Intern. Med. 2004, 164, 1066–1076. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wu, Z.; Li, D.; Li, N.; Dindot, S.V.; Satterfield, M.C.; Bazer, F.W.; Wu, G. Nutrition, epigenetics, and metabolic syndrome. Antioxid. Redox Signal. 2012, 17, 282–301. [Google Scholar] [CrossRef] [PubMed]
- Simão, A.F.; Precoma, D.B.; Andrade, J.P.; Correa Filho, H.; Saraiva, J.F.K.; Oliveira, G.M.M.; Murro, A.L.B.; Campos, A.; Alessi, A.; Avezum Junior, A.; et al. I Diretriz Brasileira de Prevenção Cardiovascular. Arq. Bras. Cardiol. 2013, 101, 1–63. [Google Scholar] [CrossRef] [PubMed]
- Ramires, E.K.N.M.; Menezes, R.C.E.; Longo-Silva, G.; Marinho, P.M.; da Silveira, J.A.C. Prevalence and Factors Associated with Metabolic Syndrome among Brazilian Adult Population: National Health Survey 2013. Arq. Bras. Cardiol. 2018, 110, 455–466. [Google Scholar] [CrossRef]
- Das Merces, M.C.; De Souza e Silva, D.; Lua, I.; Oliveira, D.S.; Souza, M.C. Burnout syndrome and abdominal adiposity among Primary Health Care nursing professionals. Psicol. Reflex. Crit. 2016, 29, 2–8. [Google Scholar] [CrossRef]
- Sposito, A.C.; Caramelli, B.; Fonseca, F.A.; Bertolami, M.C.; Afiune Neto, A.; Souza, A.D.; Lottenberg, A.M.P.; Chacra, A.P.; Faludi, A.A.; Loures-Vale, A.A.; et al. IV Brazilian Guideline on Dyslipidemia and Prevention of Atheroclerosis: Atheroclerosis Departament of Brazilian Cardiology Association. Arq. Bras. Cardiol. 2007, 88, 1–18. [Google Scholar]
- Tsai, H.H.; Yeh, C.Y.; Su, C.T.; Chen, C.J.; Peng, S.M.; Chen, R.Y. The effects of exercise program on burnout and metabolic syndrome components in banking and insurance workers. Ind. Health 2013, 51, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B.; American College of Sports, M.; et al. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement executive summary. Diabetes Care 2010, 33, 2692–2696. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Huang, J.P.; Xu, G.F.; Chen, D.X.; Wu, G.Y.; Zhang, M.; Shen, Y.; Cai, H. Association of alcohol consumption and components of metabolic syndrome among people in rural China. Nutr. Metab. 2015, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Aballay, L.R.; Eynard, A.R.; Díaz Mdel, P.; Navarro, A.; Muñoz, S.E. Overweight and obesity: A review of their relationship to metabolic syndrome, cardiovascular disease, and cancer in South America. Nutr. Rev. 2013, 71, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, T.; Baydur Şahin, S.; Şahin, O.Z. Relation of Acanthosis nigricans to metabolic syndrome in overweight and obese women. Metab. Syndr. Relat. Disord. 2014, 126, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, R.P.; Marziale, M.H.P.; Martins, J.T.; Galdino, M.J.Q.; Ribeiro, P.H.V. Occupational stress among health workers of a university hospital. Rev. Gaúcha Enferm. 2018, 39, 1–6. [Google Scholar] [CrossRef]
- Chandola, T.; Brunner, E.; Marmot, M. Chronic stress at work and the metabolic syndrome: Prospective study. BMJ. 2006, 332, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Davila, E.P.; Florez, H.; Fleming, L.E.; Lee, D.J.; Goodman, E.; LeBlanc, W.G.; Caban-Martinez, A.J.; Arheart, K.L.; McCollister, K.E.; Christ, S.L.; et al. Prevalence of the metabolic syndrome among U.S. workers. Diabetes Care 2010, 33, 2390–2395. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Ann. Rev. Psycol. 2001, 52, 397–422. [Google Scholar] [CrossRef]
- Melamed, S.; Shirom, A.; Toker, S.; Berliner, S.; Shapira, I. Burnout and risk of cardiovascular disease: Evidence, possible causal paths, and promising research directions. Psychol. Bull. 2006, 132, 327–353. [Google Scholar] [CrossRef]
