The Effects of 12 Weeks of a Combined Exercise Program on Physical Function and Hormonal Status in Elderly Korean Women



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval and Consent to Participate
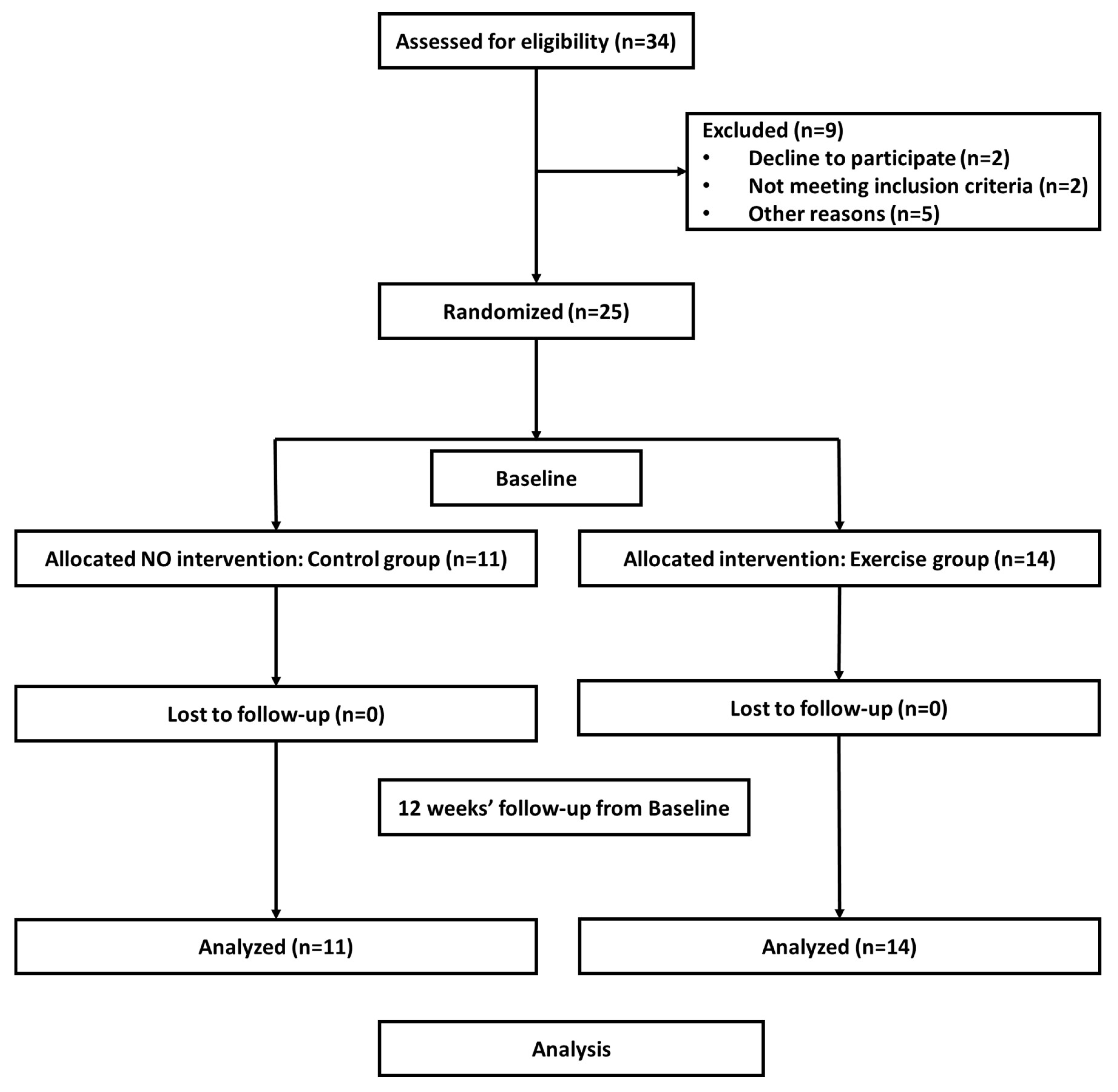
2.2. Participants and Study Design
2.3. Perceived Exertion
2.4. Exercise Program
2.5. Assessment of Body Composition, Balance, Flexibility, and Muscle Strength
2.6. Blood Collection and Measurements
2.7. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Statistical Research Institute. Social Trend of Korea 2018; Korea National Statistical Office, Statistical Research Institute: Daejeon, Korea, 2018.
