Adolescent Socioeconomic Status and Mental Health Inequalities in the Netherlands, 2001–2017


Abstract
:1. Introduction
1.1. Associations between SES Indicators and Adolescent Mental Health Problems
1.2. A Moderating Role for Adolescent Subjective SES and Adolescent Educational Level?
1.3. Changes in Socioeconomic Inequalities in Adolescent Mental Health
- To what extent are three SES indicators—parental SES, adolescent subjective SES and adolescent educational level—independently associated with adolescent mental health problems?
- To what extent is the association between parental SES and adolescent mental health problems moderated by adolescent subjective SES and adolescent educational level?
- To what extent have the associations between three SES indicators, their interplay and adolescent mental health problems changed between 2001 and 2017?
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Socioeconomic Status Indicators
2.2.2. Adolescent Mental Health Problems
2.2.3. Other Variables
2.3. Strategy of Analyses
3. Results
3.1. Descriptive Statistics
3.2. Associations between Three SES Indicators and Adolescent Mental Health Problems
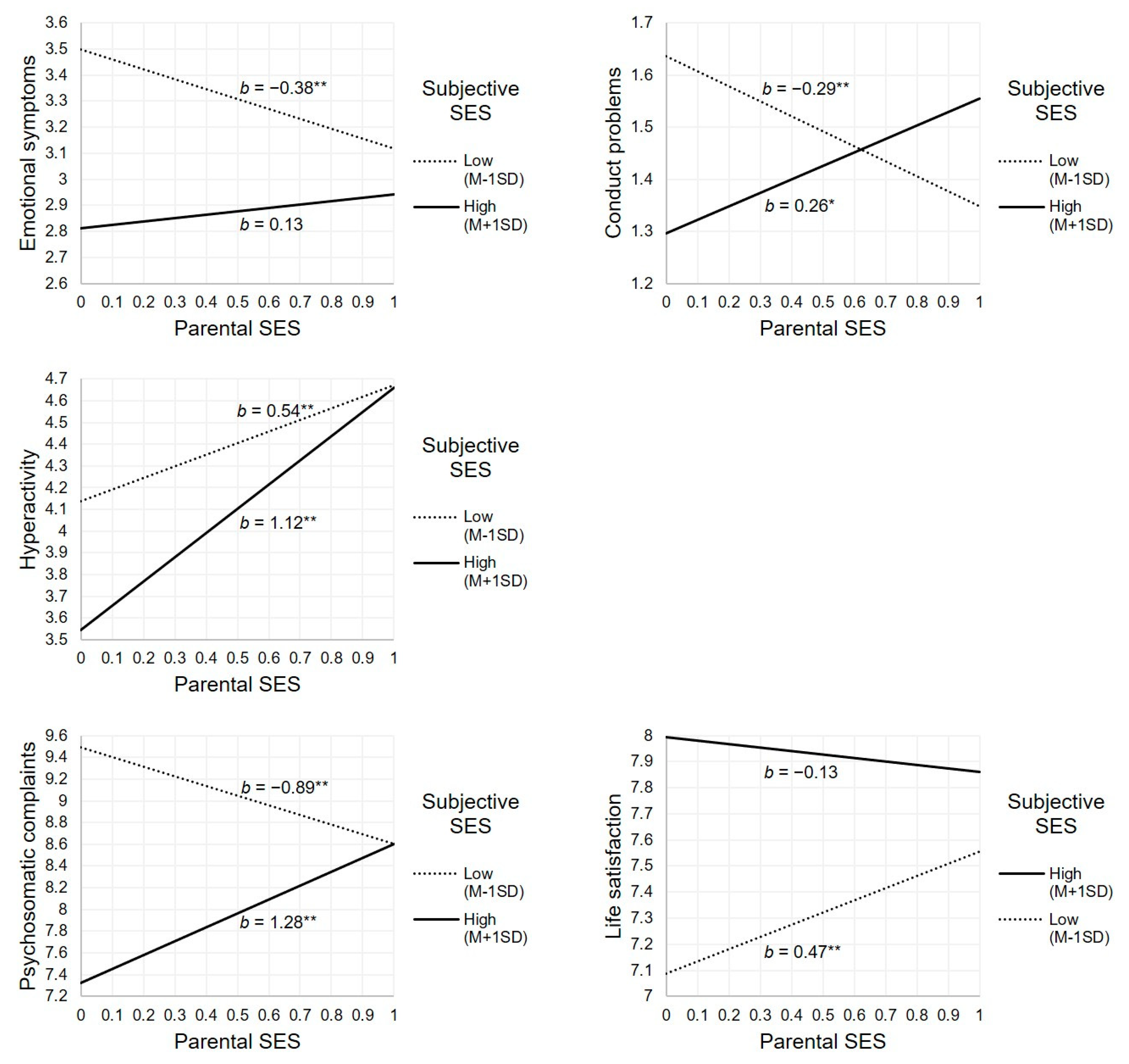
3.3. Moderation Effects of Adolescent Subjective SES and Adolescent Educational Level
3.4. Changes in Socioeconomic Inequalities between 2001 and 2017
4. Discussion
4.1. Adolescent Subjective SES and Educational Level Associated with Mental Health Problems
4.2. Adolescent Subjective SES Buffers the Association between Low Parental SES and Adolescent Mental Health Problems
4.3. No Changes in Socioeconomic Inequalities in Adolescent Mental Health
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Elgar, F.J.; Pförtner, T.K.; Moor, I.; De Clercq, B.; Stevens, G.W.J.M.; Currie, C. Socioeconomic Inequalities in Adolescent Health 2002–2010: A Time-Series Analysis of 34 Countries Participating in the Health Behaviour in School-Aged Children Study. Lancet 2015, 385, 2088–2095. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.; Torsheim, T.; Augustson, L.; Mathison, F.; Aleman-Diaz, A.Y.; Molcho, M.; Weber, M.W.; et al. Growing up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being: Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Reiss, F. Socioeconomic Inequalities and Mental Health Problems in Children and Adolescents: A Systematic Review. Soc. Sci. Med. 2013, 90, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Conger, R.D.; Conger, K.J.; Martin, M.J. Socioeconomic Status, Family Processes, and Individual Development. J. Marriage Fam. 2010, 72, 685–704. [Google Scholar] [CrossRef] [PubMed]
- Devenish, B.; Hooley, M.; Mellor, D. The Pathways between Socioeconomic Status and Adolescent Outcomes: A Systematic Review. Am. J. Community Psychol. 2017, 59, 219–238. [Google Scholar] [CrossRef] [PubMed]
- Koivusilta, L.; Rimpelä, A.; Kautiainen, S. Health Inequality in Adolescence. Does Stratification Occur by Familial Social Background, Family Affluence, or Personal Social Position? BMC Public Health 2006, 6, 110. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; Costello, E.J.; Leblanc, W.; Sampson, N.A.; Kessler, R.C. Socioeconomic Status and Adolescent Mental Disorders. Am. J. Public Health 2012, 102, 1742–1750. [Google Scholar] [CrossRef] [PubMed]
- Quon, E.C.; McGrath, J.J. Subjective Socioeconomic Status and Adolescent Health: A Meta-Analysis. Health Psychol. 2014, 33, 433–447. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Valverde, J.R.; Artnik, B.; Bopp, M.; Brønnum-Hansen, H.; Deboosere, P.; Kalediene, R.; Kovács, K.; Leinsalu, M.; Martikainen, P.; et al. Trends in Health Inequalities in 27 European Countries. Proc. Natl. Acad. Sci. USA 2018, 115, 6440–6445. [Google Scholar] [CrossRef]