- Ranchal-Sánchez, A.; Vaquero-Abellán, M. Protocol for the monitoring of the health of teachers with attention to the occupational disease. Med. Segur. Trab. 2008, 54, 47–60. [Google Scholar]
- Kitaoka-Higashiguchi, K.; Morikawa, Y.; Miura, K.; Ishizaki, M.; Kido, T.; Naruse, Y.; Nakagawa, H. Burnout and risk factors for arteriosclerotic disease: Follow-up study. J. Occup. Health. 2009, 51, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Metlaine, A.; Sauvet, F.; Gomez-Merino, D.; Boucher, T.; Elbaz, M.; Delafosse, J.Y.; Leger, D.; Chennaoui, M. Sleep and biological parameters in professional burnout: A psychophysiological characterization. PLoS ONE 2018, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Artalejo, F.; Graciani, A.; Guallar-Castillon, P.; Leon-Munoz, L.M.; Zuluaga, M.C.; Lopez-Garcia, E.; Gutierrez-Fisac, J.L.; Taboada, J.M.; Aguilera, M.T.; Regidor, E.; et al. Justificación y métodos del estudio sobre nutrición y riesgo cardiovascular en España. Rev. Esp. Cardiol. 2011, 64, 876–882. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) | Metabolic Syndrome (n = 1111) a | ||
|---|---|---|---|---|
| P (%) b | PR c (CI) d | p-Value e | ||
| Sex (n = 1125) | ||||
| Male | 136 (12.1) | 40 (29.4) | 1.00 | |
| Female | 989 (87.9) | 231 (23.7) | 0.81 (0.61–1.07) | 0.14 |
| Age (n = 1125) | ||||
| Up to 35 years old | 587 (52.2) | 110 (18.9) | 1.00 | |
| 36 years old or older | 538 (47.8) | 161 (30.2) | 1.59 (1.29–1.97) | <0.01 * |
| Profession (n = 1125) | ||||
| Nurse | 455 (40.4) | 80 (17.7) | 1.00 | |
| Nursing Technician | 670 (59.6) | 191 (28.9) | 1.64 (1.29–2.07) | <0.01 * |
| Race (n = 1098) a | ||||
| Non-Black People | 246 (22.4) | 48 (19.5) | 1.00 | |
| Black People | 852 (77.6) | 220 (26.3) | 1.35 (1.02–1.78) | 0.03 * |
| Satisfaction with current occupation (n = 1125) | ||||
| Yes | 987 (87.7) | 233 (23.9) | 1.00 | |
| No | 138 (12.3) | 38 (27.7) | 1.16 (0.87–1.55) | 0.33 |
| Occupation time in PHC (n = 1125) | ||||
| Up to 4 years old | 555 (49.3) | 109 (19.7) | 1.00 | |
| 5 years old or older | 570 (50.7) | 162 (29.0) | 1.47 (1.19–1.82) | <0.01 * |
| Night shift (n = 1125) | ||||
| No | 894 (79.5) | 206 (23.3) | 1.00 | |
| Yes | 231 (20.5) | 65 (28.6) | 1.23 (0.97–1.56) | 0.09 |
| Family income (n = 1125) | ||||
| Up to two minimum wages | 523 (46.5) | 141 (27.5) | 1.27 (1.03–1.56) | 0.02 * |
| three or more minimum wages | 602 (53.5) | 130 (21.7) | 1.00 | |
| Economic situation (n = 1125) | ||||
| Satisfied | 573 (50.9) | 124 (22.1) | 1.00 | |
| Dissatisfied | 552 (49.1) | 147 (26.8) | 1.21 (0.99–1.49) | 0.07 |
| Work bond (n = 1125) | ||||
| Stable | 866 (77) | 220 (25.8) | 1.00 | |
| Precarious | 259 (23) | 51 (19.8) | 0.77 (0.58–1.01) | 0.05 * |
| Submitted to work-related aggression (n = 1225) | ||||
| No | 751 (66.8) | 167 (22.6) | 1.00 | |
| Yes | 374 (33.2) | 104 (28.0) | 1.24 (1.01–1.53) | 0.04 * |
| Rest break (n = 1125) | ||||
| Yes | 672 (59.7) | 143 (21.7) | 1.00 | |
| No | 453 (40.3) | 128 (28.3) | 1.30 (1.06–1.59) | 0.01 * |
| Work conditions (n = 1125) | ||||
| Satisfactory | 698 (62.0) | 162 (23.6) | 1.00 | |
| Precarious | 427 (38.0) | 109 (25.7) | 1.09 (0.88–1.34) | 0.44 |
| Variables | n (%) | Metabolic Syndrome (n = 1111) a | ||
|---|---|---|---|---|
| P (%) b | PRc (CI) d | p value e | ||
| Quality of life (n = 1125) | ||||
| Good | 836 (74.3) | 189 (22.9) | 1.00 | |
| Poor | 289 (25.7) | 82 (28.4) | 1.23 (0.99–1.54) | 0.07 |
| Polycystic ovary (n = 964) a | ||||
