Death Anxiety, Religious Doubt, and Depressive Symptoms across Race in Older Adults


Abstract
:1. Introduction
1.1. Death Anxiety and Depression
1.2. Religious Doubt, Death Anxiety, and Depression
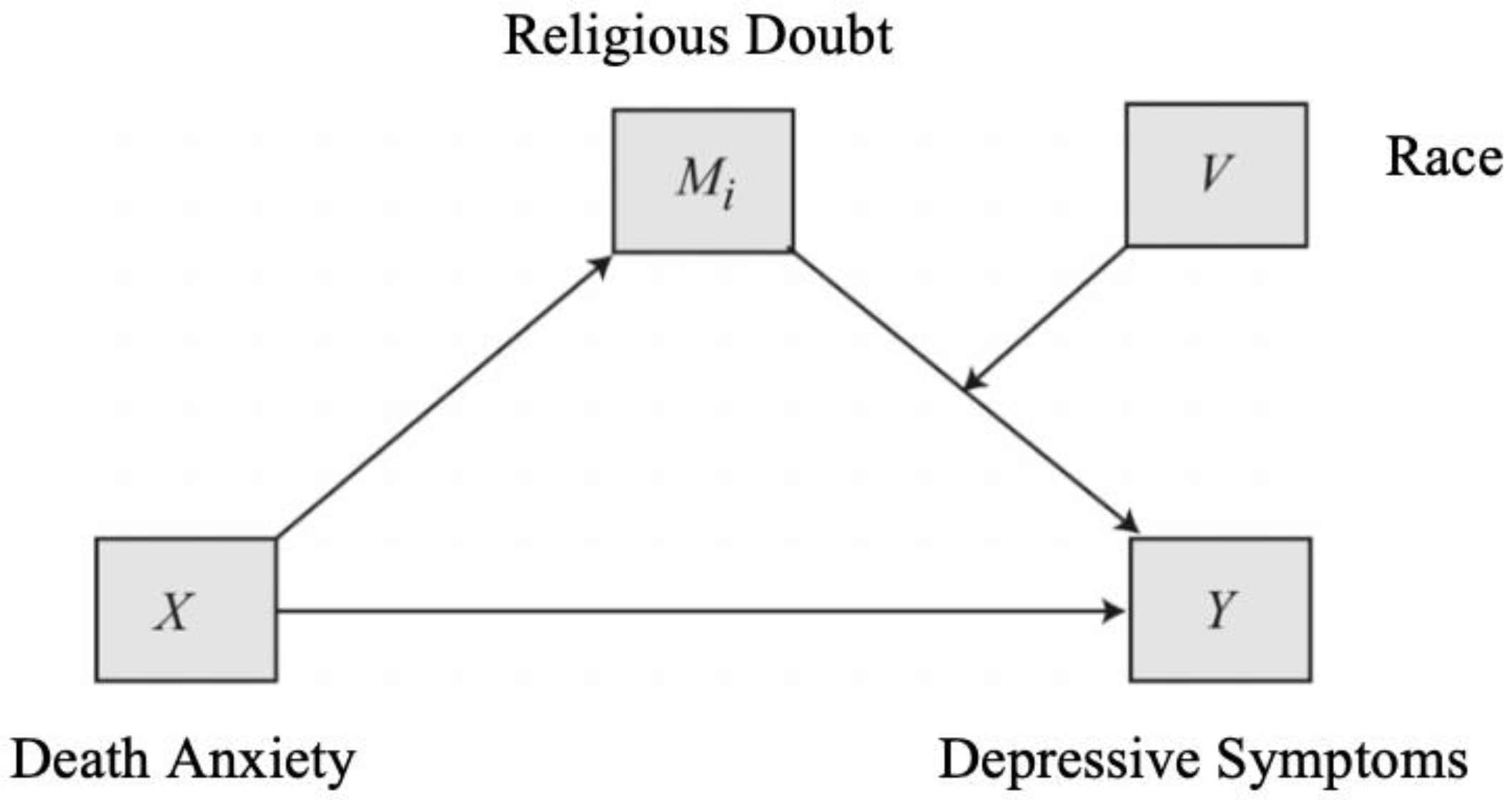
1.3. Consideration of Race
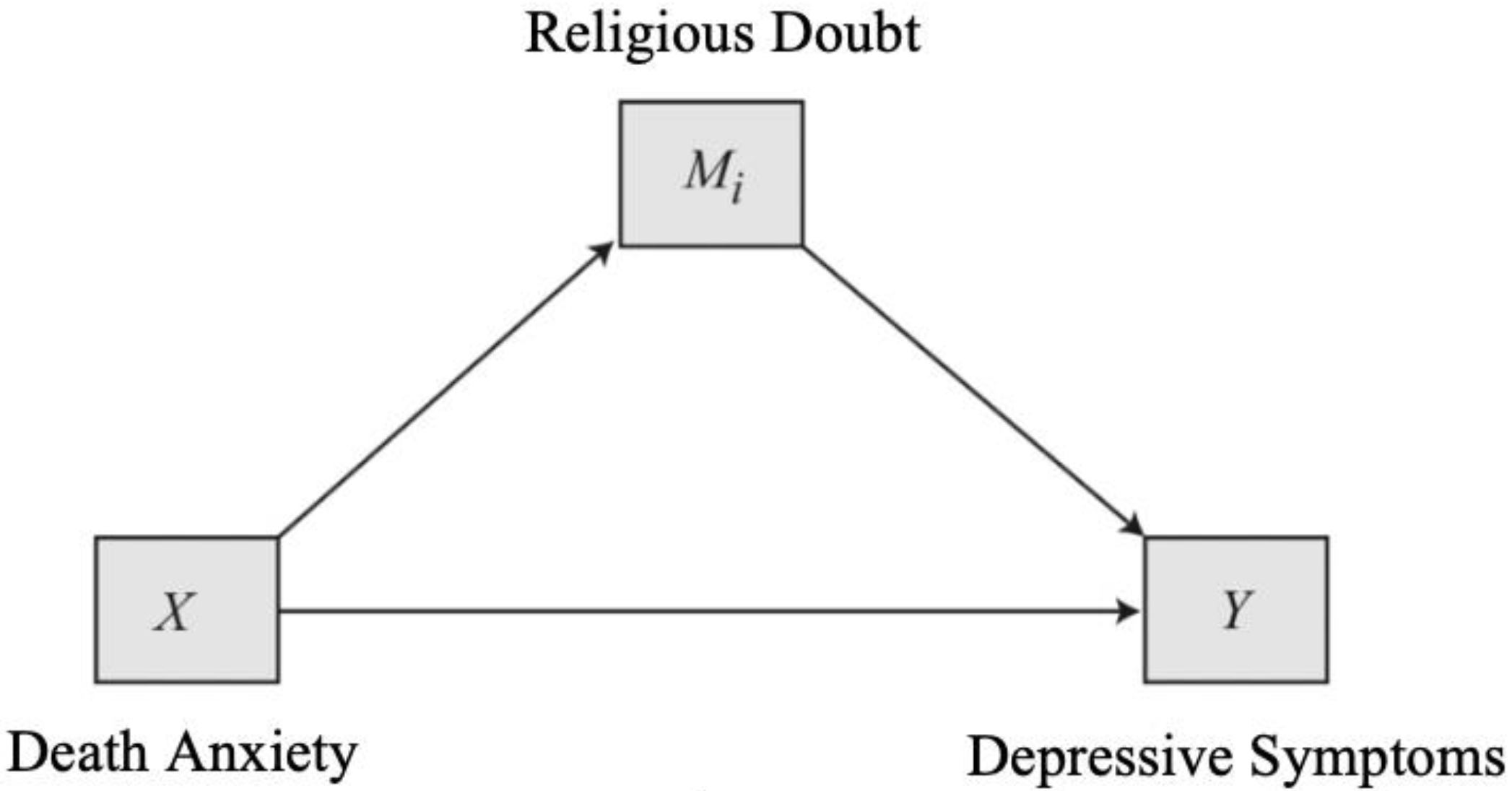
1.4. Current Study
2. Method
Participants and Procedures
3. Measures
3.1. Demographics
3.2. Religious Doubt
3.3. Death Anxiety
3.4. Depressive Symptoms
3.5. Rumination
3.6. Subjective Health
3.7. Data Analytic Plan
4. Results
4.1. Preliminary Results
4.2. Direct Effects
4.3. Indirect Effects
4.4. Moderated Indirect Effects
5. Discussion
Clinical Implications, Limitations, and Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mather, M.; Jacobsen, L.A.; Pollard, K.M. Population bulletin: Aging in the United States. Popul. Ref. Bur. 2015, 70, 1–5. [Google Scholar]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in older adults. Ann. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef] [PubMed]
- Blazer, D.G. Depression in late life: Review and commentary. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 58, 249–265. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Schimmele, C.M.; Chappell, N.L. Aging and late-life depression. J. Aging Health 2012, 24, 3–28. [Google Scholar] [CrossRef] [PubMed]
- Fortner, B.V.; Neimeyer, R.A. Death anxiety in older adults: A quantitative review. Death Stud. 1999, 23, 387–411. [Google Scholar] [CrossRef]
- Thorson, J.A.; Powell, F.C. Feelings about death in younger and older adults. In Series in Death, Dying, and Bereavement. Death Attitudes and the Older Adult: Theories, Concepts, and Applications; Tomer, A., Ed.; Brunner-Routledge: New York, NY, USA, 2000; pp. 123–136. [Google Scholar]
- Chan, L.C.; Yap, C.C. Age, gender, and religiosity as related to death anxiety. Sunway Acad. J. 2009, 6, 1–16. [Google Scholar]
- Krause, N. A preliminary assessment of race differences in the relationship between religious doubt and depressive symptoms. Rev. Relig. Res. 2003, 45, 93–115. [Google Scholar] [CrossRef]
- Galek, K.; Krause, N.; Ellison, C.G.; Kudler, T.; Flannelly, K.J. Religious doubt and mental health across the lifespan. J. Adult Dev. 2007, 14, 16–25. [Google Scholar] [CrossRef]
- Henrie, J.; Patrick, J.H. Religiousness, religious doubt, and death anxiety. Int. J. Aging Hum. Dev. 2014, 78, 203–227. [Google Scholar] [CrossRef]