- Statistical Research Institute. Social Trend of Korea 2013; Korea National Statistical Office, Statistical Research Institute: Daejeon, Korea, 2013.
- Bartke, A. Growth Hormone and Aging: Updated Review. World J. Mens Health 2019, 37, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.; Santoro, A.; Franceschi, C.; Kadi, F. Detrimental links between physical inactivity, metabolic risk and N-glycomic biomarkers of aging. Exp. Gerontol. 2019, 124, 110626. [Google Scholar] [CrossRef] [PubMed]
- Martini, E.M.; Garrett, N.; Lindquist, T.; Isham, G.J. The boomers are coming: A total cost of care model of the impact of population aging on health care costs in the United States by Major Practice Category. Health Serv. Res. 2007, 42, 201–218. [Google Scholar] [CrossRef] [PubMed]
- Velez, M.P.; Rosendaal, N.; Alvarado, B.; da Camara, S.; Belanger, E.; Pirkle, C.M. Data on the association between age at natural menopause and physical function in older women from the International Mobility in Aging Study (IMIAS). Data Brief. 2019, 23, 103811. [Google Scholar] [CrossRef]
- Mayhew, A.J.; Griffith, L.E.; Gilsing, A.; Beauchamp, M.K.; Kuspinar, A.; Raina, P. The association between self-reported and performance-based physical function with activities of daily living disability in the Canadian Longitudinal Study on Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2019. Epub ahead of print. [Google Scholar] [CrossRef]
- Dipietro, L.; Campbell, W.W.; Buchner, D.M.; Erickson, K.I.; Powell, K.E.; Bloodgood, B.; Hughes, T.; Day, K.R.; Piercy, K.L.; Vaux-Bjerke, A.; et al. Physical Activity, Injurious Falls, and Physical Function in Aging: An Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1303–1313. [Google Scholar] [CrossRef]
- Konak, H.E.; Kibar, S.; Ergin, E.S. The effect of single-task and dual-task balance exercise programs on balance performance in adults with osteoporosis: A randomized controlled preliminary trial. Osteoporos Int. 2016, 27, 3271–3278. [Google Scholar] [CrossRef]
- Stathokostas, L.; Little, R.M.; Vandervoort, A.A.; Paterson, D.H. Flexibility training and functional ability in older adults: A systematic review. J. Aging Res. 2012, 2012, 306818. [Google Scholar] [CrossRef]
- Stathokostas, L.; McDonald, M.W.; Little, R.M.; Paterson, D.H. Flexibility of older adults aged 55-86 years and the influence of physical activity. J. Aging Res. 2013, 2013, 743843. [Google Scholar] [CrossRef]
- Trivedi, D.P.; Khaw, K.T. Dehydroepiandrosterone sulfate and mortality in elderly men and women. J. Clin. Endocrinol. Metab. 2001, 86, 4171–4177. [Google Scholar] [CrossRef]
