Adjustment Disorder and Suicidal Behaviours Presenting in the General Medical Setting: A Systematic Review


Abstract
:1. Introduction
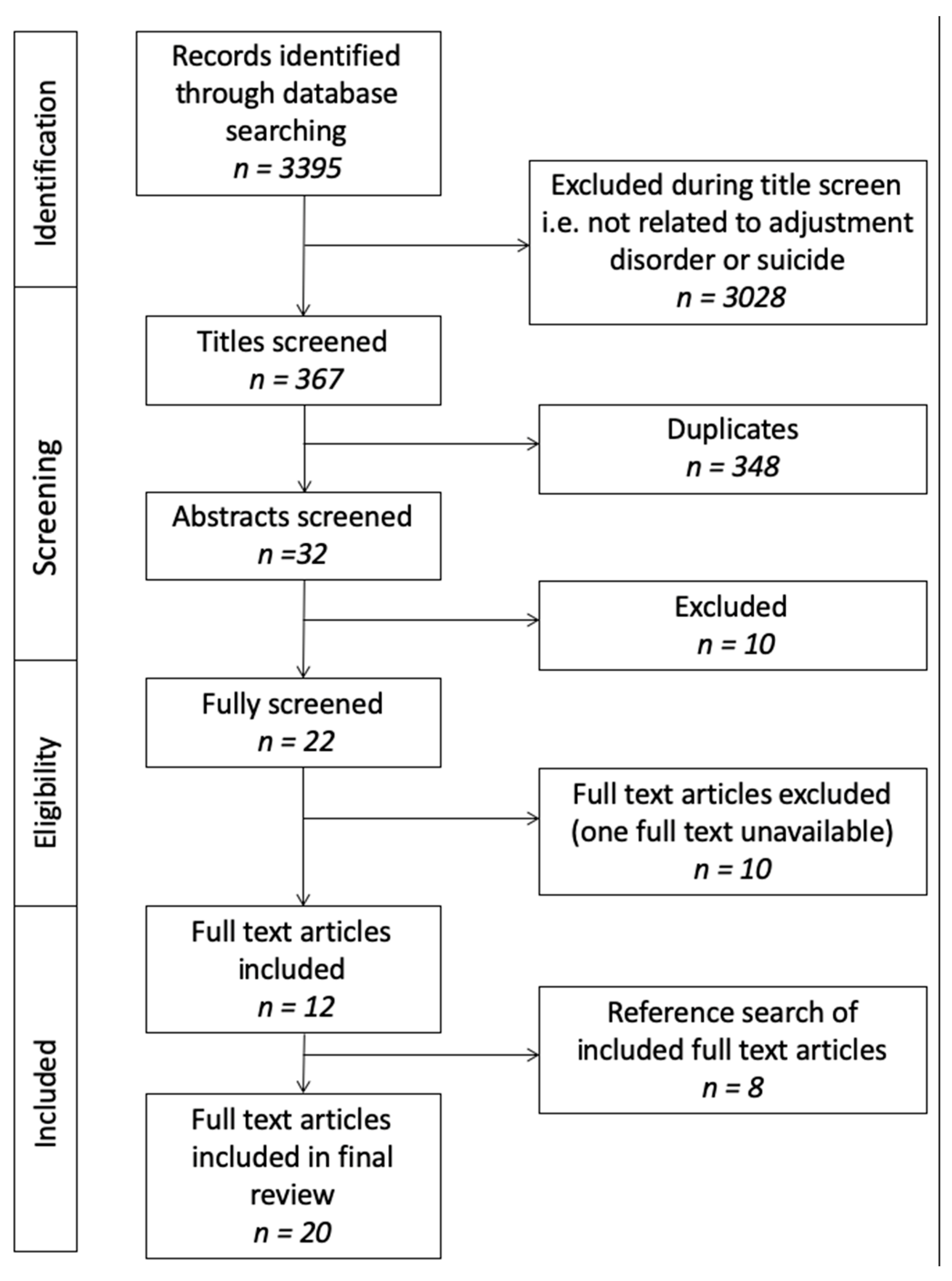
2. Materials and Methods
- (a)
- Included patients diagnosed with AD, either clinical diagnosis or using structured diagnostic instruments.