- Ingram, B.J.; Leitner, L.M. Death threat, religiosity, and fear of death: A repertory grid investigation. Int. J. Pers. Constr. Psychol. 1989, 2, 199–214. [Google Scholar] [CrossRef]
- Wolitzky-Taylor, K.B.; Castriotta, N.; Lenze, E.J.; Stanley, M.A.; Craske, M.G. Anxiety disorders in older adults: A comprehensive review. Depress. Anxiety 2010, 27, 190–211. [Google Scholar] [CrossRef] [PubMed]
- Neimeyer, R.A. (Ed.) Death Anxiety Handbook: Research, Instrumentation, and Application; Taylor & Francis: New York, NY, USA, 2015. [Google Scholar]
- Russac, R.J.; Gatliff, C.; Reece, M.; Spottswood, D. Death anxiety across the adult years: An examination of age and gender effects. Death Stud. 2007, 34, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, N.; Moradi, M.; Soleimani, M.A.; Kalantari, Z.; Hosseini, F. Death anxiety and its relationship with quality of life in women with cancer. Iran J. Nurs. 2013, 26, 51–61. [Google Scholar]
- Sherman, D.W.; Norman, R.; McSherry, C.B. A comparison of death anxiety and quality of life of patients with advanced cancer or AIDS and their family caregivers. J. Assoc. Nurses AIDS Care 2010, 21, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Fortner, B.V.; Neimeyer, R.A.; Rybarczyk, B. Correlates of death anxiety in older adults: A comprehensive review. In Series in Death, Dying, and Bereavement. Death Attitudes and the Older Adult: Theories, Concepts, and Applications; Tomer, A., Ed.; Brunner-Routledge: New York, NY, USA, 2000; pp. 95–108. [Google Scholar]
- Cataldo, J.K. An Investigation of the Relationship of Hardiness and Death Attitudes to Depression in Older Persons in Skilled Nursing Facilities. Ph.D. Thesis, New York University, School of Education, Health, Nursing, and Arts Professions, New York, NY, USA, 1989. [Google Scholar]
- Templer, D.I. Death anxiety as related to depression and health of retired persons. J. Gerontol. 1971, 26, 521–523. [Google Scholar] [CrossRef]
- Williams, A.K. Physical Illness and Depression: Changes over Time in Middle Aged and Elderly Persons. Ph.D. Thesis, Portland State University, Portland, OR, USA, 1985. [Google Scholar]
- Argue, A.; Johnson, D.R.; White, L.K. Age and religiosity: Evidence from a three-wave panel analysis. J. Sci. Study Relig. 1999, 38, 423–435. [Google Scholar] [CrossRef]
- Hunsberger, B.; McKenzie, B.; Pratt, M.; Pancer, S.M. Religious doubt: A social psychological analysis. In Research in the Social Scientific Study of Religion; Lynn, M.L., Moberg, D.O., Eds.; JAI Press: Greenwich, CT, USA, 1993; Volume 5, pp. 27–51. [Google Scholar]