- Vincent, A.; Riggs, B.L.; Atkinson, E.J.; Oberg, A.L.; Khosla, S. Effect of estrogen replacement therapy on parathyroid hormone secretion in elderly postmenopausal women. Menopause 2003, 10, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Meinhardt, U.J.; Ho, K.K. Modulation of growth hormone action by sex steroids. Clin. Endocrinol. (Oxf) 2006, 65, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, F.C.; Landon, J. Growth hormone secretion in response to stress in man. Nature 1966, 210, 540–541. [Google Scholar] [CrossRef]
- Roy, T.A.; Blackman, M.R.; Harman, S.M.; Tobin, J.D.; Schrager, M.; Metter, E.J. Interrelationships of serum testosterone and free testosterone index with FFM and strength in aging men. Am. J. Physiol. Endocrinol. Metab. 2002, 283, E284–E294. [Google Scholar] [CrossRef]
- Darabi, M.; Ani, M.; Panjehpour, M.; Rabbani, M.; Movahedian, A.; Zarean, E. Effect of estrogen receptor beta A1730G polymorphism on ABCA1 gene expression response to postmenopausal hormone replacement therapy. Genet. Test. Mol. Biomarkers 2011, 15, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Nawata, H.; Yanase, T.; Goto, K.; Okabe, T.; Ashida, K. Mechanism of action of anti-aging DHEA-S and the replacement of DHEA-S. Mech. Ageing Dev. 2002, 123, 1101–1106. [Google Scholar] [CrossRef]
- Vandevyver, C.; Vanhoof, J.; Declerck, K.; Stinissen, P.; Vandervorst, C.; Michiels, L.; Cassiman, J.J.; Boonen, S.; Raus, J.; Geusens, P. Lack of association between estrogen receptor genotypes and bone mineral density, fracture history, or muscle strength in elderly women. J. Bone Miner. Res. 1999, 14, 1576–1582. [Google Scholar] [CrossRef]
- Orentreich, N.; Brind, J.L.; Rizer, R.L.; Vogelman, J.H. Age changes and sex differences in serum dehydroepiandrosterone sulfate concentrations throughout adulthood. J. Clin. Endocrinol. Metab. 1984, 59, 551–555. [Google Scholar] [CrossRef]
- Valenti, G.; Denti, L.; Maggio, M.; Ceda, G.; Volpato, S.; Bandinelli, S.; Ceresini, G.; Cappola, A.; Guralnik, J.M.; Ferrucci, L. Effect of DHEAS on skeletal muscle over the life span: The InCHIANTI study. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 466–472. [Google Scholar] [CrossRef]
- Kahonen, M.H.; Tilvis, R.S.; Jolkkonen, J.; Pitkala, K.; Harkonen, M. Predictors and clinical significance of declining plasma dehydroepiandrosterone sulfate in old age. Aging (Milano) 2000, 12, 308–314. [Google Scholar]
- Mazat, L.; Lafont, S.; Berr, C.; Debuire, B.; Tessier, J.F.; Dartigues, J.F.; Baulieu, E.E. Prospective measurements of dehydroepiandrosterone sulfate in a cohort of elderly subjects: Relationship to gender, subjective health, smoking habits, and 10-year mortality. Proc. Natl. Acad. Sci. USA 2001, 98, 8145–8150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monico-Neto, M.; Antunes, H.K.; Dattilo, M.; Medeiros, A.; Souza, H.S.; Lee, K.S.; de Melo, C.M.; Tufik, S.; de Mello, M.T. Resistance exercise: A non-pharmacological strategy to minimize or reverse sleep deprivation-induced muscle atrophy. Med. Hypotheses 2013, 80, 701–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, C.B.; Teixeira, P.D.S.; Alves Dos Santos, G.; Dantas Maya, A.T.; Americano do Brasil, P.; Souza, V.C.; Cordova, C.; Ferreira, A.P.; Lima, R.M.; Nobrega, O.T. Effects of a 12-Week Exercise Training Program on Physical Function in Institutionalized Frail Elderly. J. Aging Res. 2018, 2018, 7218102. [Google Scholar] [CrossRef] [PubMed]