- (b)
- Conducted in medical settings where the specialty of liaison psychiatry is to be found i.e., emergency departments/rooms, general medical wards, critical care units etc.
- (c)
- Described patients presenting with self-harm (regardless of suicidal intent) or suicidal ideation.
- (d)
- Studies that included at least one clinical characteristic in addition to diagnosis (self-harm methods, previous attempts, etc.
- (e)
- Observational studies with or without comparison groups.
3. Results
3.1. Description of Studies
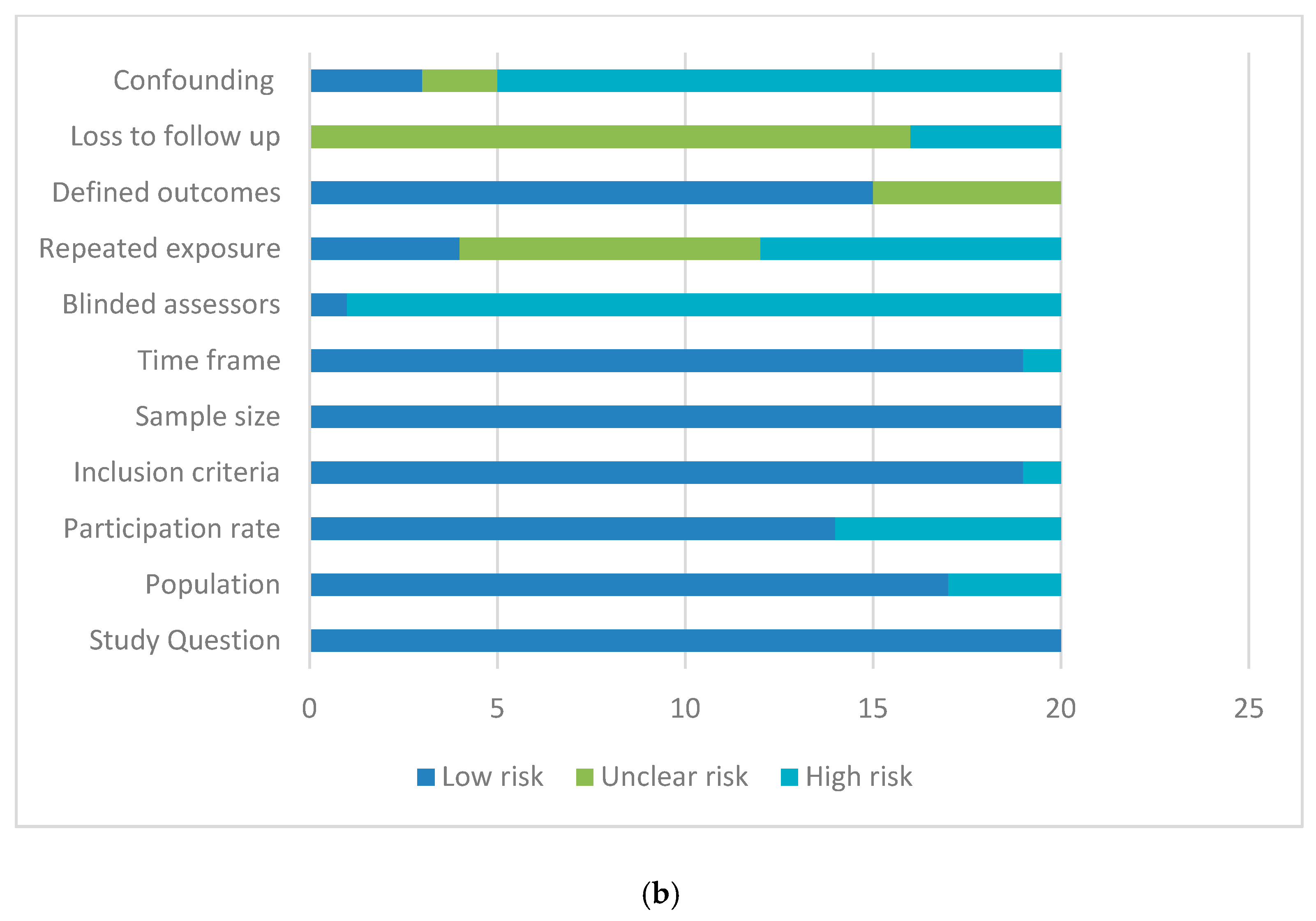
3.2. Methodological Quality of Studies
3.3. Socio-Demographic Factors
3.3.1. Age
3.3.2. Gender
3.4. Frequency of Adjustment Disorder (AD) Diagnosis
3.5. Suicide Attempt Method and Mortality Rates
3.6. Precipitants
4. Discussion
4.1. Strengths and Limitations
4.2. Further Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Silverstone, P.H. Prevalence of psychiatric disorders in medical inpatients. J. Nerv. Ment. Dis. 1996, 184, 43–51. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. International Classification of Diseases, 10th ed.; World Health Organisation: Geneva, Switzerland, 1992. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Zimmerman, M.; Martinez, J.H.; Dalrymple, K.; Martinez, J.H.; Chelminski, I.; Young, D. Is the distinction between adjustment disorder with depressed mood and adjustment disorder with mixed anxious and depressed mood valid? Ann. Clin. Psychiatry 2013, 25, 257–265. [Google Scholar] [PubMed]