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our Future: A Lancet Commission on Adolescent Health and Wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef]
- Pförtner, T.K.; Elgar, F.J.; Rathmann, K.; Richter, M. The Great Recession, Health, and Health Inequalities in Adolescents in North America, Europe, and Israel. In Young People’s Development and the Great Recession; Schoon, I., Bynner, J., Eds.; Cambridge University Press: Cambridge, UK, 2017; pp. 401–424. [Google Scholar] [CrossRef]
- Hagquist, C. Health Inequalities among Adolescents—the Impact of Academic Orientation and Parents’ Education. Eur. J. Public Health 2007, 17, 21–26. [Google Scholar] [CrossRef]
- Havas, J.; Bosma, H.; Spreeuwenberg, C.; Feron, F.J. Mental Health Problems of Dutch Adolescents: The Association with Adolescents’ and Their Parents’ Educational Level. Eur. J. Public Health 2010, 20, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Grant, K.E.; Compas, B.E.; Stuhlmacher, A.F.; Thurm, A.E.; McMahon, S.D.; Halpert, J.A. Stressors and Child and Adolescent Psychopathology: Moving from Markers to Mechanisms of Risk. Psychol. Bull. 2003, 129, 447–466. [Google Scholar] [CrossRef] [PubMed]
- Odgers, C.L. Income Inequality and the Developing Child: Is It All Relative? Am. Psychol. 2015, 70, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.G. Health, Hierarchy, and Social Anxiety. Ann. N. Y. Acad. Sci. 1999, 896, 48–63. [Google Scholar] [CrossRef] [PubMed]
- Festinger, L. A Theory of Social Comparison Processes. Hum. Relat. 1954, 7, 117–140. [Google Scholar] [CrossRef]
- Goodman, E.; Adler, N.E.; Kawachi, I.; Frazier, A.L.; Huang, B.; Colditz, G.A. Adolescents’ Perceptions of Social Status: Development and Evaluation of a New Indicator. Pediatrics 2001, 108, e31. [Google Scholar] [CrossRef] [PubMed]
- Hoebel, J.; Lampert, T. Subjective Social Status and Health: Multidisciplinary Explanations and Methodological Challenges. J. Health Psychol. 2018. [Google Scholar] [CrossRef]
- Smith, H.J.; Pettigrew, T.F.; Pippin, G.M.; Bialosiewicz, S. Relative Deprivation: A Theoretical and Meta-Analytic Review. Personal. Soc. Psychol. Rev. 2012, 16, 203–232. [Google Scholar] [CrossRef]
- Taylor, S.E.; Seeman, T.E. Psychosocial Resources and the SES-Health Relationship. Ann. N. Y. Acad. Sci. 1999, 896, 210–225. [Google Scholar] [CrossRef]
- Schoon, I.; Lyons-Amos, M. A Socio-Ecological Model of Agency: The Role of Psycho-Social and Socioeconomic Resources in Shaping Education and Employment Transitions in England. Longitud. Life Course Stud. 2017, 8, 35–56. [Google Scholar] [CrossRef]
- Antaramian, S.P.; Huebner, E.S.; Hills, K.J.; Valois, R.F. A Dual-factor Model of Mental Health: Toward a More Comprehensive Understanding of Youth Functioning. Am. J. Orthopsychiatry 2010, 80, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Dishion, T.J.; Tipsord, J.M. Peer Contagion in Child and Adolescent Social and Emotional Development. Annu. Rev. Psychol. 2011, 62, 189–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, G.R.; DeBaryshe, B.D.; Ramsey, E. A Developmental Perspective on Antisocial Behavior. Am. Psychol. 1989, 44, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Veed, G.J.; McGinley, M.; Crockett, L.J. Friendship Network Influence on the Development of Internalizing Symptoms during Adolescence. J. Appl. Dev. Psychol. 2019, 60, 157–165. [Google Scholar] [CrossRef]
