Evaluation of the Effectiveness of Mobile App-Based Stress-Management Program: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
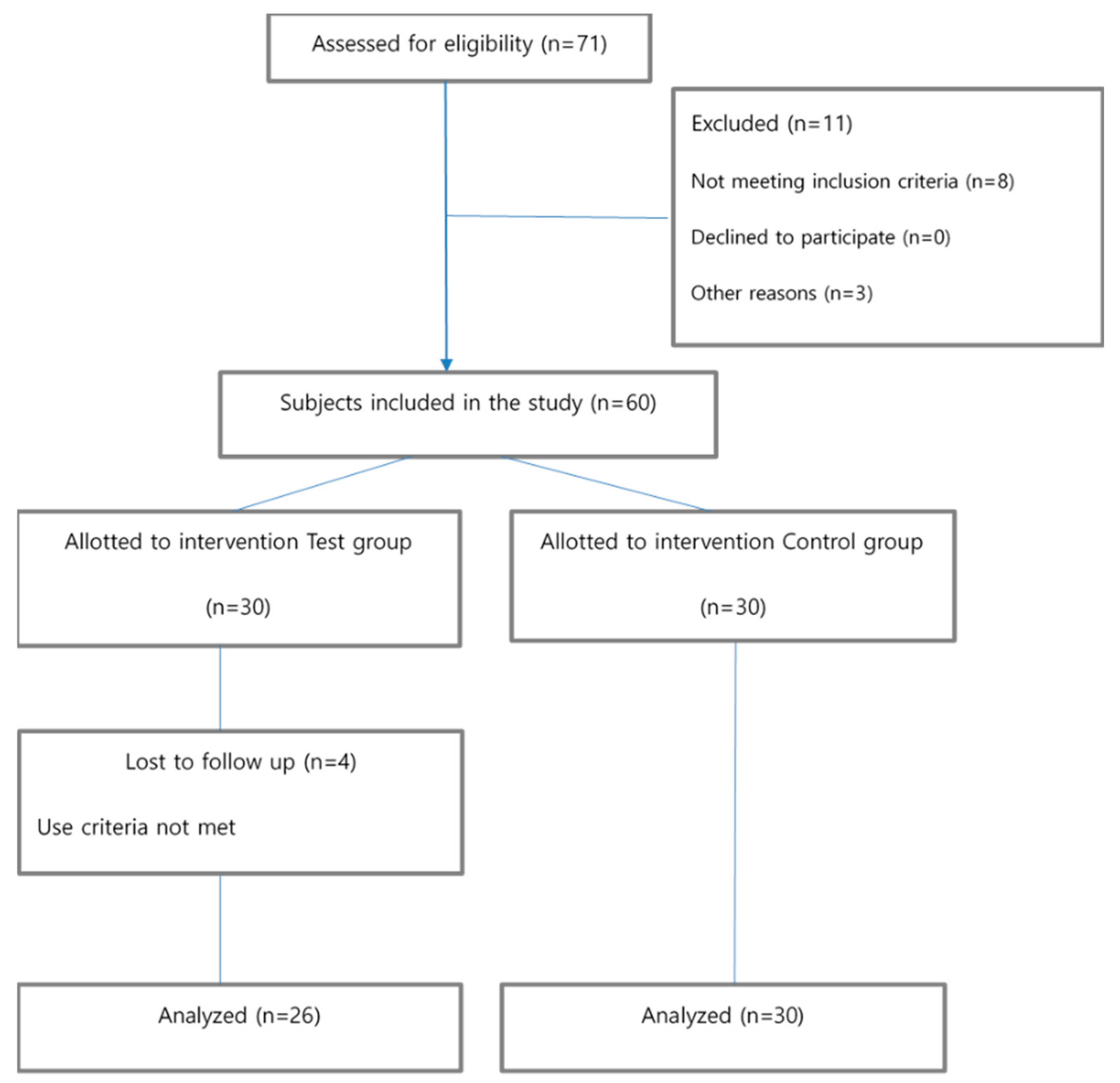
2.2. Subjects and Experimental Procedures
2.3. Outcome Measures
2.3.1. Perceived Stress and Job Stress
2.3.2. Depression
2.3.3. Anxiety
2.3.4. Emotional Labor
2.3.5. Well-Being
2.3.6. Self-Efficacy
2.3.7. App Satisfaction
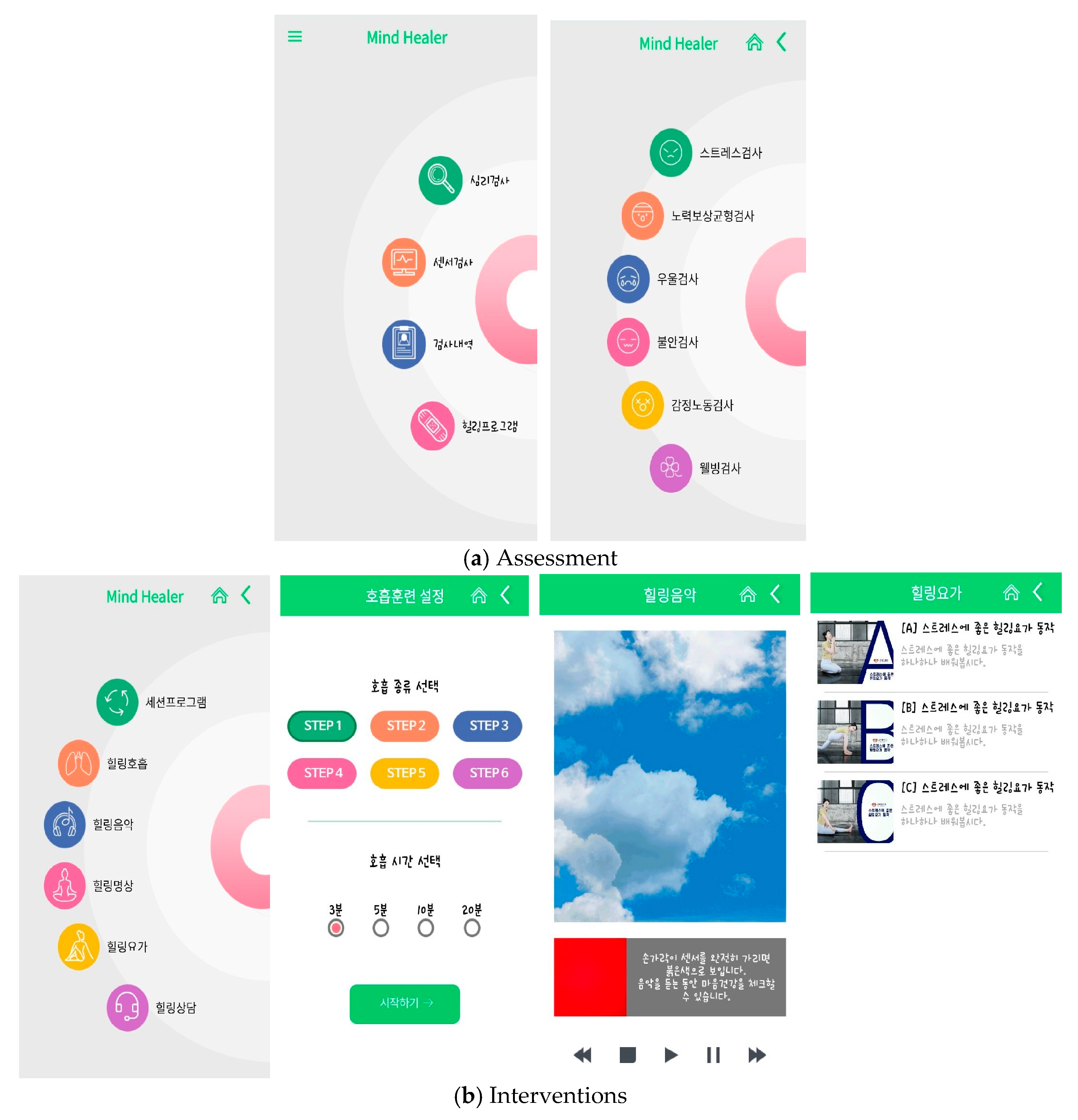
2.4. App Development
2.5. Analytical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Levy, D. Emerging mHealth: Paths for Growth. A Global Research Study About the Opportunities and Challenges of Mobile Health from the Perspective of Patients, Payers and Providers. PricewaterhouseCoopers (PWC) 2012. Available online: http://www.pwc.com/en_GX/gx/healthcare/mhealth/assets/pwc-emerging-mhealth-full.pdf (accessed on 10 September 2019).