- Geirsdottir, O.G.; Arnarson, A.; Ramel, A.; Briem, K.; Jonsson, P.V.; Thorsdottir, I. Muscular strength and physical function in elderly adults 6-18 months after a 12-week resistance exercise program. Scand. J. Public Health 2015, 43, 76–82. [Google Scholar] [CrossRef]
- Borst, S.E.; Millard, W.J.; Lowenthal, D.T. Growth hormone, exercise, and aging: The future of therapy for the frail elderly. J. Am. Geriatr. Soc. 1994, 42, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; Earnest, C.P.; Blair, S.N.; Church, T.S. The effect of different doses of aerobic exercise training on endothelial function in postmenopausal women with elevated blood pressure: Results from the DREW study. Br. J. Sports Med. 2012, 46, 753–758. [Google Scholar] [CrossRef]
- Lim, S.T.; Min, S.K.; Park, H.; Park, J.H.; Park, J.K. Effects of a healthy life exercise program on arteriosclerosis adhesion molecules in elderly obese women. J. Phys. Ther. Sci. 2015, 27, 1529–1532. [Google Scholar] [CrossRef] [Green Version]
- Jang, H.R.; Lee, J.H.; Lee, S.K. The comparison of body composition, functional performance ability, talar tilt angle and foot injuries in accordance with the functional ankle instability in high school traditional Korean dance majors. Korea Dance Educ. Soc. J. 2014, 25, 149–162. [Google Scholar]
- Park, J.H.; Park, H.; Lim, S.T.; Park, J.K. Effects of a 12-week healthy-life exercise program on oxidized low-density lipoprotein cholesterol and carotid intima-media thickness in obese elderly women. J. Phys. Ther. Sci. 2015, 27, 1435–1439. [Google Scholar] [CrossRef] [Green Version]
- Jeon, M.Y.; Bark, E.S.; Lee, E.G.; Im, J.S.; Jeong, B.S.; Choe, E.S. The effects of a Korean traditional dance movement program in elderly women. Taehan Kanho Hakhoe Chi 2005, 35, 1268–1276. [Google Scholar] [CrossRef]
- Kim, S.M.; Park, H.J.; Min, B.J.; So, W.Y. Effects of a Korean Traditional Dance Program on Health-related Fitness and Blood Lipid Profiles in Korean Elderly Females. Iran. J. Public Health 2018, 47, 127–129. [Google Scholar] [PubMed]
- Chatterjee, S.; Mondal, S. Effect of regular yogic training on growth hormone and dehydroepiandrosterone sulfate as an endocrine marker of aging. Evid. Based Complement. Altern. Med. 2014, 2014, 240581. [Google Scholar] [CrossRef] [PubMed]
- Chaya, M.S.; Kurpad, A.V.; Nagendra, H.R.; Nagarathna, R. The effect of long term combined yoga practice on the basal metabolic rate of healthy adults. BMC Complement. Altern. Med. 2006, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Raub, J.A. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: A literature review. J. Altern. Complement. Med. 2002, 8, 797–812. [Google Scholar] [CrossRef]