- Goodman, E.; Huang, B.; Schafer-Kalkhoff, T.; Adler, N.E. Perceived Socioeconomic Status: A New Type of Identity That Influences Adolescents’ Self-Rated Health. J. Adolesc. Health 2007, 41, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Pförtner, T.K.; Günther, S.; Levin, K.A.; Torsheim, T.; Richter, M. The Use of Parental Occupation in Adolescent Health Surveys. An Application of ISCO-Based Measures of Occupational Status. J. Epidemiol. Community Health 2015, 69, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Svedberg, P.; Nygren, J.M.; Staland-Nyman, C.; Nyholm, M. The Validity of Socioeconomic Status Measures among Adolescents Based on Self-Reported Information about Parents Occupations, FAS and Perceived SES; Implication for Health Related Quality of Life Studies. BMC Med. Res. Methodol. 2016, 16, 48. [Google Scholar] [CrossRef]
- Moreno-Maldonado, C.; Rivera, F.; Ramos, P.; Moreno, C. Measuring the Socioeconomic Position of Adolescents: A Proposal for a Composite Index. Soc. Indic. Res. 2018, 136, 517–538. [Google Scholar] [CrossRef]
- Moor, I.; Lampert, T.; Rathmann, K.; Kuntz, B.; Kolip, P.; Spallek, J.; Richter, M. Explaining Educational Inequalities in Adolescent Life Satisfaction: Do Health Behaviour and Gender Matter? Int. J. Public Health 2014, 59, 309–317. [Google Scholar] [CrossRef]
- Klanšček, H.J.; Žiberna, J.; Korošec, A.; Zurc, J.; Albreht, T. Mental Health Inequalities in Slovenian 15-Year-Old Adolescents Explained by Personal Social Position and Family Socioeconomic Status. Int. J. Equity Health 2014, 13, 26. [Google Scholar] [CrossRef]
- Mackenbach, J.P. The Persistence of Health Inequalities in Modern Welfare States: The Explanation of a Paradox. Soc. Sci. Med. 2012, 75, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.E.; Mirowsky, J. The Interaction of Personal and Parental Education on Health. Soc. Sci. Med. 2011, 72, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.A. Health Returns to Education by Family Socioeconomic Origins, 1980–2008: Testing the Importance of Gender, Cohort, and Age. SSM Popul. Health 2016, 2, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Destin, M. Socioeconomic Mobility, Identity, and Health: Experiences That Influence Immunology and Implications for Intervention. Am. Psychol. 2019, 74, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.E.; Richeson, J.A.; Finkel, E.J. Middle Class and Marginal? Socioeconomic Status, Stigma, and Self-Regulation at an Elite University. J. Personal. Soc. Psychol. 2011, 100, 838–852. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.S.; Saucier, D.A.; Hafner, E. Meta-Analysis of the Relationships between Social Support and Well-Being in Children and Adolescents. J. Soc. Clin. Psychol. 2010, 29, 624–645. [Google Scholar] [CrossRef]
- Sweeting, H.; West, P.; Young, R.; Der, G. Can We Explain Increases in Young People’s Psychological Distress over Time? Soc. Sci. Med. 2010, 71, 1819–1830. [Google Scholar] [CrossRef]
- Ashton, D.N. Globalization and Its Impact on the Political, Economic, and Labor Market Aspects of the Transition. In Young People’s Development and the Great Recession; Schoon, I., Bynner, J., Eds.; Cambridge University Press: Cambridge, UK, 2017; pp. 25–51. [Google Scholar] [CrossRef]
- Kalil, A. Effects of the Great Recession on Child Development. Ann. Am. Acad. Pol. Soc. Sci. 2013, 650, 232–250. [Google Scholar] [CrossRef] [Green Version]
- Centraal Bureau voor de Statistiek (CBS). VO; Leerlingen, Onderwijssoort in Detail, Leerjaar. Available online: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/80040ned/table?dl=2527B (accessed on 26 August 2019).
