Associations between Maternal Health-Related Quality of Life during Pregnancy and Birth Outcomes: The Generation R Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
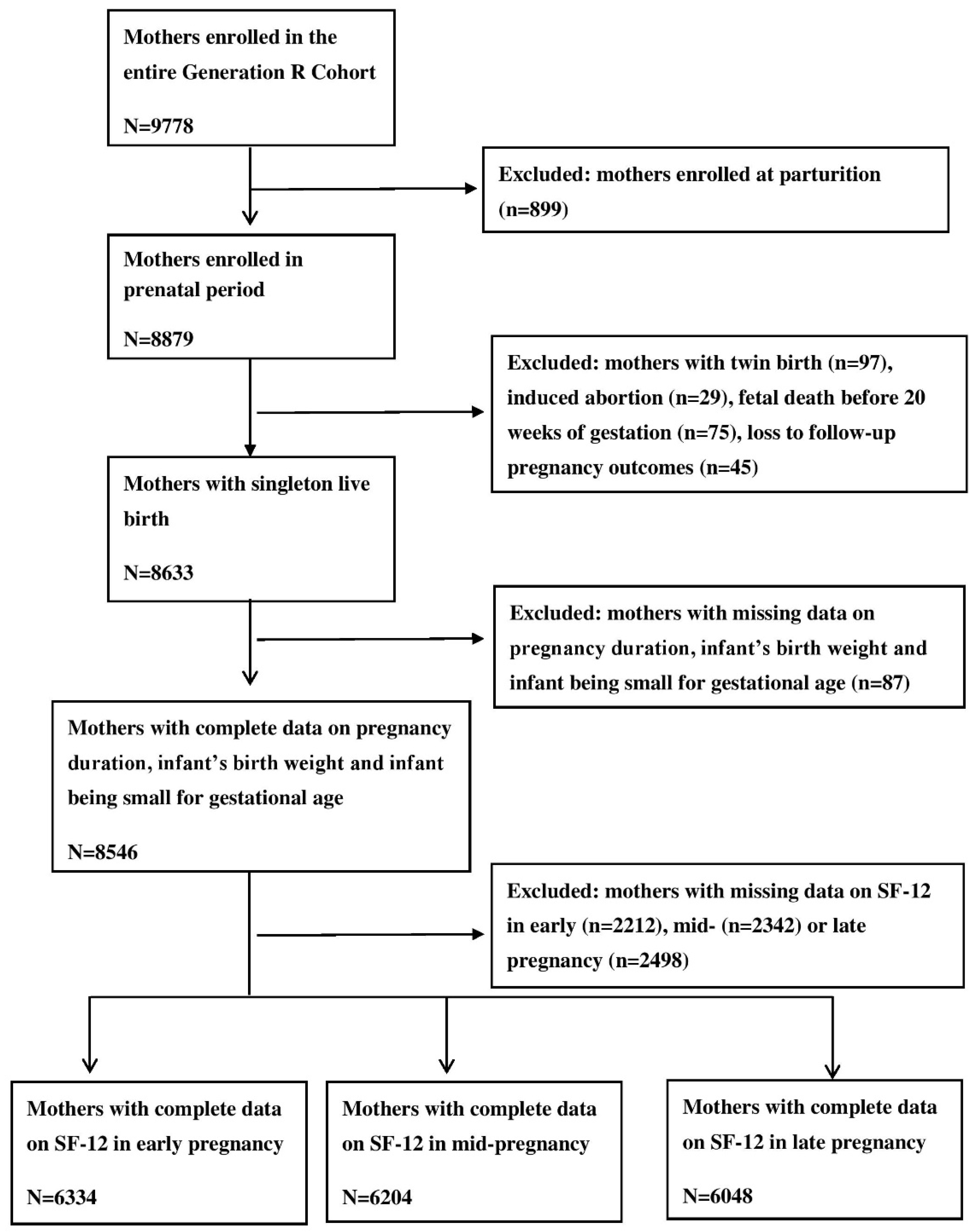
2.2. Study Population
2.3. HRQoL
2.4. Birth Outcomes
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. General Characterisitics of Mothers and Children
3.2. Associations between Physical and Mental HRQoL during Pregnancy and Birth Outcomes
3.3. Differences in Birth Outcomes between Subgroups with Very High vs. Very Low HRQoL during Pregnancy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Beck, S.; Wojdyla, D.; Say, L.; Betran, A.P.; Merialdi, M.; Requejo, J.H.; Rubens, C.; Menon, R.; Van Look, P.F. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull. World Health Organ. 2010, 88, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.; Salihu, H.M.; Keith, L.G.; Kirby, R.S.; Fowler, K.B.; Pass, M.A. SGA subtypes and mortality risk among singleton births. Early Hum. Dev. 2007, 83, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Cousens, S.; Chou, D.; Oestergaard, M.; Say, L.; Moller, A.-B.; Kinney, M.; Lawn, J. Born Too Soon: The global epidemiology of 15 million preterm births. Reprod. Health 2013, 10, S2. [Google Scholar] [CrossRef] [PubMed]
- Oudgenoeg-Paz, O.; Mulder, H.; Jongmans, M.J.; van der Ham, I.J.M.; Van der Stigchel, S. The link between motor and cognitive development in children born preterm and/or with low birth weight: A review of current evidence. Neurosci. Biobehav. Rev. 2017, 80, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Heaman, M.; Kingston, D.; Chalmers, B.; Sauve, R.; Lee, L.; Young, D. Risk Factors for Preterm Birth and Small-for-gestational-age Births among Canadian Women. Paediatr. Perinat. Epidemiol. 2013, 27, 54–61. [Google Scholar] [CrossRef]
- Frey, H.A.; Klebanoff, M.A. The epidemiology, etiology, and costs of preterm birth. Semin. Fetal Neonatal Med. 2016, 21, 68–73. [Google Scholar] [CrossRef]
- Kaplan, R.M. Quality of Life Measures: Measurement Strategies in Health Psychology; John Wiley: New York, NY, USA, 1985. [Google Scholar]
- Tibblin, G.; Svardsudd, K.; Welin, L.; Erikson, H.; Larsson, B. Quality of life as an outcome variable and a risk factor for total mortality and cardiovascular disease: A study of men born in 1913. J. Hypertens Suppl. 1993, 11, S81–S86. [Google Scholar] [CrossRef]
- Mapes, D.L.; Lopes, A.A.; Satayathum, S.; McCullough, K.P.; Goodkin, D.A.; Locatelli, F.; Fukuhara, S.; Young, E.W.; Kurokawa, K.; Saito, A.; et al. Health-related quality of life as a predictor of mortality and hospitalization: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int. 2003, 64, 339–349. [Google Scholar] [CrossRef] [Green Version]
- Stamnes Koepp, U.M.; Frost Andersen, L.; Dahl-Joergensen, K.; Stigum, H.; Nass, O.; Nystad, W. Maternal pre-pregnant body mass index, maternal weight change and offspring birthweight. Acta. Obstet. Gynecol. Scand. 2012, 91, 243–249. [Google Scholar] [CrossRef]