- Fowler, J.W. Stages of Faith: The Psychology of Human Development and the Quest for Meaning; Harper & Row: New York, NY, USA, 1976. [Google Scholar]
- Pargament, K.I.; Koenig, H.G.; Perez, L.M. The many methods of religious coping: Development and initial validation of the RCOPE. J. Clin. Psychol. 2000, 56, 519–543. [Google Scholar] [CrossRef]
- Krause, N.; Ingersoll-Dayton, B.; Ellison, C.G.; Wulff, K.M. Aging, religious doubt, and psychological well-being. Gerontologist 1999, 39, 525–533. [Google Scholar] [CrossRef]
- Pew Research Center. Religious Landscape Study. Religion & Public Life. Available online: http://www.pewforum.org/religious-landscape-study/ (accessed on 27 September 2019).
- Stark, R.; Finke, R. Acts of Faith: Explaining the Human Side of Religion; University of California Press: Berkeley, CA, USA, 2000. [Google Scholar]
- Putney, S.; Middleton, R. Dimensions and correlates of religious ideologies. Soc. Forces 1961, 39, 285–290. [Google Scholar] [CrossRef]
- Tomás-Sábado, J.; Gómez-Benito, J. Construction and validation of the Death Anxiety Inventory (DAI). Eur. J. Psychol. Assess. 2005, 21, 108–114. [Google Scholar] [CrossRef]
- Krause, N. Exploring race and sex differences in church involvement during late life. Int. J. Psychol. Relig. 2006, 16, 127–144. [Google Scholar] [CrossRef]
- Hope, M.O.; Assari, S.; Cole-Lewis, Y.C.; Caldwell, C.H. Religious social support, discrimination, and psychiatric disorders among Black adolescents. Race Soc. Probl. 2017, 9, 102–114. [Google Scholar] [CrossRef]
- Pargament, K.I. The psychology of Religion and Coping; Guilford: New York, NY, USA, 1997. [Google Scholar]
- Ferraro, K.F.; Kim, S. Health benefits of religion among Black and White older adults? Race, religiosity, and C-reactive protein. Soc. Sci. Med. 2014, 120, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Krause, N. Exploring the stress-buffering effects of church-based and secular social support on self-rated health in late life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2006, 61, S35–S43. [Google Scholar] [CrossRef] [PubMed]