- Onderwijsraad. Herkenbaar Vmbo Met Sterk Vakmanschap; Onderwijsraad: The Hague, The Netherlands, 2015; Available online: https://www.onderwijsraad.nl/upload/documents/publicaties/volledig/Herkenbaar-vmbo-1.7.pdf (accessed on 26 August 2019).
- Timmermans, A.C.; de Boer, H.; Amsing, H.T.A.; van der Werf, M.P.C. Track Recommendation Bias: Gender, Migration Background and SES Bias over a 20-Year Period in the Dutch Context. Br. Educ. Res. J. 2018, 44, 847–874. [Google Scholar] [CrossRef]
- Peter, J.; Valkenburg, P.M. Adolescents’ Internet Use: Testing the “Disappearing Digital Divide” versus the “Emerging Digital Differentiation” Approach. Poetics 2006, 34, 293–305. [Google Scholar] [CrossRef]
- Van Deursen, A.J.A.M.; Helsper, E.J. The Third-Level Digital Divide: Who Benefits Most from Being Online? In Studies in Media and Communications; Robinson, L., Cotten, S.R., Schulz, J., Hale, T.M., Williams, A., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2015; Volume 10, pp. 29–52. [Google Scholar] [CrossRef]
- Odgers, C.L. Smartphones Are Bad for Some Adolescents, Not All. Nature 2018, 554, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Moor, I.; Richter, M.; Ravens-Sieberer, U.; Ottová-Jordan, V.; Elgar, F.J.; Pförtner, T.K. Trends in Social Inequalities in Adolescent Health Complaints from 1994 to 2010 in Europe, North America and Israel: The HBSC Study. Eur. J. Public Health 2015, 25, 57–60. [Google Scholar] [CrossRef]
- Duinhof, E.L.; Stevens, G.W.J.M.; van Dorsselaer, S.; Monshouwer, K.; Vollebergh, W.A.M. Ten-Year Trends in Adolescents’ Self-Reported Emotional and Behavioral Problems in the Netherlands. Eur. Child Adolesc. Psychiatry 2015, 24, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Van Vuuren, C.L.; Uitenbroek, D.G.; van der Wal, M.F.; Chinapaw, M.J.M. Sociodemographic Differences in 10-Year Time Trends of Emotional and Behavioural Problems among Adolescents Attending Secondary Schools in Amsterdam, The Netherlands. Eur. Child Adolesc. Psychiatry 2018, 27, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Frasquilho, D.; Matos, M.G.; Salonna, F.; Guerreiro, D.; Storti, C.C.; Gaspar, T.; Caldas-de-Almeida, J.M. Mental Health Outcomes in Times of Economic Recession: A Systematic Literature Review. BMC Public Health 2016, 16, 115. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Subramanian, S.V. Social Epidemiology for the 21st Century. Soc. Sci. Med. 2018, 196, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.W.J.M.; van Dorsselaer, S.; Boer, M.; de Roos, S.; Duinhof, E.L.; Ter Bogt, T.; Van Den Eijnden, R.J.J.M.; Kuyper, L.; Visser, D.; Vollebergh, W.A.M.; et al. HBSC 2017: Gezondheid En Welzijn van Jongeren in Nederland; Utrecht University: Utrecht, The Netherlands, 2018. [Google Scholar]
- Inchley, J.; Currie, D.; Cosma, A.; Piper, A.; Spanou, G. (Eds.) Health Behaviour in School-Aged Children (HBSC) Internal Protocol 2017/18; CAHRU: St Andrews, UK, 2017. [Google Scholar]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching Health Inequalities in Adolescents: The Development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Boyce, W.; Torsheim, T.; Currie, C.; Zambon, A. The Family Affluence Scale as a Measure of National Wealth: Validation of an Adolescent Self-Report Measure. Soc. Indic. Res. 2006, 78, 473–487. [Google Scholar] [CrossRef]
- Elgar, F.J.; Xie, A.; Pförtner, T.K.; White, J.; Pickett, K.E. Assessing the View from Bottom: How to Measure Socioeconomic Position and Relative Deprivation in Adolescents; SAGE Publications Ltd.: London, UK, 2017. [Google Scholar] [CrossRef]
- Hartley, J.E.K.; Levin, K.; Currie, C. A New Version of the HBSC Family Affluence Scale—FAS III: Scottish Qualitative Findings from the International FAS Development Study. Child Indic. Res. 2016, 9, 233–245. [Google Scholar] [CrossRef]
- Schnohr, C.W.; Makransky, G.; Kreiner, S.; Torsheim, T.; Hofmann, F.; De Clercq, B.; Elgar, F.J.; Currie, C. Item Response Drift in the Family Affluence Scale: A Study on Three Consecutive Surveys of the Health Behaviour in School-Aged Children (HBSC) Survey. Measurement 2013, 46, 3119–3126. [Google Scholar] [CrossRef]
- Huppert, F.A.; Whittington, J.E. Evidence for the Independence of Positive and Negative Well-Being: Implications for Quality of Life Assessment. Br. J. Health Psychol. 2003, 8, 107–122. [Google Scholar] [CrossRef] [PubMed]
- Duinhof, E.L.; Lek, K.M.; de Looze, M.E.; Cosma, A.; Mazur, J.; Gobina, I.; Wüstner, A.; Vollebergh, W.A.M.; Stevens, G.W.J.M. Revising the Self-Report Strengths and Difficulties Questionnaire for Cross-Country Comparisons of Adolescent Mental Health Problems: The SDQ-R. Epidemiol. Psychiatr. Sci. 2019, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Youthinmind. Downloadable SDQs and Related Items. Available online: http://www.sdqinfo.org/py/sdqinfo/b0.py (accessed on 26 August 2019).