- Baumeister, H.; Maercker, A.; Casey, P. Adjustment disorder with depressed mood: A critique of its DSM-IV and ICD-10 conceptualisations and recommendations for the future. Psychopathology 2009, 42, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Casey, P. Diagnosing adjustment disorder with depressive features. Expert Rev. Neurother. 2008, 8, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Polyakova, I.; Knobler, H.Y.; Ambrumova, A.; Lerner, V. Characteristics of suicidal attempts in major depression versus adjustment reactions. J. Affect. Disord. 1998, 47, 159–167. [Google Scholar] [CrossRef]
- Maercker, A.; Brewin, C.R.; Bryant, R.A.; Cloitre, M.; Van Ommeren, M.; Jones, L.M.; Humayan, A.; Kagee, A.; Llosa, A.E.; Rousseau, C.; et al. Diagnosis and classification of disorders specifically associated with stress: Proposals for ICD-11. World Psychiatry 2013, 12, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Huyse, F.J.; Herzog, T.; Lobo, A.; Malt, U.F.; Opmeer, B.C.; Stein, B.; Jonge, P.; van Dijck, R.; Creed, F.; Crespo, M.D.; et al. Consultation-Liaison psychiatric service delivery: Results from a European study. Gen. Hosp. Psychiatry 2001, 23, 124–132. [Google Scholar] [CrossRef]
- National Institutes of Health (NIH). Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. NIH, 2018. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 12 August 2019).