- Seco, J.; Abecia, L.C.; Echevarria, E.; Barbero, I.; Torres-Unda, J.; Rodriguez, V.; Calvo, J.I. A long-term physical activity training program increases strength and flexibility, and improves balance in older adults. Rehabil. Nurs. 2013, 38, 37–47. [Google Scholar] [CrossRef]
- Scherr, J.; Wolfarth, B.; Christle, J.W.; Pressler, A.; Wagenpfeil, S.; Halle, M. Associations between Borg’s rating of perceived exertion and physiological measures of exercise intensity. Eur. J. Appl. Physiol. 2013, 113, 147–155. [Google Scholar] [CrossRef]
- Park, J.M.; Hyun, G.S.; Jee, Y.S. Effects of pilates core stability exercises on the balance abilities of archers. J. Exerc. Rehabil. 2016, 12, 553–558. [Google Scholar] [CrossRef]
- Adamo, D.E.; Talley, S.A.; Goldberg, A. Age and task differences in functional fitness in older women: Comparisons with Senior Fitness Test normative and criterion-referenced data. J. Aging Phys. Act. 2015, 23, 47–54. [Google Scholar] [CrossRef]
- Dugan, S.A.; Gabriel, K.P.; Lange-Maia, B.S.; Karvonen-Gutierrez, C. Physical Activity and Physical Function: Moving and Aging. Obstet. Gynecol. Clin. N. Am. 2018, 45, 723–736. [Google Scholar] [CrossRef]
- Patel, K.V.; Phelan, E.A.; Leveille, S.G.; Lamb, S.E.; Missikpode, C.; Wallace, R.B.; Guralnik, J.M.; Turk, D.C. High prevalence of falls, fear of falling, and impaired balance in older adults with pain in the United States: Findings from the 2011 National Health and Aging Trends Study. J. Am. Geriatr. Soc. 2014, 62, 1844–1852. [Google Scholar] [CrossRef]
- Calcada, D.; Vianello, D.; Giampieri, E.; Sala, C.; Castellani, G.; de Graaf, A.; Kremer, B.; van Ommen, B.; Feskens, E.; Santoro, A.; et al. The role of low-grade inflammation and metabolic flexibility in aging and nutritional modulation thereof: A systems biology approach. Mech. Ageing Dev. 2014, 136–137, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Somani, Y.B.; Pawelczyk, J.A.; De Souza, M.J.; Kris-Etherton, P.M.; Proctor, D.N. Aging women and their endothelium: Probing the relative role of estrogen on vasodilator function. Am. J. Physiol. Heart. Circ. Physiol. 2019, 317, H395–H404. [Google Scholar] [CrossRef] [PubMed]
- Nigdelis, M.P.; Martinez-Dominguez, S.J.; Goulis, D.G.; Perez-Lopez, F.R. Effect of programmed exercise on perceived stress in middle-aged and old women: A meta-analysis of randomized trials. Maturitas 2018, 114, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Furtado, H.L.; Sousa, N.; Simao, R.; Pereira, F.D.; Vilaca-Alves, J. Physical exercise and functional fitness in independently living vs. institutionalized elderly women: A comparison of 60- to 79-year-old city dwellers. Clin. Interv. Aging 2015, 10, 795–801. [Google Scholar] [PubMed]