- Leigh, S.; Flatt, S. App-based psychological interventions: Friend or foe? Evid. Based Ment. Health 2015, 18, 97. [Google Scholar] [CrossRef]
- Commission, E. Green paper on mobile health (m-Health). 2014, Internet: European Commission. Available online: https://ec.europa.eu/digital-agenda/en/news/green-paper-mobile-health-mhealth (accessed on 10 November 2016).
- Boulos, M.N.K.; Brewer, A.C.; Karimkhani, C.; Buller, D.B.; Dellavalle, R.P. Mobile medical and health apps: State of the art, concerns, regulatory control and certification. Online J. Public Health Inform. 2014, 5, 229. [Google Scholar] [PubMed]
- APAC. Mobile Apps in APAC 2016 Report. Available online: http://apacthinkwithgooglecom/articles/mobile-apps-in-apac-2016-reporthtml (accessed on 20 September 2019 ).
- Welfare MoHa. 2016 The Survey of Mental Disorders in Korea; Welfare MoHa: Seoul, Korea, 2017. [Google Scholar]
- Song, S.-M. Stress Management: Health Consequences and Policy Implications. Korea Health Promot. Forum 2017, 4, 4–17. [Google Scholar]
- WHO. International Classification of Diseases, 10th ed.; WHO: Geneva, Swizerland, 1948. [Google Scholar]
- Jina, J.; Min-Hee, L.; Jin-Ho, K. Recent Changes in Mental Health Policy in Korea. Health Welf. Forum 2017, 246, 51–63. [Google Scholar]
- Center SMHaW. Seoul Citizens’ Perception Survey Report on Mental Health. Seoul Ment. Health Stat. 2017. Available online: http://seoulmentalhealth.kr/dataroom/report.jsp?cmd=view&test_num=90 (accessed on 2 November 2019).
- Hwang, W.J.; Kim, J.A.; Rankin, S. Depressive symptom and related factors: A cross-sectional study of Korean female workers working at traditional markets. Int. J. Environ. Res. Public Health 2017, 14, 1465. [Google Scholar] [CrossRef]
- Luxton, D.D.; McCann, R.A.; Bush, N.E.; Mishkind, M.C.; Reger, G.M. mHealth for mental health: Integrating smartphone technology in behavioral healthcare. Prof. Psychol. Res. Pract. 2011, 42, 505. [Google Scholar] [CrossRef]
- Zapata, B.C.; Fernández-Alemán, J.L.; Idri, A.; Toval, A. Empirical studies on usability of mHealth apps: A systematic literature review. J. Med Syst. 2015, 39, 1. [Google Scholar] [CrossRef]
- WHO. Mental health: A state of well-being. Available online: http://wwwwhoint/features/factfiles/mental_health/en/ (accessed on 2 October 2019).