- Troya, M.I.; Babatunde, O.; Polidano, K.; Bartlam, B. Self-harm in older adults: Systematic review. Br. J. Psychiatry 2019, 214, 186–200. [Google Scholar] [CrossRef]
- Farzaneh, E.; Mehrpour, O.; Alfred, S.; Moghaddam, H.H.; Behnoush, B.; Seghatoleslam, T. Self-poisoning suicide attempts among students in Tehran, Iran. Psychiatr. Danub. 2010, 22, 34–38. [Google Scholar]
- Magat, R.C.; Guerrero, A.P.S. Suicidal behaviour trends in a pediatric population in Hawai’i. Hawaii Med. J. 2008, 673, 69–73. [Google Scholar]
- Suss, A.; Homel, P.; Wilson, T.E.; Shah, B. Risk factors for nonfatal suicide behaviors among inner-city adolescents. Pediatr. Emerg. Care 2004, 20, 426–429. [Google Scholar] [CrossRef] [PubMed]
- Lingeswaran, A. Profile of Young Suicide Attempt Survivors in a Tertiary Care Hospital in Puducherry. Indian J. Psychol. Med. 2016, 38, 533–539. [Google Scholar] [CrossRef] [Green Version]
- Mitrev, I. A study of deliberate self-poisoning in patients with adjustment disorders. Folia Med. 1996, 38, 11–16. [Google Scholar]
- Ghimire, S.; Devkota, S.; Budhathoki, R.; Sapkota, N.; Thakur, A. Psychiatric Comorbidities in Patients with Deliberate Self-Harm in a Tertiary Care Center. J. Nepal. Med. Assoc. 2014, 52, 697–701. [Google Scholar] [CrossRef]
- McCauley, M.; Russell, V.; Bedford, D.; Khan, A.; Kelly, R. Assessment following deliberate self-harm: Who are we seeing and are we following the guidelines? Ir. J. Psychol. Med. 2001, 18, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Galgali, R.B.; Rao, S.; Ashok, M.V.; Appaya, P.; Srinivasan, K. Psychiatric diagnosis of self poisoning cases: A general hospital study. Indian J. Psychiatry 1998, 40, 254–259. [Google Scholar] [PubMed]
- Zarghami, M.; Khalilian, A. Deliberate self-burning in Mazandaran, Iran. Burn. J. Int. Soc. Burn Inj. 2002, 28, 115–119. [Google Scholar] [CrossRef]
- AbuMadini, M.S.; Rahim, S.I.A. Deliberate self harm in a Saudi university hospital: A case series over 6 years. Arab J. Psychiatry 2001, 12, 22–35. [Google Scholar]
- Wai, B.H.; Hong, C.; Heok, K.E. Suicidal behavior among young people in Singapore. Gen. Hosp. Psychiatry 1999, 21, 128–133. [Google Scholar]
- Casey, P.; Jabbar, F.; O’Leary, E.; Doherty, A.M. Suicidal behaviours in adjustment disorder and depressive episode. J. Affect. Disord. 2015, 174, 441–446. [Google Scholar] [CrossRef]
- Brakoulias, V.; Ryan, C.; Byth, K. Patients with deliberate self-harm seen by a consultation-liaison service. Australas Psychiatry 2006, 14, 192–197. [Google Scholar] [CrossRef]
- Briskman, I.; Shelef, A.; Berger, U.; Baruch, Y.; Bar, G.; Asherov, J.; Lvovski, A.; Apter, A.; Barak, Y. Deliberate Self-Harm in Older Adults: A General Hospital Emergency Department Survey. Isr. Med. Assoc. J. 2017, 19, 160–163. [Google Scholar]
- Lin, C.; Yen, T.H.; Juang, Y.-Y.; Leong, W.C.; Hung, H.-M.; Ku, C.-H.; Li, J.-L.; Lee, S.-H. Comorbid psychiatric diagnoses in suicide attempt by charcoal burning: A 10-year study in a general hospital in Taiwan. Gen. Hosp. Psychiatry 2012, 34, 552–556. [Google Scholar] [CrossRef]
- Lin, C.; Yen, T.H.; Juang, Y.Y.; Lee, C.P.; Lee, S.H. Distinct psychopathology of patients who attempted suicide with rodenticide in Taiwan: A comparative study with patients of suicide with paraquat. Psychol. Res. Behav. Manag. 2018, 29, 323–328. [Google Scholar] [CrossRef]
- Taggart, C.; O’Grady, J.; Stevenson, M.; Hand, E.; McClelland, R.; Kelly, C. Accuracy of diagnosis at routine psychiatric assessment in patients presenting to an accident and emergency department. Gen. Hosp. Psychiatry 2006, 28, 330–335. [Google Scholar] [CrossRef]