- Santaella, D.F.; Devesa, C.R.; Rojo, M.R.; Amato, M.B.; Drager, L.F.; Casali, K.R.; Montano, N.; Lorenzi-Filho, G. Yoga respiratory training improves respiratory function and cardiac sympathovagal balance in elderly subjects: A randomised controlled trial. BMJ Open 2011, 1, e000085. [Google Scholar] [CrossRef]
- Youkhana, S.; Dean, C.M.; Wolff, M.; Sherrington, C.; Tiedemann, A. Yoga-based exercise improves balance and mobility in people aged 60 and over: A systematic review and meta-analysis. Age Ageing 2016, 45, 21–29. [Google Scholar] [CrossRef]
- Melzer, I.; Benjuya, N.; Kaplanski, J. Postural stability in the elderly: A comparison between fallers and non-fallers. Age Ageing 2004, 33, 602–607. [Google Scholar] [CrossRef]
- Muir, S.W.; Berg, K.; Chesworth, B.M.; Klar, N.; Speechley, M. Modifiable Risk Factors Identify People Who Transition from Non-fallers to Fallers in Community-Dwelling Older Adults: A Prospective Study. Physiother. Can. 2010, 62, 358–367. [Google Scholar] [CrossRef]
- Thomas, E.; Battaglia, G.; Patti, A.; Brusa, J.; Leonardi, V.; Palma, A.; Bellafiore, M. Physical activity programs for balance and fall prevention in elderly: A systematic review. Medicine (Baltimore) 2019, 98, e16218. [Google Scholar] [CrossRef]
- Smeets, E.; Schutzler, S.E.; Wei, J.Y.; Azhar, G.; Wolfe, R.R. Do anabolic nutritional supplements stimulate human growth hormone secretion in elderly women with heart failure? Physiol. Rep. 2017, 5, e13366. [Google Scholar] [CrossRef]
- Morrison, M.F.; Freeman, E.W.; Lin, H.; Sammel, M.D. Higher DHEA-S (dehydroepiandrosterone sulfate) levels are associated with depressive symptoms during the menopausal transition: Results from the PENN Ovarian Aging Study. Arch. Womens Ment. Health 2011, 14, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Sampson, J.N.; Brenner, D.R.; Moore, S.C.; Courneya, K.S.; Ziegler, R.G.; Friedenreich, C.M. Effects of Exercise and Cardiorespiratory Fitness on Estrogen Metabolism in Postmenopausal Women. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1480–1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li Voon Chong, J.S.; Benbow, S.; Foy, P.; Wallymahmed, M.E.; Wile, D.; MacFarlane, I.A. Elderly people with hypothalamic-pituitary disease and growth hormone deficiency: Lipid profiles, body composition and quality of life compared with control subjects. Clin. Endocrinol. (Oxf) 2000, 53, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Rudman, D.; Feller, A.G.; Nagraj, H.S.; Gergans, G.A.; Lalitha, P.Y.; Goldberg, A.F.; Schlenker, R.A.; Cohn, L.; Rudman, I.W.; Mattson, D.E. Effects of human growth hormone in men over 60 years old. N. Engl. J. Med. 1990, 323, 1–6. [Google Scholar] [CrossRef]
- Holloway, L.; Butterfield, G.; Hintz, R.L.; Gesundheit, N.; Marcus, R. Effects of recombinant human growth hormone on metabolic indices, body composition, and bone turnover in healthy elderly women. J. Clin. Endocrinol. Metab. 1994, 79, 470–479. [Google Scholar]