- Essau, C.A.; Olaya, B.; Anastassiou-Hadjicharalambous, X.; Pauli, G.; Gilvarry, C.; Bray, D.; O’callaghan, J.; Ollendick, T.H. Psychometric Properties of the Strength and Difficulties Questionnaire from Five European Countries. Int. J. Methods Psychiatr. Res. 2012, 21, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U.; Erhart, M.; Torsheim, T.; Hetland, J.; Freeman, J.; Danielson, M.; Thomas, C. An International Scoring System for Self-Reported Health Complaints in Adolescents. Eur. J. Public Health 2008, 18, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Gariépy, G.; Elgar, F.J. Trends in Psychological Symptoms among Canadian Adolescents from 2002 to 2014: Gender and Socioeconomic Differences. Can. J. Psychiatry 2016, 61, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantril, H. Pattern of Human Concerns; Rutgers University Press: New Brunswick, NJ, USA, 1965. [Google Scholar]
- Levin, K.A.; Currie, C. Reliability and Validity of an Adapted Version of the Cantril Ladder for Use with Adolescent Samples. Soc. Indic. Res. 2014, 119, 1047–1063. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Ahlborg, M.; Svedberg, P.; Nyholm, M.; Morgan, A.; Nygren, J.M. Socioeconomic Inequalities in Health among Swedish Adolescents—Adding the Subjective Perspective. BMC Public Health 2017, 17, 838. [Google Scholar] [CrossRef]
- Buijs, T.; Maes, L.; Salonna, F.; Van Damme, J.; Hublet, A.; Kebza, V.; Costongs, C.; Currie, C.; De Clercq, B. The Role of Community Social Capital in the Relationship between Socioeconomic Status and Adolescent Life Satisfaction: Mediating or Moderating? Evidence from Czech Data. Int. J. Equity Health 2016, 15, 203. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, S.; Rahkonen, O. Subjective Social Status and Health in Young People. Sociol. Health Illn. 2011, 33, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.P.; Porter, M.R.; McFarland, F.C.; Marsh, P.; McElhaney, K.B. The Two Faces of Adolescents’ Success with Peers: Adolescent Popularity, Social Adaptation, and Deviant Behavior. Child Dev. 2005, 76, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Garbarski, D. Perceived Social Position and Health: Is There a Reciprocal Relationship? Soc. Sci. Med. 2010, 70, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Nobles, J.; Ritterman Weintraub, M.; Adler, N. Subjective Socioeconomic Status and Health: Relationships Reconsidered. Soc. Sci. Med. 2013, 82, 58–66. [Google Scholar] [CrossRef]
- Kraus, M.W.; Adler, N.; Chen, T.W.D. Is the Association of Subjective SES and Self-Rated Health Confounded by Negative Mood? An Experimental Approach. Health Psychol. 2013, 32, 138–145. [Google Scholar] [CrossRef] [PubMed]
- De Zeeuw, E.L.; van Beijsterveldt, C.E.M.; Ehli, E.A.; de Geus, E.J.C.; Boomsma, D.I. Attention Deficit Hyperactivity Disorder Symptoms and Low Educational Achievement: Evidence Supporting a Causal Hypothesis. Behav. Genet. 2017, 47, 278–289. [Google Scholar] [CrossRef]
- Elstad, J.I. Indirect Health-Related Selection or Social Causation? Interpreting the Educational Differences in Adolescent Health Behaviours. Soc. Theory Health 2010, 8, 134–150. [Google Scholar] [CrossRef]
- Halpern-Manners, A.; Schnabel, L.; Hernandez, E.M.; Silberg, J.L.; Eaves, L.J. The Relationship between Education and Mental Health: New Evidence from a Discordant Twin Study. Soc. Forces 2016, 95, 107–131. [Google Scholar] [CrossRef]