- Chan, S.R.; Torous, J.; Hinton, L.; Yellowlees, P. Mobile tele-mental health: Increasing applications and a move to hybrid models of care. Healthcare 2014, 2, 220–233. [Google Scholar] [CrossRef]
- An, S.; Lee, H. Use of Mobile Mental Health Application for Mental Health Promotion: Based on the Information-Motivation-Behavioral Skills Model. Korean J. Commun. Stud. 2018, 62, 167–194. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.J.; Koh, S.B.; Kang, D.; Kim, S.A.; Kang, M.G.; Lee, C.G.; Kim, J.W. Developing an occupational stress scale for Korean employees. Korean J. Occup. Environ. Med. 2005, 17, 297–317. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Lee, J.; Han E-m Hong, H.; Lee, I. Validation of the Korean Version of the Emotional Labor Scale (ELS). Korean Psychol. Assoc. 2016, 21, 243–256. [Google Scholar]
- Bech, P. Measuring the dimension of psychological general well-being by the WHO-5. Qual. Life Newsl. 2004, 32, 15–16. [Google Scholar]
- World Health Organization. Use of well-being measures in primary health care-the DepCare project health for all. Target 1998, 12, E60246. [Google Scholar]
- Schwarzer, R.; Born, A.; Iwawaki, S.; Lee, Y.-M. The assessment of optimistic self-beliefs: Comparison of the Chinese, Indonesian, Japanese, and Korean versions of the General Self-Efficacy scale. Psychol. Int. J. Psychol. Orient. 1997, 40, 1–13. [Google Scholar]
- Carissoli, C.; Villani, D.; Riva, G. Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 46–53. [Google Scholar] [CrossRef]
- Holkup, P.A. Evidence-based protocol: Elderly suicide-secondary prevention. J. Gerontol. Nurs. 2003, 29, 6–9. [Google Scholar] [CrossRef]
- Cole, D.A.; Nolen-Hoeksema, S.; Girgus, J.; Paul, G. Stress exposure and stress generation in child and adolescent depression: A latent trait-state-error approach to longitudinal analyses. J. Abnorm. Psychol. 2006, 115, 40. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.; Cheon, M.; Hong, H. A meta-analysis on the effect of the workplace stress management program. Korean J. Couns. 2016, 17, 487–512. [Google Scholar] [CrossRef]
- Cuijpers, P.; Marks, I.M.; van Straten, A.; Cavanagh, K.; Gega, L.; Andersson, G. Computer-aided psychotherapy for anxiety disorders: A meta-analytic review. Cogn. Behav. Ther. 2009, 38, 66–82. [Google Scholar] [CrossRef] [PubMed]
- Villani, D.; Riva, G. Does interactive media enhance the management of stress? Suggestions from a controlled study. Cyberpsychology Behav. Soc. Netw. 2012, 15, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Villani, D.; Grassi, A.; Cognetta, C.; Toniolo, D.; Cipresso, P.; Riva, G. Self-help stress management training through mobile phones: An experience with oncology nurses. Psychol. Serv. 2013, 10, 315. [Google Scholar] [CrossRef]
- Nilsson, U. The anxiety-and pain-reducing effects of music interventions: A systematic review. AORN J. 2008, 87, 780–807. [Google Scholar] [CrossRef]
- Ahtinen, A.; Mattila, E.; Välkkynen, P.; Kaipainen, K.; Vanhala, T.; Ermes, M.; Lappalainen, R. Mobile mental wellness training for stress management: Feasibility and design implications based on a one-month field study. JMIR mHealth uHealth 2013, 1, e11. [Google Scholar] [CrossRef]
- Zeidan, F.; Johnson, S.K.; Gordon, N.S.; Goolkasian, P. Effects of brief and sham mindfulness meditation on mood and cardiovascular variables. J. Altern. Complement. Med. 2010, 16, 867–873. [Google Scholar] [CrossRef]
- Hammen, C. Generation of stress in the course of unipolar depression. J. Abnorm. Psychol. 1991, 100, 555. [Google Scholar] [CrossRef]
- Endler, N.S. Stress, Anxiety and coping: The multidimensional interaction model. Can. Psychol. Psychol. Can. 1997, 38, 136. [Google Scholar] [CrossRef]