- Grudnikoff, E.; Soto, E.C.; Frederickson, A.; Birnbaum, M.L.; Saito, E.; Dicker, R.; Kane, J.M.; Correll, C.U. Suicidality and hospitalization as cause and outcome of pediatric psychiatric emergency room visits. Eur. Child. Adolesc. Psychiatry 2015, 24, 797–814. [Google Scholar] [CrossRef]
- Portzky, G.; Audenaert, K.; van Heeringen, K. Suicide among adolescents: A psychological autopsy study of psychiatric, psychosocial and personality-related risk factors. Soc. Psychiatry Psychiatr. Epidemiol. Int. J. Res. Soc. Genet. Epidemiol. Ment. Health Serv. 2005, 40, 922–930. [Google Scholar] [CrossRef]
- Marttunen, M.J.; Aro, H.M.; Henriksson, M.M.; Lönnqvist, J.K. Adolescent suicides with adjustment disorders or no psychiatric diagnosis. Eur. Child. Adolesc. Psychiatry 1994, 3, 101–110. [Google Scholar] [CrossRef]
- Lin, Y.W.; Huang, H.C.; Lin, M.F.; Shyu, M.L.; Tsai, P.L.; Chang, H.J. Influential Factors for and Outcomes of Hospitalized Patients with Suicide-Related Behaviors: A National Record Study in Taiwan from 1997–2010. PLoS ONE 2016, 11, e0149559. [Google Scholar] [CrossRef]
- Chiou, P.-N.; Chen, Y.-S.; Lee, Y.-C. Characteristics of adolescent suicide attempters admitted to an acute psychiatric ward in Taiwan. J. Chin. Med Assoc. JCMA 2006, 69, 428–435. [Google Scholar] [CrossRef]
- Pompili, M.; Belvederi Murri, M.; Patti, S.; Innamorati, M.; Lester, D.; Girardi, P. The communication of suicidal intentions: A meta-analysis. Psychol. Med. 2016, 46, 2239–2253. [Google Scholar] [CrossRef]
- Strain, J.J.; Diefenbacher, A. The adjustment disorders: The conundrums of the diagnoses. Compr. Psychiatry 2008, 49, 121–130. [Google Scholar] [CrossRef]
- Doherty, A.M.; Kelly, B.D.; Jabbar, F.; Casey, P. Distinguishing between adjustment disorder and depressive episode in clinical practice: The role of personality disorder. J. Affect. Disord. 2014, 168, 78–85. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Study | Type | No. of Participants | Setting | Age | Diagnosis | Study Length | Self-Harm Method | Previous or Subsequent Attempt | Death | Influencing Factors/Precipitants |
|---|---|---|---|---|---|---|---|---|---|---|
| AbuMadidi et al. (2001) | Retrospective study (chart review) | 398 | ED, Saudi Arabia | 13–74 years | AD 30.1%; personality disorder 32%, depression 8.6% | 6 years | 78.7% poisoning; 26% cutting | Previous attempt in 21.5% | Not stated | Females more likely to have dx AD (p < 0.01), stressful life events (p < 0.001). Males more likely to have substance misuse (p < 0.001), psychosis (p < 0.01) |
| Brakoulias et al. (2006) | Retrospective study (chart review) | 1295 | Liaison psychiatry service, Australia | 18–88 years | AD 35.9%; major depression %; schizophrenia | 5 years | 79.2% poisoning; 12.7% cutting; 4.7% violent | 12% prior self-harm | Not stated | Women more likely to poison, men more likely to cut or violent act. Separated and divorced women 18–24 high risk. Violent group, AD less common than depression or schizophrenia. |
| Briskman et al. (2017) | Prospective cohort study | 1149 | ED Israel | 18–95 years | AD 48% most common diagnosis, personality 16%; depression; 15% depression | 8 years | 92.5% poisoning; 7.5% hanging; cutting | 30% | Not stated | AD 46.7% aged 16–64, 57.8% in >65 years |
| Casey et al., (2015) | Prospective cohort study | 348 | Liaison psychiatry services in 3 Dublin Hospitals | Mean age in AD with suicidal behaviour 36.5 years | AD 49.7%; depressive episode 51.3% | 6 months | Not stated | Not stated | None | Younger age, single marital status and greater severity of depressive symptoms. |
