1. Introduction
According to the US Bureau of Transportation Statistics, approximately 9.4 million Americans (2.88%) were exposed to average 24-h aircraft noise levels exceeding 50 dB in 2017 [
1]. The most recent US sleep studies on the effects of aircraft noise on sleep date back to 1996 [
2]. Since then, US air traffic has changed significantly with changes in traffic volume and significant reductions in noise levels of single aircraft [
3]. Due to differences, e.g., in building structure, the use of central and window air conditioning, airport operational procedures, and sleep timing, results from studies performed outside the US may not transfer directly to US domestic airports. Therefore, it is important that field studies be conducted in the US to acquire current data on sleep disturbance relative to varying degrees of noise exposure.
The gold standard for measuring sleep is polysomnography, which is the simultaneous measurement of brain electrical potentials (electroencephalogram, EEG), eye movements (electrooculogram, EOG), muscle tone (electromyogram, EMG), and other signals (e.g., respiratory movements, airflow, leg movements) to diagnose sleep disorders. Sleep stages are identified based on specific patterns in the physiological signals for each 30-s segment of the night [
4]. Wake time is differentiated from sleep, and Rapid Eye Movement (REM) sleep is differentiated from non-REM sleep (stages S1 through S4). Stages S1 and S2 (N1 and N2 in the newer AASM criteria [
5]) are considered light sleep and S3 and S4 (N3 in the AASM criteria) are considered deep sleep. Shorter activations in the EEG and EMG of 3 s or longer can also be scored and are referred to as cortical arousals.
Polysomnography has been implemented in a few field studies on the effects of road, rail, or aircraft noise on sleep [
6,
7,
8,
9]. However, it is expensive to implement as trained staff are needed to apply and remove the electrodes. Trained staff are also needed to visually score sleep stages, which has both high intra- and inter-rater variability [
10,
11]. Also, the methodology is somewhat invasive and may influence sleep itself, especially during the first night(s) [
12]. A less invasive method for monitoring sleep is actigraphy, which infers sleep and wake patterns from body movements, measured using a wrist-worn device. While this approach is noninvasive and less expensive, analysis is typically based on 60-s segments and different algorithms are used to score the data. Compared to polysomnography, actigraphy has high sensitivity in identifying sleep epochs but a low specificity in identifying wake epochs [
13,
14,
15].
Awakenings are typically associated with arousals of the autonomic nervous system, which include increases in heart rate and blood pressure. Basner et al. previously developed an algorithm for automatically identifying cortical arousals of 3 s or longer in duration based on increases in heart rate alone [
16]. As these brief arousals can occur over 80 times a night without noise exposure, they are not considered a specific indicator of noise-induced sleep disturbance [
17,
18]. Therefore, during an earlier stage of this project, this algorithm was refined in order to only identify cortical arousals that are 15 s or longer in duration [
19], which is the indicator of noise-induced sleep disturbance most commonly used in the field and a more specific indicator of sleep disruption [
18]. Body movements measured with actigraphy were also newly included in the algorithm. The agreement between cortical arousals identified visually based on polysomnography data and arousals identified using the refined ECG- and actigraphy-based algorithm was evaluated by calculating Cohen’s Kappa, which represents agreement corrected for chance. A Kappa value greater than 0.80 was found, which is considered as a “near perfect” agreement between the two approaches according to conventional standards [
20]. An advantage of using ECG and actigraphy only for monitoring sleep is that participants can apply the equipment themselves; therefore, reducing the methodological study cost as staff are not needed in the field each night and morning. In addition, the combined ECG/actigraphy device used in this study only required 2 chest electrodes (1 derivation of the ECG) compared to the multiple electrodes and wires that are required for polysomnographic sleep studies, which may have an effect on an individual’s sleep quality. Finally, the algorithm that was developed allows arousals to be identified automatically and consistently across studies.