- Sweeting, H.; Green, M.; Benzeval, M.; West, P. The Emergence of Health Inequalities in Early Adulthood: Evidence on Timing and Mechanisms from a West of Scotland Cohort. BMC Public Health 2016, 16, 41. [Google Scholar] [CrossRef]
- Davidovitch, M.; Koren, G.; Fund, N.; Shrem, M.; Porath, A. Challenges in Defining the Rates of ADHD Diagnosis and Treatment: Trends over the Last Decade. BMC Pediatrics 2017, 17, 218. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.E.; Ford, T.; Williams, R.; Russell, G. The Association between Socioeconomic Disadvantage and Attention Deficit/Hyperactivity Disorder (ADHD): A Systematic Review. Child Psychiatry Hum. Dev. 2016, 47, 440–458. [Google Scholar] [CrossRef] [PubMed]
- Willcutt, E.G. The Prevalence of DSM-IV Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, K.A.; Gallo, L.C. Psychological Perspectives on Pathways Linking Socioeconomic Status and Physical Health. Annu. Rev. Psychol. 2011, 62, 501–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piko, B.F.; Luszczynska, A.; Fitzpatrick, K.M. Social Inequalities in Adolescent Depression: The Role of Parental Social Support and Optimism. Int. J. Soc. Psychiatry 2013, 59, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, D.; Stevens, G.W.J.M.; Finkenauer, C.; Brunekreef, B.; Smit, H.A.; Wijga, A.H. The Pathways from Parental and Neighbourhood Socioeconomic Status to Adolescent Educational Attainment: An Examination of the Role of Cognitive Ability, Teacher Assessment, and Educational Expectations. PLoS ONE 2019, 14, e0216803. [Google Scholar] [CrossRef] [PubMed]
- Mulder, E.F.J.D.; Pater, B.C.D.; Fortuijn, J.C.D. The Netherlands and the Dutch: A Physical and Human Geography; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the Social Determinants of Health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]


{kind=link}
| Range | 2001 | 2005 | 2009 | 2013 | 2017 | Total | Total n | |
|---|---|---|---|---|---|---|---|---|
| Parental SES (M/SD) | 0–1 | 0.5 (0.3) | 0.5 (0.3) | 0.5 (0.3) | 0.5 (0.3) | 0.5 (0.3) | 0.5 (0.3) | 27,020 |
| Subjective SES (M/SD) | 1–5 | 3.3 (0.7) | 3.1 (0.7) | 3.2 (0.7) | 3.1 (0.8) | 3.2 (0.7) | 3.2 (0.7) | 27,020 |
| Low Educational Level (%) | 23.5 | 26.0 | 17.8 | 23.3 | 18.0 | 21.6 | 27,020 | |
| Lower Int. Educational Level (%) | 35.4 | 31.5 | 35.5 | 27.1 | 32.3 | 32.4 | 27,020 | |
| Upper Int. Educational Level (%) | 23.1 | 24.4 | 22.9 | 26.8 | 23.1 | 24.0 | 27,020 | |
| High Educational Level (%) | 18.0 | 18.1 | 23.8 | 22.8 | 26.5 | 22.0 | 27,020 | |
| Emotional Symptoms (M/SD) | 0–10 | 2.2 (2.1) | 2.2 (2.1) | 2.6 (2.3) | 2.5 (2.3) | 2.4 (2.2) | 21,503 | |
| Conduct Problems (M/SD) | 0–10 | 1.3 (1.8) | 1.1 (1.7) | 1.2 (1.7) | 1.2 (1.7) | 1.2 (1.7) | 21,480 | |
| Hyperactivity (M/SD) | 0–10 | 3.6 (2.8) | 3.9 (2.9) | 4.1 (3.0) | 4.1 (3.0) | 4.0 (2.9) | 21,518 | |
| Peer Problems (M/SD) | 0–10 | 1.7 (1.9) | 1.7 (2.0) | 1.8 (2.0) | 1.9 (2.0) | 1.8 (2.0) | 21,484 | |
| Psychosomatic Complaints (M/SD) | 0–32 | 6.6 (5.6) | 5.6 (5.8) | 6.5 (5.6) | 7.9 (6.4) | 7.9 (6.5) | 6.9 (6.1) | 26,813 |
| Life Satisfaction (M/SD) | 0–10 | 7.9 (1.6) | 7.7 (1.6) | 7.9 (1.4) | 7.6 (1.6) | 7.6 (1.6) | 7.7 (1.6) | 26,729 |
| Variables | 2 | 3 | 4 | 5 | 6 b | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | 1. Age | 0.02 | −0.03 ** | −0.06 ** | −0.05 ** | −0.10 ** | 0.06 ** | 0.02 * | 0.05 ** | 0.07 ** | 0.06 ** | −0.15 ** |