- Rodriguez, A.; Bohlin, G.; Lindmark, G. Symptoms across pregnancy in relation to psychosocial and biomedical factors. Acta. Obstet. Gynecol. Scand. 2001, 80, 213–223. [Google Scholar] [CrossRef]
- Mautner, E.; Greimel, E.; Trutnovsky, G.; Daghofer, F.; Egger, J.W.; Lang, U. Quality of life outcomes in pregnancy and postpartum complicated by hypertensive disorders, gestational diabetes, and preterm birth. J. Psychosom. Obstet. Gynaecol. 2009, 30, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Liou, S.-R.; Cheng, C.-Y. Prediction of maternal quality of life on preterm birth and low birthweight: A longitudinal study. BMC Pregnancy Childbirth 2013, 13, 124. [Google Scholar] [CrossRef] [PubMed]
- Hofman, A.; Jaddoe, V.W.; Mackenbach, J.P.; Moll, H.A.; Snijders, R.F.; Steegers, E.A.; Verhulst, F.C.; Witteman, J.C.; Buller, H.A. Growth, development and health from early fetal life until young adulthood: The Generation R Study. Paediatr. Perinat. Epidemiol. 2004, 18, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Jaddoe, V.W.; Mackenbach, J.P.; Moll, H.A.; Steegers, E.A.; Tiemeier, H.; Verhulst, F.C.; Witteman, J.C.; Hofman, A. The Generation R Study: Design and cohort profile. Eur. J. Epidemiol. 2006, 21, 475–484. [Google Scholar] [CrossRef]
- General Assembly of the World Medical, A. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. QualityMetric I, New England Medical Center H, Health Assessment, L. In SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales.; Lincoln, R.I., Ed.; QualityMetric Inc.; Health Assessment Lab: Boston, MA, USA, 2002. [Google Scholar]
- Wardlaw, T.M. Low Birthweight: Country, Regional and Global Estimates; UNICEF: New York, NY, USA, 2004. [Google Scholar]
- Verburg, B.O.; Steegers, E.A.; De Ridder, M.; Snijders, R.J.; Smith, E.; Hofman, A.; Moll, H.A.; Jaddoe, V.W.; Witteman, J.C. New charts for ultrasound dating of pregnancy and assessment of fetal growth: Longitudinal data from a population-based cohort study. Ultrasound Obstet. Gynecol. 2008, 31, 388–396. [Google Scholar] [CrossRef]
- Kramer, M.S.; Séguin, L.; Lydon, J.; Goulet, L. Socio-economic disparities in pregnancy outcome: Why do the poor fare so poorly? Paediatr. Perinat. Epidemiol. 2000, 14, 194–210. [Google Scholar] [CrossRef]
- Lumley, J.; Chamberlain, C.; Dowswell, T.; Oliver, S.; Oakley, L.; Watson, L. Interventions for promoting smoking cessation during pregnancy. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- Valero de Bernabé, J.; Soriano, T.; Albaladejo, R.; Juarranz, M.; Calle, M.a.E.; Martínez, D.; Domínguez-Rojas, V. Risk factors for low birth weight: A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116, 3–15. [Google Scholar] [CrossRef]