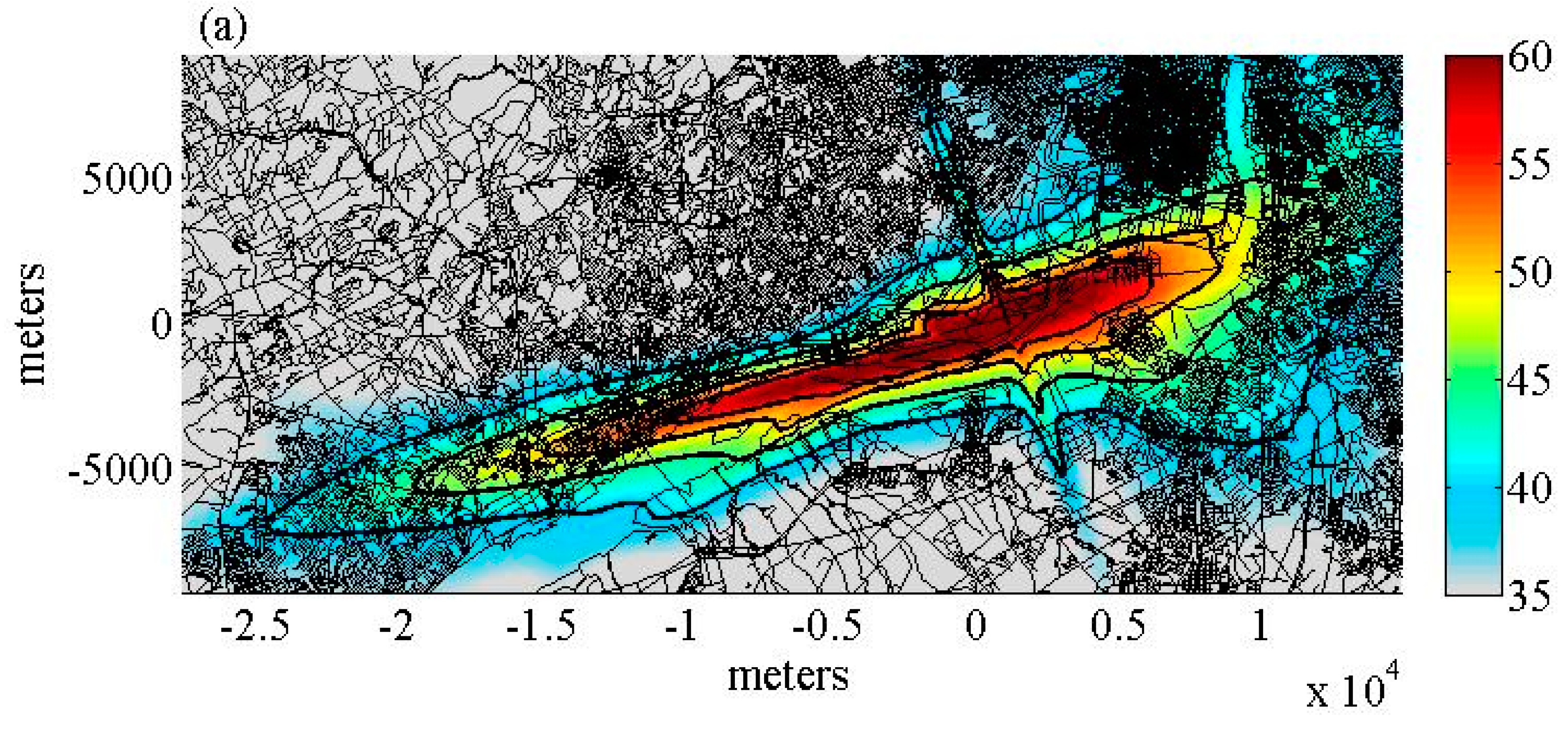
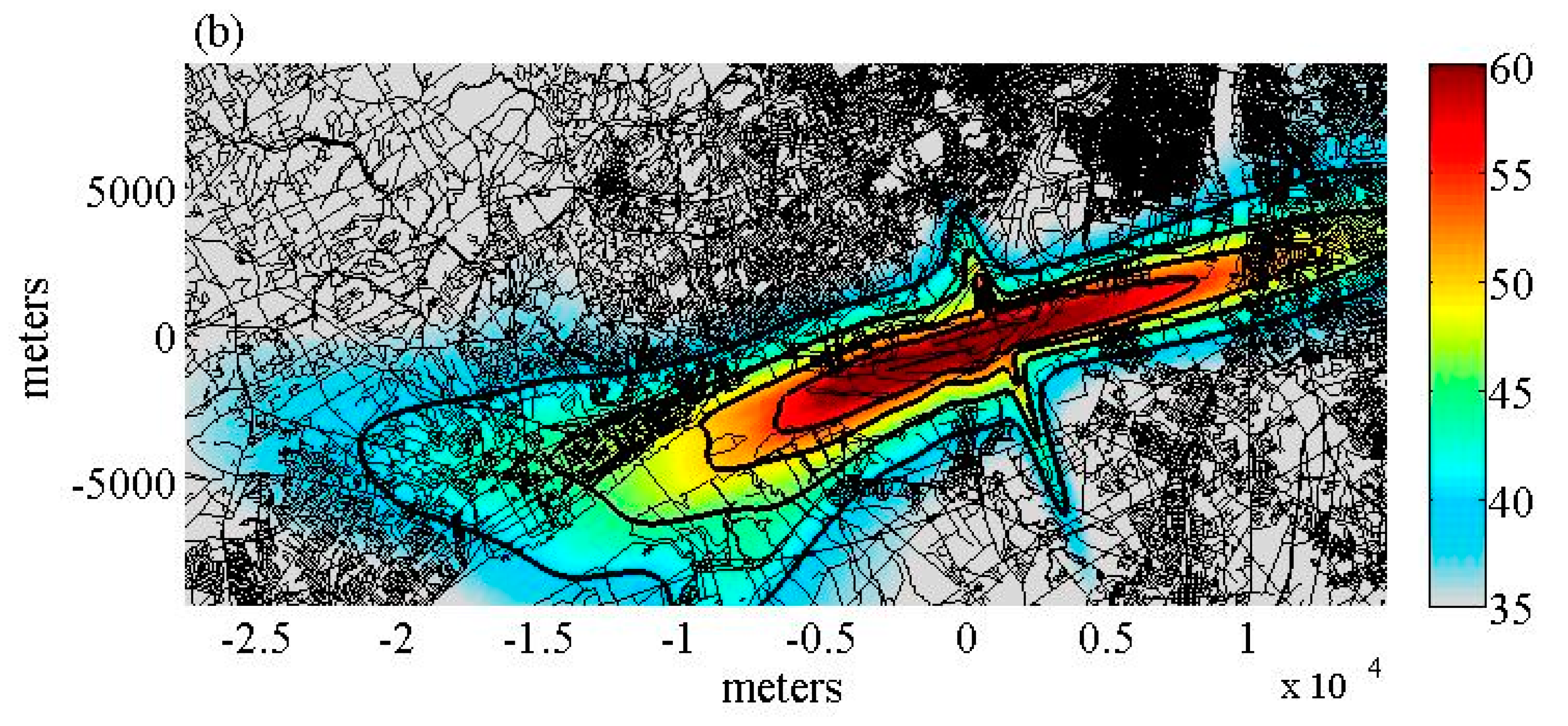
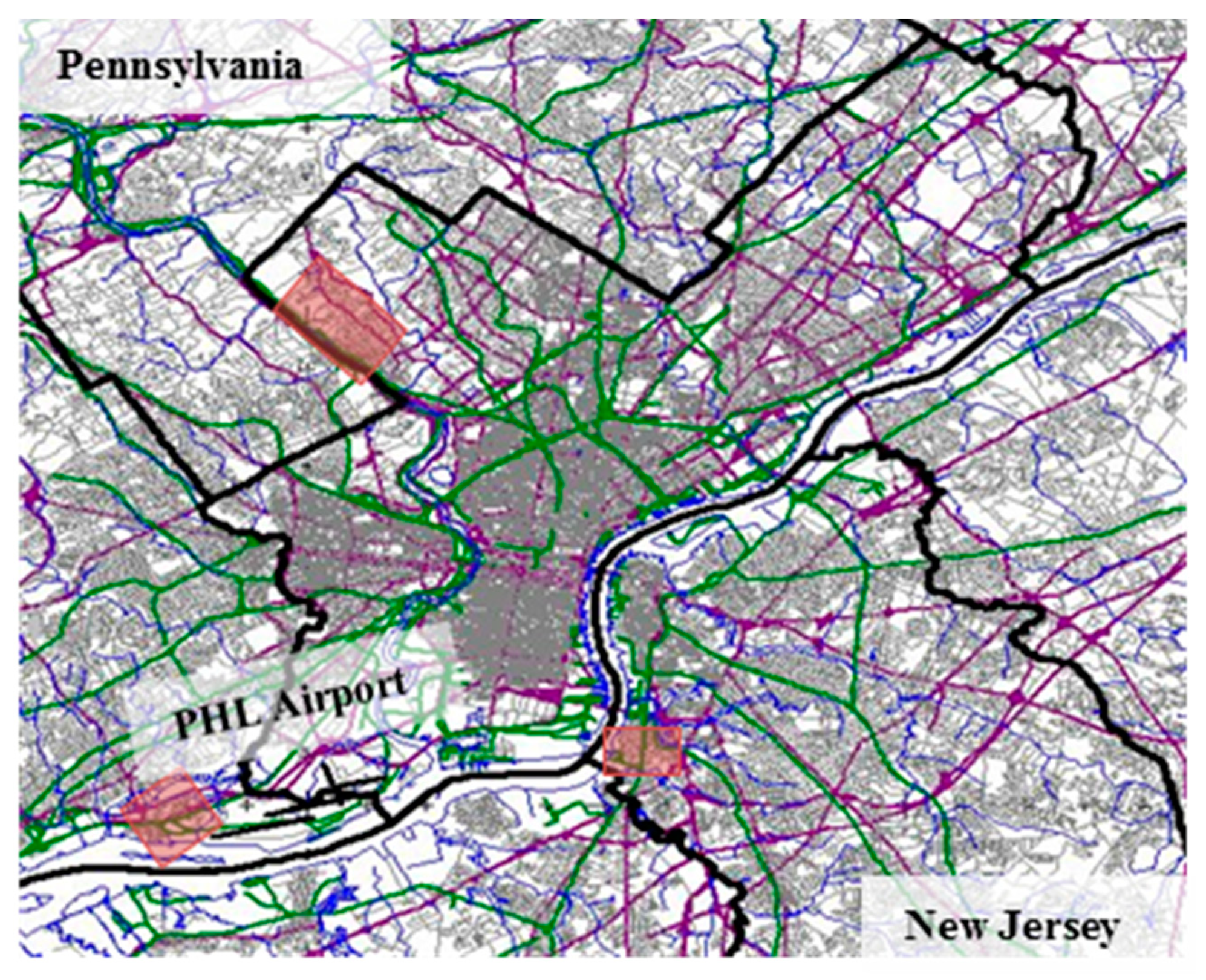
The methodology of using ECG and actigraphy to monitor sleep was implemented in a pilot study that was conducted around Philadelphia International Airport (PHL). Eighty participants were enrolled in the study, with each participant completing three nights of unattended sleep measurements. Forty participants were recruited from regions near PHL airport and 40 were recruited from regions without relevant air-traffic in Philadelphia County. The primary objective of this study was to evaluate the feasibility of the study methodology, in particular the quantity and quality of data that could be obtained when participants use physiological and noise measurement equipment unattended. A secondary objective of this study was to compare objective and subjective measures of sleep and health between control and aircraft noise exposed groups.
4. Discussion
The primary objective of this pilot field study was to evaluate the feasibility, and more specifically, the quantity and quality of the data that could be obtained when sleep and noise measurements were completed unattended. For all measurements, there was less than 10% data loss. Participants were able to correctly apply the electrodes and use the heart rate/actigraphy device. The primary reason for data loss was cables coming off the electrodes. However, actigraphy data was obtained in all cases. Additionally, participants turned on the sound recorder for the majority of nights. Overall, this demonstrates the feasibility of unattended physiological and noise measurements.