| 2. Gender a | −0.01 | 0.10 ** | 0.11 ** | −0.01 | −0.31 ** | 0.12 ** | 0.01 | 0.03 ** | −0.22 ** | 0.14 ** | ||
| Time | 3. Survey Year | 0.00 | −0.03 ** | 0.08 ** | 0.06 ** | −0.01 | 0.07 ** | 0.03 ** | 0.12 ** | −0.08 ** | ||
| SES | 4. Parental SES | 0.38 ** | 0.21 ** | −0.09 ** | −0.04 ** | 0.03 ** | −.11 ** | −0.05 ** | 0.12 ** | |||
| 5. Adol. Subjective SES | 0.11 ** | −0.14 ** | −0.04 ** | −0.04 ** | −0.08 ** | −0.12 ** | 0.23 ** | |||||
| 6. Adol. Educ. Level b | −0.02 ** | −0.20 ** | −0.11 ** | −0.15 ** | −0.01 | 0.01 | ||||||
| Adol. Mental Health Problems | 7. Emotional Symptoms | 0.28 ** | 0.29 ** | 0.35 ** | 0.63 ** | −0.46 ** | ||||||
| 8. Conduct Problems | 0.33 ** | 0.29 ** | 0.31 ** | −0.23 ** | ||||||||
| 9. Hyperactivity | 0.11 ** | 0.31 ** | −0.19 ** | |||||||||
| 10. Peer Problems | 0.26 ** | −0.23 ** | ||||||||||
| 11. Psychosomatic Complaints | −0.45 ** | |||||||||||
| 12. Life Satisfaction |
| Emotional Symptoms | Conduct Problems | Hyperactivity | Peer Problems | Psychosomatic Complaints | Life Satisfaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B (SE) | β | B (SE) | β | B (SE) | β | B (SE) | β | B (SE) | β | B (SE) | β | ||
| M1 | Intercept | 1.67 ** (0.18) | 0.00 | 0.57 ** (0.17) | 0.01 | 2.50 ** (0.29) | 0.00 | 0.26 (0.18) | 0.00 | 4.29 ** (0.49) | 0.00 | 10.14 ** (0.12) | 0.00 |
| Gender (girls = ref) | −1.39 ** (0.03) | −0.31 | 0.43 ** (0.03) | 0.12 | 0.08 (0.04) | 0.01 | 0.14 ** (0.03) | 0.04 | −2.71 ** (0.08) | −0.22 | 0.44 ** (0.02) | 0.14 | |
| Age | 0.10 ** (0.01) | 0.06 | 0.03 (0.01) | 0.02 | 0.10 ** (0.02) | 0.04 | 0.11 ** (0.01) | 0.07 | 0.29 ** (0.04) | 0.06 | −0.19 ** (0.01) | −0.15 | |
| M2a | Parental SES | −0.43 ** (0.06) | −0.06 | −0.36 ** (0.05) | −0.06 | 0.33 * (0.10) | 0.03 | −0.80 ** (0.06) | −0.11 | −0.66 ** (0.16) | −0.03 | 0.55 ** (0.04) | 0.10 |
| M2b | Adol. Subjective SES | −0.33 ** (0.02) | −0.11 | −0.12 ** (0.02) | −0.05 | −0.16 ** (0.03) | −0.04 | −0.22 ** (0.02) | −0.08 | −0.77 ** (0.06) | −0.09 | 0.44 ** (0.02) | 0.21 |
| M2c | Educ. = High | −0.19 (0.06) | −0.08 | −0.98 ** (0.05) | −0.57 | −0.88 ** (0.09) | −0.30 | −0.78 ** (0.05) | −0.40 | −0.71 * (0.20) | −0.12 | 0.07 (0.04) | 0.05 |
| Educ. = Upper Int. | −0.08 (0.06) | −0.04 | −0.69 ** (0.05) | −0.40 | −0.29 * (0.10) | −0.10 | −0.56 ** (0.05) | −0.29 | −0.54 (0.19) | −0.09 | −0.02 (0.04) | −0.02 | |
| Educ. = Lower Int. | −0.12 (0.06) | −0.05 | −0.37 ** (0.05) | −0.21 | −0.10 (0.09) | −0.03 | −0.27 ** (0.06) | −0.13 | −0.37 (0.18) | −0.06 | −0.04 (0.04) | −0.03 | |
| M3 | Parental SES | −0.12 (0.06) | −0.02 | −0.01 (0.05) | 0.00 | 0.83 ** (0.10) | 0.08 | −0.49 ** (0.06) | −0.07 | 0.25 (0.16) | 0.01 | 0.15 * (0.04) | 0.03 |
| Adol. Subjective SES | −0.31 ** (0.03) | −0.10 | −0.06 (0.02) | −0.02 | −0.22 ** (0.03) | −0.05 | −0.11 ** (0.02) | −0.04 | −0.78 ** (0.07) | −0.09 | 0.42 ** (0.02) | 0.20 | |
| Educ. = High | −0.09 (0.07) | −0.04 | −0.97 ** (0.05) | −0.56 | −0.98 ** (0.08) | −0.34 | −0.66 ** (0.05) | −0.034 | −0.57 (0.20) | −0.09 | −0.05 (0.04) | −0.03 | |
| Educ. = Upper Int. | −0.03 (0.06) | −0.01 | −0.68 ** (0.05) | −0.39 | −0.37 ** (0.09) | −0.13 | −0.48 ** (0.05) | −0.25 | −0.48 (0.19) | −0.08 | −0.09 (0.04) | −0.06 | |
| Educ. = Lower Int. | −0.10 (0.06) | −0.04 | −0.37 ** (0.05) | −0.21 | −0.14 (0.09) | −0.05 | −0.23 ** (0.06) | −0.12 | −0.35 (0.18) | −0.06 | −0.07 (0.04) | −0.04 | |