- Krause, N. Religious meaning and subjective well-being in late life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.J.; Chatters, L.M.; Abelson, J.M. Religious involvement and DSM-IV 12 month and lifetime major depressive disorder among African Americans. J. Nerv. Ment. Dis. 2012, 200, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.W.; Aten, J.D.; Moore, M.; Hook, J.N.; Davis, D.E. Resource loss, religiousness, health, and posttraumatic growth following Hurricane Katrina. Ment. Health Relig. Cult. 2013, 16, 352–366. [Google Scholar] [CrossRef]
- Krause, N.; Wulff, K.M. Religious doubt and health: Exploring the potential dark side of religion. Sociol. Relig. 2004, 65, 35–56. [Google Scholar] [CrossRef]
- Krause, N. A comprehensive strategy for developing closed-ended survey items for use in studies of older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2002, 57, 263–274. [Google Scholar] [CrossRef]
- Neimeyer, R.A. (Ed.) Feelings about Death Handbook: Research, Instrumentation, and Application; Taylor & Francis: New York, NY, USA, 1994. [Google Scholar]
- Radloff, L.S. The CES-D scale a self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Karim, J.; Weisz, R.; Bibi, Z.; ur Rehman, S. Validation of the eight-item center for epidemiologic studies depression scale (CES-D) among older adults. Curr. Psychol. 2015, 34, 681–692. [Google Scholar] [CrossRef]
- Little, R.J. A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. SEM: An introduction. In Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd ed.; Lawrence Erlbaum: Mahwah, NJ, USA, 2003. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Koenig, H.G. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012, 2012, 278730. [Google Scholar] [CrossRef] [PubMed]
- Ronneberg, C.R.; Miller, E.A.; Dugan, E.; Porell, F. The protective effects of religiosity on depression: A 2-year prospective study. Gerontologist 2014, 56, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Krause, N.; Ellison, C.G. The doubting process: A longitudinal study of the precipitants and consequences of religious doubt in older adults. J. Sci. Study Relig. 2009, 48, 293–342. [Google Scholar] [CrossRef]
- Cicirelli, V.G. Fear of death in older adults: Predictions from terror management theory. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2002, 57, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.H. Religiosity and death anxiety. J. Hum. Resour. Adult Learn. 2010, 6, 34–37. [Google Scholar]
- Pargament, K.I.; Smith, B.W.; Koenig, H.G.; Perez, L. Patterns of positive and negative religious coping with major life stressors. J. Sci. Study Relig. 1998, 37, 710–724. [Google Scholar] [CrossRef]