- Lagadec, N.; Steinecker, M.; Kapassi, A.; Magnier, A.M.; Chastang, J.; Robert, S.; Gaouaou, N.; Ibanez, G. Factors influencing the quality of life of pregnant women: A systematic review. BMC Pregnancy Childbirth 2018, 18, 455. [Google Scholar] [CrossRef] [PubMed]
- Bai, G.; Raat, H.; Jaddoe, V.W.V.; Mautner, E.; Korfage, I.J. Trajectories and predictors of women’s health-related quality of life during pregnancy: A large longitudinal cohort study. PLoS ONE 2018, 13, e0194999. [Google Scholar] [CrossRef] [PubMed]
- Bai, G.; Korfage, I.J.; Groen, E.H.-d.; Jaddoe, V.W.V.; Mautner, E.; Raat, H. Associations between Nausea, Vomiting, Fatigue and Health-Related Quality of Life of Women in Early Pregnancy: The Generation R Study. PLoS ONE 2016, 11, e0166133. [Google Scholar] [CrossRef] [PubMed]
- Statistics Netherlands. Migrants in the Netherlands 2004 (Allochtnen in Nederland 2004); Centraal Bureau voor de Statistiek: Voorburg/Heelen, the Netherlands, 2004. [Google Scholar]
- Statistics Netherlands. The Dutch Standard Classification of Education, SOI 2006; Centraal Bureau voor de Statistiek: Voorburg/Heelen, the Netherlands, 2008. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Jaddoe, V.W.; van Duijn, C.M.; Franco, O.H.; van der Heijden, A.J.; van Iizendoorn, M.H.; de Jongste, J.C.; van der Lugt, A.; Mackenbach, J.P.; Moll, H.A.; Raat, H.; et al. The Generation R Study: Design and cohort update 2012. Eur. J. Epidemiol. 2012, 27, 739–756. [Google Scholar] [CrossRef]
- Ludwig, D.S.; Currie, J. The Relationship Between Pregnancy Weight Gain and Birth Weight: A Within Family Comparison. Lancet 2010, 376, 984–990. [Google Scholar] [CrossRef]
- Lee, A.M.; Lam, S.K.; Sze Mun Lau, S.M.; Chong, C.S.; Chui, H.W.; Fong, D.Y. Prevalence, course, and risk factors for antenatal anxiety and depression. Obstet. Gynecol. 2007, 110, 1102–1112. [Google Scholar] [CrossRef]
- Bowen, A.; Bowen, R.; Butt, P.; Rahman, K.; Muhajarine, N. Patterns of depression and treatment in pregnant and postpartum women. Can. J. Psychiatry 2012, 57, 161–167. [Google Scholar] [CrossRef]
- Alder, J.; Fink, N.; Bitzer, J.; Hosli, I.; Holzgreve, W. Depression and anxiety during pregnancy: A risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. J. Matern.-Fetal Neonatal Med. 2007, 20, 189–209. [Google Scholar] [CrossRef]
- Feldman, P.J.; Dunkel-Schetter, C.; Sandman, C.A.; Wadhwa, P.D. Maternal Social Support Predicts Birth Weight and Fetal Growth in Human Pregnancy. Psychosom. Med. 2000, 62, 715–725. [Google Scholar] [CrossRef] [Green Version]
- Hedegaard, M.; Henriksen, T.B.; Sabroe, S.; Secher, N.J. Psychological distress in pregnancy and preterm delivery. BMJ 1993, 307, 234–239. [Google Scholar] [CrossRef]
- Glynn, L.M.; Schetter, C.D.; Hobel, C.J.; Sandman, C.A. Pattern of perceived stress and anxiety in pregnancy predicts preterm birth. Health Psychol. 2008, 27, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Generation R Next. Available online: https://www.generationr.nl/next/ (accessed on 31 October 2019).