| Farzeneh et al. (2010) | Cross-sectional cohort study | 248 | ED, Iran | 12–18 years | AD 84.3%; major depression 18%; personality disorder 10% | Not stated | Self-poisoning | Not stated | Not stated | Female—80.64%, childhood adversity—48%, family psychiatric history—33%, substances—11% |
| Galgali et al. (1998) | Retrospective study (chart review) | 119 | ED, India | Mean age 25 years | AD 33.7%; depression 21%; schizophrenia 4.3% | One year | Self-poisoning—most common being pesticides | 9.24% of the sample had a previous attempt | Not stated/unknown | Substance abuse, epilepsy, co-morbid psychiatric illnesses |
| Ghimire et al. (2012) | Retrospective study (chart review) | 200 | ED, Nepal | 15–55 and above. 77% below the age of 34 years | AD 13.5%; mood disorder 11%; substance abuse 7% | 3 months | Self-poisoning by various compounds, pesticides being the most common | Not reported | Not reported | Gender, substance abuse, interpersonal conflict |
| Grundikoff et al. (2015) | Retrospective study (chart review) | 265 93 self-harm | ED, New York | 0–17 years | AD 417.7% | 1 year | Not reported | 57 (22.4%) | Not reported | Family conflict—30% suicidal ideation, 41% self-harm. Peer conflict—30% suicidal ideation, 41% self-harm. |
| Huyse et al. (2001) | Cross-sectional cohort study | 1795 self-harm Total in study 10560 | Liaison psychiatry services in 11 European countries | Mean age presenting with self-harm 38 years | Self-harm 17%; AD 12.4% | 1 year | Not reported | Not reported | Not reported | Self-harm 56% female, 24% transferred to psychiatric ward |
| Lin et al. (2012) | Retrospective study (chart review) | 73 | Medical admissions, Taiwan | 16–83 years | AD 41.1%; depression 49.3% | 10 years | Charcoal burning | Not reported | Not reported | Stressors included end of relationship (18%), debt (18%) and illness (18%). Male patients had higher rates of AD, comorbid with alcohol abuse. |
| Lin et al. (2018) | Retrospective study (chart review) | 174 | Medical admissions, Taiwan | Mean 45.8 years (SD20) rodenticide group; 41.2 years (SD 14.9) paraquat group | AD n = 17 (9.8%)—2(3.2%) rodenticide group; 15(14.1%) paraquat group | 12 years | Self-poisoning by either rodenticide or paraquat | n = 17 (9.8%)—3(7.6%) rodenticide group; 45(30%) paraquat group | 87 (50%) total 0 rodenticide group; 87 (58%) paraquat group. No detail by diagnosis | AD significantly associated with presentation with paraquat poisoning (high lethality group) |
| Lingeswaren et al. (2016) | Prospective cohort study | 40 | Medical admissions, India | 10–30 years | Acute stress reaction/Adjustment disorder in 100% | 6 months | Self-poisoning | 1 participant had a previous suicide attempt | Death by suicide was an exclusion criterion of this study | Female—62.5% Stressors included parenting issues 47.5%, interpersonal difficulties 30%, academic 7% |
| Magat et al. (2008) | Retrospective study (chart review) | 65 | Tertiary centre in Honolulu, Hawaii | 5–18 years | AD 29%; depressive illness (45%) | 2 years | Self-poisoning | 26% | None | Gender (female) 86%, age 13–16 68% |
| McCauley et al. (2001) | Retrospective study (chart review) | 70 | ED, rural hospital, Ireland | 10 to >60 years | AD 35.78%; depressive disorder (28.6%); schizophrenia 7.1% | 1 year | 92.9% overdose; 1.4% each for drowning, hanging, inhaling exhaust fumes, laceration of wrists | Absence or presence of previous suicidal behaviour is documented in 47.7% of charts. | None | Gender Female: Male 2:1, alcohol implicated in 47% of cases |