- Wood, J.B.; Parham, I.A. Coping with perceived burden: Ethnic and cultural issues in Alzheimer’s family caregiving. J. Appl. Gerontol. 1990, 9, 325–339. [Google Scholar] [CrossRef]
- Kelley, D. Why Conservative Churches Are Growing; Harper & Row: New York, NY, USA, 1972. [Google Scholar]
- Pargament, K.; Feuille, M.; Burdzy, D. The Brief RCOPE: Current psychometric status of a short measure of religious coping. Religions 2011, 2, 51–76. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Overall Sample | Black | White | p-Value | |||
|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | ||
| Sex | 0.49 | ||||||
| Female | 626 | (63.0) | 318 | (66.0) | 308 | (60.3) | |
| Male | 367 | (37.0) | 164 | (34.0) | 203 | (39.7) | |
| Marital Status | 0.004 | ||||||
| Married | 465 | (46.8) | 172 | (35.7) | 293 | (57.3) | |
| Separated/Divorced | 93 | (9.4) | 65 | (12.5) | 28 | (5.5) | |
| Widowed | 400 | (40.3) | 228 | (47.3) | 172 | (33.7) | |
| Never Married | 33 | (3.3) | 15 | (3.1) | 18 | (3.5) | |
| Religious Affiliation | |||||||
| Catholic | 175 | (17.6) | 33 | (6.8) | 142 | (27.8) | <0.001 |
| Protestant | 631 | (63.5) | 354 | (73.4) | 277 | (54.2) | |
| Other | 150 | (15.1) | 83 | (17.2) | 67 | (13.1) | |
| Annual Family Income | |||||||
| Less than 10k | 130 | (13.1) | 108 | (22.4) | 22 | (4.3) | <0.001 |
| 10–20k | 232 | (23.4) | 135 | (28.0) | 97 | (19.0) | |
| 20–30k | 153 | (15.4) | 58 | (12.0) | 95 | (18.6) | |
| 30–40k | 63 | (6.3) | 21 | (4.4) | 42 | (8.2) | |
| 40–60k | 60 | (6.0) | 11 | (2.3) | 49 | (9.6) | |
| Over 60k | 61 | (6.1) | 5 | (1.0) | 56 | (10.9) | |
| Religious Attendance | <0.001 | ||||||
| Never | 205 | (20.6) | 53 | (11.0) | 152 | (29.7) | |
| Few times a year | 182 | (18.3) | 93 | (19.2) | 89 | (17.4) | |
| Few times a month | 100 | (10.1) | 71 | (14.7) | 29 | (5.7) | |
| Weekly | 423 | (42.6) | 215 | (44.6) | 208 | (40.7) | |
| Several times a week | 76 | (7.7) | 46 | (9.5) | 30 | (5.9) | |
| Age (Mean, SD) | 77.47 | (6.16) | 77.35 | (6.23) | 77.59 | (6.09) | 0.53 |
| Death Anxiety (Mean, SD) | 7.92 | (2.68) | 7.91 | (2.77) | 7.94 | (2.60) | 0.65 |
| Religious Doubt (Mean, SD) | 6.89 | (2.99) | 6.30 | (2.50) | 7.48 | (3.30) | 0.003 |
| Depressive Symptoms (Mean, SD) | 11.69 | (4.78) | 11.71 | (4.70) | 11.67 | (4.85) | 0.77 |
| Rumination (Mean, SD) | 9.45 | (2.95) | 9.60 | (3.03) | 9.32 | (2.88) | 0.49 |
| Subjective Health (Mean, SD) | 2.40 | (0.92) | 2.52 | (0.86) | 2.29 | (0.95) | 0.08 |