| M4a | Parental SES × Adol. Subjective SES | 0.35 ** (0.08) | 0.03 | 0.37 ** (0.07) | 0.05 | 0.39 * (0.11) | 0.03 | 0.22 (0.08) | 0.02 | 1.48 ** (0.20) | 0.05 | −0.41 ** (0.05) | −0.05 |
| M4b | Parental SES × Educ. = High | −0.40 (0.18) | −0.05 | −0.25 (0.13) | −0.04 | −0.32 (0.23) | −0.03 | −0.42 (0.17) | −0.06 | 0.15 (0.49) | 0.01 | −0.05 (0.12) | −0.01 |
| Parental SES × Educ. = Upper Int. | −0.33 (0.18) | −0.04 | −0.12 (0.13) | −0.02 | −0.07 (0.24) | −0.01 | −0.29 (0.17) | −0.04 | 0.37 (0.49) | 0.02 | −0.16 (0.12) | −0.03 | |
| Parental SES × Educ. = LOWER Int. | −0.35 (0.18) | −0.04 | −0.17 (0.14) | −0.03 | 0.16 (0.23) | 0.02 | −0.39 (0.16) | −0.06 | 0.13 (0.48) | 0.01 | −0.12 (0.12) | −0.02 | |
| M5a | Survey Year | 0.12 ** (0.02) | 0.08 | −0.02 (0.02) | −0.02 | 0.20 ** (0.03) | 0.10 | 0.06 (0.02) | 0.04 | 0.50 ** (0.04) | 0.12 | −0.09 ** (0.01) | −0.08 |
| M5b | Year × Parental SES | −0.14 (0.05) | −0.03 | −0.05 (0.04) | −0.01 | 0.05 (0.09) | 0.01 | −0.13 (0.05) | −0.03 | 0.10 (0.12) | 0.01 | 0.02 (0.03) | 0.01 |
| Year × Adol. Subjective SES | −0.02 (0.02) | −0.01 | −0.05 (0.02) | −0.03 | −0.07 (0.03) | −0.02 | −0.03 (0.02) | −0.02 | −0.11 (0.04) | −0.02 | 0.00 (0.01) | 0.00 | |
| Year × Educ. = High | 0.05 (0.05) | 0.03 | 0.10 (0.04) | 0.08 | −0.06 (0.07) | −0.03 | 0.04 (0.05) | 0.03 | 0.06 (0.12) | 0.01 | 0.00 (0.03) | 0.00 | |
| Year × Educ. = Upper Int. | 0.06 (0.05) | 0.04 | 0.11 (0.04) | 0.09 | 0.01 (0.07) | 0.00 | 0.05 (0.04) | 0.04 | 0.26 (0.12) | 0.06 | −0.04 (0.03) | −0.03 | |
| Year × Educ. = Lower Int. | 0.04 (0.05) | 0.03 | 0.05 (0.04) | 0.05 | 0.00 (0.08) | 0.00 | 0.03 (0.05) | 0.02 | 0.08 (0.11) | 0.02 | −0.03 (0.03) | −0.03 | |
| M6a | Year × Parental SES × Adol. Subjective SES | −0.07 (0.07) | −0.01 | −0.01 (0.07) | 0.00 | −0.02 (0.09) | 0.00 | −0.01 (0.07) | 0.00 | −0.08 (0.13) | 0.00 | −0.01 (0.04) | 0.00 |
| M6b | Year × Parental SES × Educ. = High | 0.20 (0.16) | 0.04 | 0.06 (0.11) | 0.01 | 0.34 (0.19) | 0.05 | −0.04 (0.14) | −0.01 | 0.62 (0.34) | 0.04 | −0.04 (0.08) | −0.01 |
| Year × Parental SES Educ. = Upper Int. | 0.26 (0.16) | 0.05 | 0.20 (0.12) | 0.05 | 0.19 (0.21) | 0.03 | 0.13 (0.14) | 0.03 | 0.35 (0.34) | 0.02 | −0.03 (0.08) | −0.01 | |
| Year × Parental SES Educ. = Lower Int. | 0.06 (0.16) | 0.01 | −0.10 (0.12) | −0.02 | 0.03 (0.21) | 0.00 | −0.17 (0.12) | −0.03 | −0.22 (0.32) | −0.01 | 0.04 (0.08) | 0.01 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinberg, D.; Stevens, G.W.J.M.; Duinhof, E.L.; Finkenauer, C. Adolescent Socioeconomic Status and Mental Health Inequalities in the Netherlands, 2001–2017. Int. J. Environ. Res. Public Health 2019, 16, 3605. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193605
Weinberg D, Stevens GWJM, Duinhof EL, Finkenauer C. Adolescent Socioeconomic Status and Mental Health Inequalities in the Netherlands, 2001–2017. International Journal of Environmental Research and Public Health. 2019; 16(19):3605. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193605
Chicago/Turabian StyleWeinberg, Dominic, Gonneke W. J. M. Stevens, Elisa L. Duinhof, and Catrin Finkenauer. 2019. "Adolescent Socioeconomic Status and Mental Health Inequalities in the Netherlands, 2001–2017" International Journal of Environmental Research and Public Health 16, no. 19: 3605. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193605