- Chia, A.-R.; Chen, L.-W.; Lai, J.S.; Wong, C.H.; Neelakantan, N.; van Dam, R.M.; Chong, M.F.-F. Maternal Dietary Patterns and Birth Outcomes: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 685–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rush, D.; Stein, Z.; Susser, M. A Randomized Controlled Trial of Prenatal Nutritional Supplementation in New York City. Pediatrics 1980, 65, 683–697. [Google Scholar] [PubMed]
- Mathews, F.; Yudkin, P.; Neil, A. Influence of maternal nutrition on outcome of pregnancy: Prospective cohort study. BMJ 1999, 319, 339–343. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables. | Values * |
|---|---|
| Maternal age at enrolment (years), mean (SD) | 29.9 (5.2) |
| Gestational age at enrolment (weeks), mean (SD) | 15.0 (4.0) |
| Parity, number (%) | |
| Nulliparous | 3679 (58.2) |
| Multiparous | 2642 (41.8) |
| Missing | 13 |
| Educational level, number (%) | |
| High education | 1563 (25.1) |
| Mid-high | 1234 (19.8) |
| Mid-low | 1929 (30.9) |
| Low | 1507 (24.2) |
| Missing | 101 |
| Ethnic background, number (%) | |
| Dutch | 3375 (53.5) |
| Non-Dutch, Western | 552 (8.8) |
| Non-Dutch, non-Western | 2378 (37.7) |
| Missing | 29 |
| Body mass index at enrolment, mean (SD) | 24.7 (4.5) |
| Missing | 29 |
| Maternal smoking in early pregnancy, number (%) | |
| Never smoking | 4738 (75.9) |
| Stopped smoking when the pregnancy was known | 761 (12.2) |
| Continuing smoking in pregnancy | 746 (11.9) |
| Missing | 89 |
| HRQoL score, SF-12 | |
| Physical component summary score, mean (SD) | 47.6 (9.1) |
| Mental component summary score, mean (SD) | 48.7 (10.4) |
| Birth outcomes | |
| Pregnancy duration (weeks), number (%) | 39.9 (1.7) |
| Preterm birth (yes), number (%) | 331 (5.2) |
| Birth weight (grams), mean (SD) | 3428 (558) |
| Low birth weight (yes), number (%) | 290 (4.6) |
| Small for gestational age (yes), number (%) | 604 (9.5) |
| Pregnancy Duration | Preterm Birth | Birth Weight | Low Birth Weight | Small Size for Gestational Age | |
|---|---|---|---|---|---|
| B (95% CI) | Exp (B) (95%CI) | B (95% CI) | Exp (B) (95%CI) | Exp (B) (95%CI) | |
| HRQoL in early pregnancy | |||||
| PCS score | 0.05 (0.00, 0.10) | 0.96 (0.85, 1.08) | −4.57 (−19.55, 10.42) | 1.07 (0.94, 1.23) | 1.05 (0.96, 1.16) |
| MCS score | 0.01 (−0.03, 0.06) | 0.90 (0.82, 1.00) | 7.90 (−5.62, 21.42) | 0.96 (0.86, 1.08) | 1.02 (0.94, 1.10) |
| HRQoL in mid-pregnancy | |||||
| PCS score | 0.004 (−0.001, 0.008) | 0.99 (0.98, 1.00) | −0.45 (−1.92, 1.03) | 1.00 (0.99, 1.01) | 1.00 (0.99, 1.01) |
| MCS score | −0.002 (−0.007, 0.002) | 1.00 (0.99, 1.02) | 0.44 (−1.92, 1.05) | 1.00 (0.99, 1.02) | 1.00 (0.99, 1.01) |
| HRQoL in late pregnancy | |||||
| PCS score | 0.08 (0.03, 0.13) | 0.90 (0.79, 1.03) | −18.10 (−33.43, −2.78) | 1.01 (0.88, 1.17) | 1.20 (1.08, 1.33) * |
| MCS score | 0.007 (−0.04, 0.05) | 0.96 (0.85, 1.09) | 14.06 (0.01, 28.10) | 0.96 (0.85, 1.09) | 0.93 (0.85, 1.01) |
| Pregnancy Duration | Preterm Birth | Birth Weight | Low Birth Weight | Small for Gestational Age | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | p value | effect size | Yes (%) | No (%) | p value | Mean (SD) | p value | effect size | Yes (%) | No (%) | p value | Yes (%) | No (%) | p value | |