The second objective of this study was to evaluate whether there were differences in objective and subjective sleep and health measures between the airport and the control region. The sleep fragmentation index was higher in residents living near PHL airport relative to residents living in the control region, albeit statistically non-significantly. This can likely be attributed to the low statistical power of this pilot field study. It is somewhat surprising, though, especially since a significant exposure-response relationship between aircraft noise L
ASmax and awakenings inferred from body movements and ECG arousals was found. It is possible that airport residents were able to compensate for noise-induced awakenings during noise-free intervals [
24]. Furthermore, the ECG-based algorithm is somewhat less sensitive in older subjects, and even though we adjusted for age in our models, residual confounding may have masked a higher sleep fragmentation in airport residents.
High blood pressure and cardiovascular disease have been shown to be associated with chronic exposure to aircraft noise [
27,
28]. However, in this study, we did not find a significant difference in either systolic or diastolic blood pressure between those living near the airport and those living in the control region. However, the power of this pilot study was likely too low to detect small differences in morning blood pressure.
For subjective responses, it was found that those living near the airport reported poorer sleep quality reflected in responses to the PROMIS and PSQI sleep questions, and poorer health as reported in the SF-36. It is currently unclear whether additional confounding variables that were not collected in the current study may account for some of these differences. The extension of this pilot study conducted around a different US airport collected more extensive information on noise exposure, attitudes, and health outcomes, and will thus likely shed more light on this question. The PROMIS and PSQI sleep questions referred to a one-month time frame. When participants were asked in the morning about their last night’s sleep, no significant difference was found between the airport and the control group.