- Blackman, M.R.; Sorkin, J.D.; Munzer, T.; Bellantoni, M.F.; Busby-Whitehead, J.; Stevens, T.E.; Jayme, J.; O’Connor, K.G.; Christmas, C.; Tobin, J.D.; et al. Growth hormone and sex steroid administration in healthy aged women and men: A randomized controlled trial. JAMA 2002, 288, 2282–2292. [Google Scholar] [CrossRef]
- Liu, H.; Bravata, D.M.; Olkin, I.; Nayak, S.; Roberts, B.; Garber, A.M.; Hoffman, A.R. Systematic review: The safety and efficacy of growth hormone in the healthy elderly. Ann. Intern. Med. 2007, 146, 104–115. [Google Scholar] [CrossRef]
- Fukai, S.; Akishita, M.; Yamada, S.; Hama, T.; Ogawa, S.; Iijima, K.; Eto, M.; Kozaki, K.; Toba, K.; Ouchi, Y. Association of plasma sex hormone levels with functional decline in elderly men and women. Geriatr. Gerontol. Int. 2009, 9, 282–289. [Google Scholar] [CrossRef]
- Goldman, N.; Glei, D.A. Sex differences in the relationship between DHEAS and health. Exp. Gerontol. 2007, 42, 979–987. [Google Scholar] [CrossRef] [Green Version]
- Morsink, L.F.; Vogelzangs, N.; Nicklas, B.J.; Beekman, A.T.; Satterfield, S.; Rubin, S.M.; Yaffe, K.; Simonsick, E.; Newman, A.B.; Kritchevsky, S.B.; et al. Associations between sex steroid hormone levels and depressive symptoms in elderly men and women: Results from the Health ABC study. Psychoneuroendocrinology 2007, 32, 874–883. [Google Scholar] [CrossRef]
- Munsell, M.F.; Sprague, B.L.; Berry, D.A.; Chisholm, G.; Trentham-Dietz, A. Body mass index and breast cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status. Epidemiol. Rev. 2014, 36, 114–136. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.M.; Kang, Y.; Zhuang, Y.C. Effects of Elastic Resistance Band Exercise on Postural Balance, Estrogen, Bone Metabolism Index, and Muscle Strength of Perimenopausal Period Women. J. Am. Geriatr. Soc. 2016, 64, 1368–1370. [Google Scholar] [CrossRef] [PubMed]
- Moreau, K.L.; Stauffer, B.L.; Kohrt, W.M.; Seals, D.R. Essential role of estrogen for improvements in vascular endothelial function with endurance exercise in postmenopausal women. J. Clin. Endocrinol. Metab. 2013, 98, 4507–4515. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Exercise | Duration | Frequency | Week | Intensity | ||
|---|---|---|---|---|---|---|
| Warm up | Stretching | 5 min | 3 times/week | 1–6 | RPE 12 | |
| Main exercise | Static balance exercise | Valdidim, Parlsawee, Zainngareem, Saetaryeong | 30 min | |||
| Dynamic balance exercise | A sitting position, Sitting Forward Bend Pose, Butterfly Pose, Bat Pose, God of the Half Fishes Pose, Cow Facing Pose | 20 min | 6–12 | RPE 13 | ||
| Cool-down | Stretching, respiration arrangement, and meditation (Baddha Konasana) | 5 min | ||||
| Variable 1 | Intervention | Effects (p-Value) | |||||