| Variable | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Death Anxiety | 1.00 | 0.17 ** | 0.13 ** | 0.19 ** | 0.04 |
| I find it hard to face up to the fact that I will die. | |||||
| Thinking about death makes me feel uneasy. | |||||
| I do not feel prepared to face my own death. | |||||
| I am disturbed by the shortness of life. | |||||
| 2. Religious Doubt | 1.00 | 0.06 | 0.12 ** | −0.02 | |
| How often do you have doubts about your religious or spiritual beliefs? | |||||
| How often do you have doubts about the things you’ve been taught in church? | |||||
| How often do you doubt whether solutions to your problems can be found in the Bible? | |||||
| How often do you doubt whether your prayers make a difference in your life? | |||||
| How often do you doubt that God is directly involved in your daily life? | |||||
| 3. Depressive Symptoms | 1.00 | 0.41 ** | 0.40 ** | ||
| I felt I could not shake off the blues, even with the help of my family and friends. | |||||
| I felt depressed. | |||||
| I had crying spells. | |||||
| I felt sad. | |||||
| I did not feel like eating, my appetite was poor. | |||||
| I felt like everything I did was an effort. | |||||
| My sleep was restless. | |||||
| I could not get going. | |||||
| 4. Rumination | 1.00 | 0.19 ** | |||
| I often have thoughts I try to avoid. | |||||
| There are thoughts that keep jumping into my head. | |||||
| I wish I could stop thinking about certain things. | |||||
| I have thoughts I cannot stop. | |||||
| 5. Subjective Health | |||||
| How would you rate your overall health at the present time? | 1.00 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willis, K.D.; Nelson, T.; Moreno, O. Death Anxiety, Religious Doubt, and Depressive Symptoms across Race in Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 3645. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193645
Willis KD, Nelson T, Moreno O. Death Anxiety, Religious Doubt, and Depressive Symptoms across Race in Older Adults. International Journal of Environmental Research and Public Health. 2019; 16(19):3645. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193645
Chicago/Turabian StyleWillis, Kelcie D., Tamara Nelson, and Oswaldo Moreno. 2019. "Death Anxiety, Religious Doubt, and Depressive Symptoms across Race in Older Adults" International Journal of Environmental Research and Public Health 16, no. 19: 3645. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193645