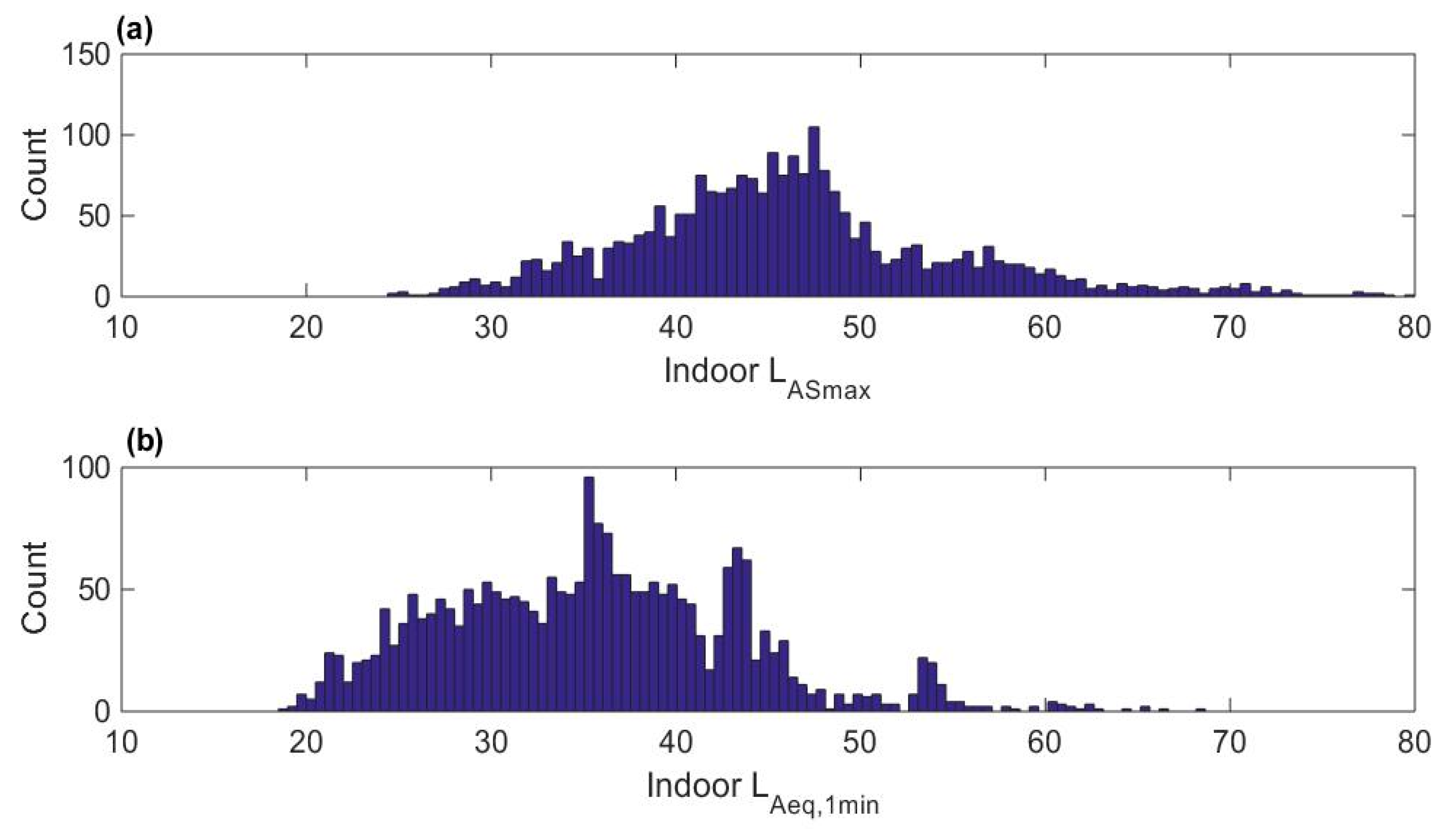
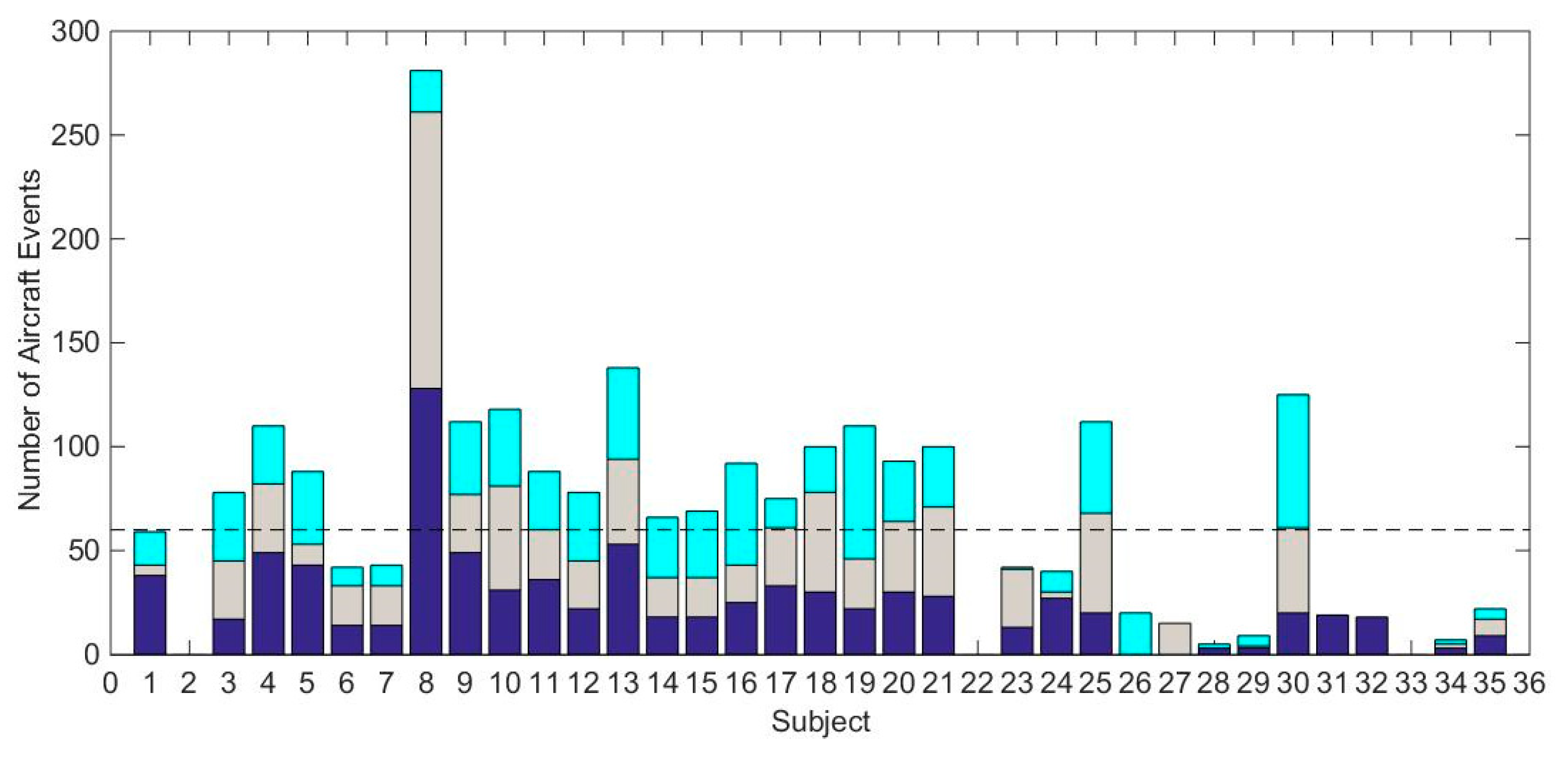
An exposure-response model relating the indoor noise level of the aircraft events to the probability of awakening inferred from body movements and ECG arousals was also derived. Awakening probability increased statistically significantly with LASmax of aircraft noise events both in the unadjusted model and in the model adjusted for age, sex, BMI, and elapsed sleep time. The number of aircraft events of high noise levels was low in this study, as shown by the skewed distribution of noise levels. In addition, the total number of aircraft events contributing to this analysis was only approximately 2000. These two limitations led to a wide confidence interval for the estimated awakening probability.
The long-term goal of this line of research is to derive exposure-response relationships that are representative for the US population exposed to nocturnal aircraft noise. This study was the first step in evaluating the feasibility of a study methodology for collecting unattended physiological and noise data to develop these models. Based on experiences in this study, further refinements of the protocol are needed. The target enrollment of 80 participants for the study was met, however, to recruit the participants, 3700 flyers were mailed. This low response rate limits the generalizability of the results. One contributing factor to the low response rate may be that, while the measurements took place unattended, staff members still had to enter participants’ homes to setup and collect the equipment. A website was created with information on the study which allowed individuals to verify both the study and study team. The link for the website was provided on the recruitment flyers. However, despite the website and the provided information, potential participants may still have been reluctant to allow unknown individuals into their home.
Another limitation of the study design was the methodological expense. This study required staff to be in the field from 2 to 4 days per week. If a multi-airport field study was conducted this way, trained staff would be required close to each of the measurement sites, which may not be feasible. In addition, the sound recording equipment used for this study cost several thousand dollars, which restricts the number of devices that can be purchased or available for use, restricts the number of sites that can be studied concurrently, and thus, also limits the sample size for the study. For this study, we had equipment to study three sites concurrently, which meant a minimum of 27 weeks of field work.
Visual identification of aircraft noise and other events was cumbersome and also requires trained staff. We made important progress in automatically identifying aircraft noise events based on sound level measurements and flight-track data. However, aircraft noise events were often masked by other indoor noise sources, especially air conditioning units. These masked aircraft noise events had to be excluded form data analysis. This needs to be taken into account for sample size analyses for future field studies in the US.
Finally, inferring awakenings from changes in heart rate and body movements has several advantages including the low methodological expense, the possibility of self-instrumentation, automatic analysis, and low invasiveness. However, the approach does not allow for a classification of sleep in stages, and therefore, an investigation of the effects of noise on sleep architecture. With the ongoing development and miniaturization of EEG technology, it may be possible to reliably measure the EEG with similar properties to the methodology used in our study in the future.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}