|---|---|---|---|---|---|---|---|
| Control Group (n = 11) | Exercise Group (n = 14) | ||||||
| Baseline | 12 Weeks | Baseline | 12 Weeks | Time | Group | Time × Group | |
| Age (years) | 69.36 ± 2.94 | - | 71.57 ± 3.22 | - | N.A. | N.A. | N.A. |
| Height (cm) | 154.63 ± 5.04 | - | 153.57 ± 7.11 | - | N.A. | N.A. | N.A. |
| Weight (kg) | 62.83 ± 7.58 | 63.00 ± 8.00 | 58.76 ± 9.01 | 59.32 ± 8.94 | 0.877 | 0.116 | 0.936 |
| LBM (kg) | 39.40 ± 4.39 | 38.87 ± 4.53 | 37.02 ± 4.50 | 37.17 ± 4.39 | 0.877 | 0.115 | 0.790 |
| FM (kg) | 23.41 ± 3.98 | 24.13 ± 4.47 | 21.72 ± 5.52 | 22.15 ± 5.30 | 0.685 | 0.199 | 0.918 |
| BF (%) | 37.19 ± 2.93 | 38.16 ± 3.46 | 36.58 ± 4.73 | 36.99 ± 4.08 | 0.542 | 0.433 | 0.802 |
| BMI (kg.m−2) | 26.36 ± 2.38 | 26.31 ± 2.73 | 24.77 ± 2.84 | 25.07 ± 2.37 | 0.868 | 0.062 | 0.820 |
| Variable | Intervention | Effects (p-Value) | |||||
|---|---|---|---|---|---|---|---|
| Control Group (n = 11) | Exercise Group (n = 14) | ||||||
| Baseline | 12 Weeks | Baseline | 12 Weeks | Time | Group | Time × Group | |
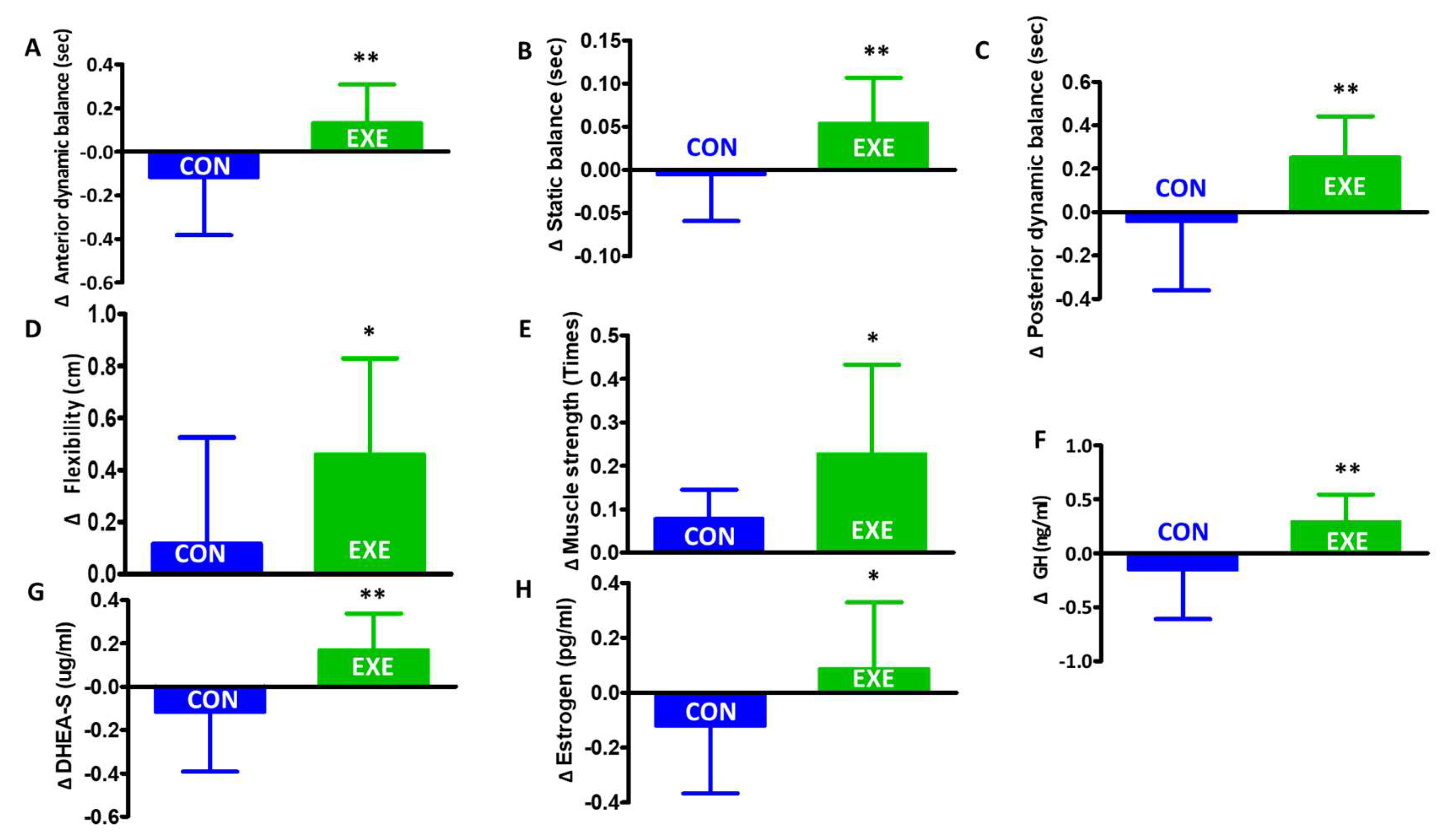
| Anterior dynamic balance (sec) | 32.18 ± 3.81 | 30.09 ± 6.90 | 32.35 ± 5.34 | 37.78 ± 4.59 | 0.270 | 0.012 | 0.016 |
| Posterior dynamic balance (sec) | 22.27 ± 4.62 | 22.81 ± 7.01 | 21.64 ± 5.10 | 29.71 ± 6.75 | 0.15 | 0.072 | 0.032 |
| Static balance (sec) | 87.18 ± 3.60 | 86.90 ± 2.77 | 86.71 ± 3.60 | 91.71 ± 1.85 | 0.008 | 0.014 | 0.003 |
| Flexibility (cm) | 11.36 ± 9.40 | 13.60 ± 9.00 | 10.57 ± 8.59 | 18.11 ± 7.49 | 0.51 | 0.452 | 0.284 |
| Muscle strength | 12.72 ± 3.63 | 13.72 ± 3.28 | 14.35 ± 3.05 | 19.35 ± 4.60 | 0.007 | 0.001 | 0.066 |
| GH (ng/mL) | 1.35 ± 0.41 | 1.24 ± 0.33 | 1.14 ± 0.46 | 1.88 ± 1.11 | 0.109 | 0.278 | 0.037 |
| DHEA-S (µg/mL) | 46.89 ± 20.01 | 43.30 ± 19.38 | 62.15 ± 33.83 | 75.90 ± 40.84 | 0.568 | 0.010 | 0.332 |
| Estrogen (pg/mL) | 26.36 ± 2.38 | 26.31 ± 2.73 | 24.77 ± 2.84 | 25.07 ± 2.37 | 0.868 | 0.062 | 0.820 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Im, J.Y.; Bang, H.S.; Seo, D.Y. The Effects of 12 Weeks of a Combined Exercise Program on Physical Function and Hormonal Status in Elderly Korean Women. Int. J. Environ. Res. Public Health 2019, 16, 4196. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214196
Im JY, Bang HS, Seo DY. The Effects of 12 Weeks of a Combined Exercise Program on Physical Function and Hormonal Status in Elderly Korean Women. International Journal of Environmental Research and Public Health. 2019; 16(21):4196. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214196
Chicago/Turabian StyleIm, Ji Yu, Hyun Seok Bang, and Dae Yun Seo. 2019. "The Effects of 12 Weeks of a Combined Exercise Program on Physical Function and Hormonal Status in Elderly Korean Women" International Journal of Environmental Research and Public Health 16, no. 21: 4196. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214196