| No | 807 (83.7) | 192 (24.2) | 1.00 | |
| Yes | 157 (16.3) | 34 (21.7) | 0.89 (0.65–1.23) | 0.49 |
| Psychiatric follow-up (n = 1111) a | ||||
| No | 728 (65.5) | 169 (23.6) | 1.00 | |
| Yes | 383 (34.5) | 96 (25.3) | 1.07 (0.86–1.33) | 0.53 |
| Practice of physical activities (n = 1125) | ||||
| Yes | 639 (56.8) | 130 (20.6) | 1.00 | |
| No | 486 (43.2) | 141 (29.3) | 1.42 (1.15–1.75) | <0.01 * |
| Smoking (n = 1125) | ||||
| No | 992 (88.2) | 228 (23.3) | 1.00 | |
| Yes | 133 (11.8) | 43 (32.3) | 1.39 (1.06–1.82) | 0.02 * |
| Consumption of alcoholic beverage (n = 1125) | ||||
| No | 1083 (96.3) | 255 (23.8) | 1.00 | |
| Yes | 42 (3.7) | 16 (39.0) | 1.64 (1.10–2.44) | 0.03 * |
| Last medical consultation (n = 1125) | ||||
| Less than 12 months | 924 (82.1) | 222 (24.3) | 1.00 | |
| More than 12 months | 201 (17.9) | 49 (24.7) | 1.02 (0.78–1.33) | 0.89 |
| Presence of periodontitis (n = 848) a | ||||
| No | 740 (87.3) | 165 (22.6) | 1.00 | |
| Yes | 108 (12.7) | 27 (25.0) | 1.11 (0.78–1.57) | 0.58 |
| Acanthosis Nigerians (n = 1125) | ||||
| No | 1067 (94.8) | 227 (21.6) | 1.00 | |
| Yes | 58 (5.2) | 44 (75.9) | 3.52 (2.92–4.24) | <0.01 * |
| Non-alcoholic fatty liver disease (n = 1073) a | ||||
| No | 1040 (96.9) | 242 (23.6) | 1.00 | |
| Yes | 33 (3.1) | 18 (54.5) | 2.31 (1.66–3.22) | <0.01 * |
| Obstructive sleep apnea (n = 1076) a | ||||
| No | 967 (89.9) | 212 (22.2) | 1.00 | |
| Yes | 109 (10.1) | 50 (45.9) | 2.06 (1.63–2.61) | <0.01 * |
| Insulin resistance (n = 132) a | ||||
| No | 103 (78.0) | 17 (16.5) | 1.00 | |
| Yes | 29 (22.0) | 17 (58.6) | 3.55 (2.09–6.04) | <0.01 * |
| Burnout syndrome (n = 1121) a | ||||
| No | 916 (81.7) | 192 (21.3) | 1.00 | |
| Yes | 205 (18.3) | 78 (38.1) | 1.79 (1.44–2.22) | <0.01 * |
| Factors Associated with MS * | PRadjusted | CI (95%) |
|---|---|---|
| Physical activity | 1.25 | (1.02–1.53) |
| Consumption of alcoholic beverage | 1.84 | (1.22–2.77) |
| Acanthosis nigricans | 3.23 | (2.65–3.92) |
| Burnout syndrome | 1.45 | (1.17–1.81) |
| Age | 1.37 | (1.12–1.69) |
| Profession | 1.43 | (1.14–1.80) |
| Area under the ROC Curve | 0.70 | |
| Goodness-of-fit test ¥ | 0.62 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
das Merces, M.C.; Santana, A.I.C.; Lua, I.; da Silva, D.A.R.; e Silva, D.d.S.; Gomes, A.M.T.; Miranda, M.C.d.M.; Barbosa, C.d.S.; Magalhães, L.B.N.C.; Coelho, J.M.F.; et al. Metabolic Syndrome Among Primary Health Care Nursing Professionals: A Cross-Sectional Population-Based Study. Int. J. Environ. Res. Public Health 2019, 16, 2686. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152686
das Merces MC, Santana AIC, Lua I, da Silva DAR, e Silva DdS, Gomes AMT, Miranda MCdM, Barbosa CdS, Magalhães LBNC, Coelho JMF, et al. Metabolic Syndrome Among Primary Health Care Nursing Professionals: A Cross-Sectional Population-Based Study. International Journal of Environmental Research and Public Health. 2019; 16(15):2686. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152686
Chicago/Turabian Styledas Merces, Magno Conceição, Amália Ivine Costa Santana, Iracema Lua, Dandara Almeida Reis da Silva, Douglas de Souza e Silva, Antonio Marcos Tosoli Gomes, Manuela Conceição das Merces Miranda, Caroline da Silva Barbosa, Lucélia Batista Neves Cunha Magalhães, Julita Maria Freitas Coelho, and et al. 2019. "Metabolic Syndrome Among Primary Health Care Nursing Professionals: A Cross-Sectional Population-Based Study" International Journal of Environmental Research and Public Health 16, no. 15: 2686. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16152686