| PCS score in early pregnancy | |||||||||||||||
| <10th (n = 634) | 39.8 (1.8) | 0.18 | 0.06 | 32 (5.0) | 602 (95.0) | 0.60 | 3425 (559) | 0.81 | 0.01 | 24 (3.8) | 610 (96.2) | 0.42 | 56 (8.8) | 578 (91.2) | 0.70 |
| >90th (n = 686) | 39.9 (1.8) | 30 (4.4) | 656 (95.6) | 3418 (551) | 33 (4.8) | 653 (95.2) | 65 (9.5) | 621 (90.5) | |||||||
| MCS score in early pregnancy | |||||||||||||||
| <10th (n = 633) | 39.8 (1.8) | 0.31 | 0.06 | 40 (6.3) | 593 (93.7) | 0.55 | 3351 (550) | 0.005 | 0.15 | 36 (5.7) | 597 (94.3) | 0.81 | 68 (10.7) | 565 (89.3) | 0.46 |
| >90th (n = 640) | 39.9 (1.8) | 35 (5.5) | 605 (94.5) | 3440 (582) | 34 (5.3) | 606 (94.7) | 60 (9.4) | 580 (90.6) | |||||||
| PCS score in mid-pregnancy | |||||||||||||||
| <10th (n = 621) | 39.8 (1.7) | 0.01 | 0.12 | 38 (6.1) | 583 (93.9) | 0.03 | 3444 (555) | 0.71 | 0.02 | 27 (4.3) | 594 (95.7) | 0.47 | 53 (8.5) | 568 (91.5) | 0.61 |
| >90th (n = 622) | 40.0 (1.6) | 22 (3.5) | 600 (90.5) | 3433 (513) | 22 (3.5) | 600 (96.5) | 48 (7.7) | 574 (92.3) | |||||||
| MCS score in mid-pregnancy | |||||||||||||||
| <10th (n = 621) | 39.8 (1.8) | 0.08 | 0.11 | 40 (6.4) | 581 (93.6) | 0.17 | 3376 (546) | 0.001 | 0.18 | 27 (4.3) | 594 (95.7) | 0.23 | 62 (10.0) | 559 (90.0) | 0.04 |
| >90th (n = 631) | 40.0 (1.5) | 29 (4.6) | 602 (95.4) | 3474 (518) | 19 (3.0) | 612 (97.0) | 42 (6.7) | 589 (93.3) | |||||||
| PCS score in late-pregnancy | |||||||||||||||
| <10th (n = 604) | 39.7 (1.6) | 0.01 | 0.18 | 36 (6.0) | 568 (94.0) | 0.62 | 3480 (564) | 0.01 | 0.15 | 27 (4.5) | 577 (95.5) | 0.79 | 45 (7.5) | 559 (92.5) | 0.005 |
| >90th (n = 608) | 40.0 (1.7) | 32 (5.3) | 576 (94.7) | 3397 (563) | 30 (4.7) | 578 (95.1) | 75 (12.3) | 533 (87.7) | |||||||
| MCS score in late-pregnancy | |||||||||||||||
| <10th (n = 604) | 39.9 (1.7) | 0.07 | 0.06 | 35 (5.8) | 569 (94.2) | 0.08 | 3344 (542) | <0.001 | 0.24 | 30 (5.0) | 574 (95.0) | 0.15 | 74 (12.3) | 530 (87.7) | 0.001 |
| >90th (n = 605) | 40.0 (1.5) | 22 (3.6) | 583 (96.4) | 3474 (524) | 20 (3.3) | 585 (96.7) | 39 (6.4) | 566 (93.6) | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, G.; Korfage, I.J.; Mautner, E.; Raat, H. Associations between Maternal Health-Related Quality of Life during Pregnancy and Birth Outcomes: The Generation R Study. Int. J. Environ. Res. Public Health 2019, 16, 4243. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214243
Bai G, Korfage IJ, Mautner E, Raat H. Associations between Maternal Health-Related Quality of Life during Pregnancy and Birth Outcomes: The Generation R Study. International Journal of Environmental Research and Public Health. 2019; 16(21):4243. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214243
Chicago/Turabian StyleBai, Guannan, Ida J Korfage, Eva Mautner, and Hein Raat. 2019. "Associations between Maternal Health-Related Quality of Life during Pregnancy and Birth Outcomes: The Generation R Study" International Journal of Environmental Research and Public Health 16, no. 21: 4243. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214243