| Mitrev (1996) | Prospective descriptive study | 140 | Toxicological unit, Germany | 15 to >60 years | AD 100%, no additional diagnosis | 2 years | Self-poisoning | 20% had a prior suicide attempt | None | Interpersonal conflict—70%, occupational/ economic—25% |
| Polyakova, 1998 | Prospective observational study | 155 | ED, Moscow | 18–65 years | AD 55.5%; depression 44.5% | 9 months | AD group poisoning n = 60 (70%: males 19, 22%, female 41, 48%); hanging 17 (20%: males 12, 14%, female 5, 6%); other 9 (10%: males 4, 5%, female 5, 5%) | Not reported | None | AD less educated, lower social status, unmarried. Majority unfavourable childhood events. Alcohol 3 times more likely to be involved in AD than depression, more impulsive. AD regretted (92%, compared with only 12% in the depression group) |
| Suss et al. (2004) | Cross sectional cohort study | 92 | ED, New York | 12–18 years | AD 77% of the more serious suicide attempts and 50% of the less serious suicide attempts. Other diagnoses are not listed | 2 years | Self-poisoning | 32% had previous suicide attempt, with 6% having two or more previous attempts | None–the study was conducted exclusively on non-fatal suicide attempts | Gender—86% of participants were female. Ethnicity 82% of participants were African American |
| Taggart et al. (2006) | Prospective cohort study | 125 self-harm, of 167 patients in study | ED, Belfast | 13–77 years | AD—49 (31.8%) clinically; 12 (7.8) SCID Depression 30 (19.5%) clinically; 56 (36.4%) SCID | 1 year | Poisoning 104 (83.2%); cutting 10 (8%); other 11 (8.8%) | 129 (83.8%) prior self-harm, 25 (16.4) >x2 Figures given for whole sample, figures for those presenting with self-harm not described separately | Not reported | 54.5% female, 45.5% male. 67.5% previous psychiatric treatment. |
| Wai et al. (1999) | Retrospective study (chart review) | 214 | ED and medical admissions, Singapore | 13–21 years | AD (53.5%), Major depression (24.3%), Schizophrenia (1.9%) Substance misuse (0.5%) | 4 years | 90% poisoning; 6% mixed; 4% violent incl defenestration | Not reported | Not reported | Family conflict 24.5%; conflict with friends 23.6%; school problems 11%; military service in 10% of males. |
| Zhargami et al. (2002) | Prospective descriptive study, included psychological autopsy | 318 | Burns unit, Iran | No age range given. Average age of 27 years stated | AD 42.1%; major depression 11%; anxiety d/o 4.7%; schizophrenia 4.1% | Initial interviews over 2-year period, follow up interviews 8 years later | Self-immolation | 27% of cases had a previous suicide attempt | 242 or 79% of the study group died as a result of self-immolation | Marital conflict (30%), family problems (12%), “love affair” (10%), conflict with spouse’s family (5%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fegan, J.; Doherty, A.M. Adjustment Disorder and Suicidal Behaviours Presenting in the General Medical Setting: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 2967. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162967
Fegan J, Doherty AM. Adjustment Disorder and Suicidal Behaviours Presenting in the General Medical Setting: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(16):2967. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162967
Chicago/Turabian StyleFegan, Joanne, and Anne M. Doherty. 2019. "Adjustment Disorder and Suicidal Behaviours Presenting in the General Medical Setting: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 16: 2967. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162967