- Wahle, F.; Kowatsch, T.; Fleisch, E.; Rufer, M.; Weidt, S. Mobile sensing and support for people with depression: A pilot trial in the wild. JMIR mHealth uHealth 2016, 4, e111. [Google Scholar] [CrossRef] [PubMed]
- Shen, N.; Levitan, M.J.; Johnson, A.; Bender, J.L.; Hamilton-Page, M.; Jadad, A.A.R.; Wiljer, D. Finding a depression app: A review and content analysis of the depression app marketplace. JMIR mHealth uHealth 2015, 3, e16. [Google Scholar] [CrossRef] [PubMed]
- Huguet, A.; Rao, S.; McGrath, P.J.; Wozney, L.; Wheaton, M.; Conrod, J.; Rozario, S. A systematic review of cognitive behavioral therapy and behavioral activation apps for depression. PLoS ONE 2016, 11, e0154248. [Google Scholar] [CrossRef] [PubMed]
- Pisaniello, S.L.; Winefield, H.R.; Delfabbro, P.H. The influence of emotional labour and emotional work on the occupational health and wellbeing of South Australian hospital nurses. J. Vocat. Behav. 2012, 80, 579–591. [Google Scholar] [CrossRef]
- Parks, A.C.; Della Porta, M.D.; Pierce, R.S.; Zilca, R.; Lyubomirsky, S. Pursuing happiness in everyday life: The characteristics and behaviors of online happiness seekers. Emotion 2012, 12, 1222. [Google Scholar] [CrossRef]
- Lee, K.-H.; Song, J.-S. The effect of emotional intelligence on self-efficacy and job stress of nurses-mediating role of self-efficacy. J. Korean Acad. Nurs. Adm. 2010, 16, 17–25. [Google Scholar] [CrossRef]
- Yu, S.-Y.; Suh, E.E. Conditional Effect of Years Employed in Self-efficacy and Stress among Studying Clinical Nurses: An Exploratory Mixed Method Study. Korean J. Adult Nurs. 2019, 31, 303–314. [Google Scholar] [CrossRef]
- Tam, C.; Santos, D.; Oliveira, T. Exploring the influential factors of continuance intention to use mobile Apps: Extending the expectation confirmation model. Inf. Syst. Front. 2018, 1–15. [Google Scholar] [CrossRef]
- Park, D.-J.; Choi, J.-H.; Kim, D.-J. The Influence of Health Apps Efficacy, Satisfaction and Continued Use Intention on Wearable Device Adoption: A Convergence Perspective. J. Digit. Converg. 2015, 13, 137–145. [Google Scholar] [CrossRef]
- Lee Ls Lee, S.H.; Jeong, J.S.; Noh, K.Y. Psychological Factors Influencing Continuous Use of Mobile Healthcare Applications. Soc. Digit. Policy Manag. 2017, 15, 445–456. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | N (%) | Experimental Group (N = 26) | Control Group (N = 30) | χ2/Z | p-Value |
|---|---|---|---|---|---|---|
| Sex | Male | 3 (5.4) | 1 | 2 | −0.463 | 0.643 |
| Female | 53 (94.6) | 25 | 28 | |||
| Age (years) | <30 a | 14 (25) | 4 | 10 | 1.307 | 0.279 |
| 31–40 a | 30 (53.5) | 15 | 15 | |||
| >40 a | 12 (21.5) | 7 | 5 | |||
| Marital status | Unmarried | 27 (48.2) | 11 | 16 | −0.816 | 0.414 |
| Married | 29 (51.8) | 15 | 14 | |||
| Educational attainment | College | 26 (46.4) | 16 | 18 | −0.117 | 0.907 |
| >College | 30 (53.6) | 10 | 12 | |||
| Income (won millions) | <200 a | 4 (7.2) | 2 | 2 | 0.158 | 0.854 |
| 201–400 a | 26 (46.4) | 11 | 15 | |||
| >400 a | 26 (46.4) | 13 | 13 |
| Variable | Experimental Group (N = 26) M ± SD | Control Group (N = 30) M ± SD | Z-Value | p-Value | |
|---|---|---|---|---|---|
| Perceived health | Physical health | 3.27 ± 0.72 | 3.23 ± 0.82 | −0.080 | 0.936 |
| Mental health | 3.42 ± 0.76 | 3.30 ± 0.75 | 0.493 | 0.622 | |
| Stress | PSS 1 | 20.00 ± 4.18 | 18.63 ± 3.72 | −0.933 | 0.351 |
| KOSS 2 | 2.53 ± 0.31 | 2.53 ± 0.27 | −0.198 | 0.843 | |
| Depression | 7.11 ± 4.49 | 7.53 ± 6.14 | −0.025 | 0.980 | |
| Anxiety | 4.26 ± 3.42 | 4.40 ± 4.34 | −0.306 | 0.759 | |
| Emotional labor | 2.88 ± 0.41 | 2.81 ± 0.32 | −0.617 | 0.537 | |
| Well-being | 2.06 ± 0.98 | 2.20 ± 0.95 | −0.396 | 0.692 | |
| Self-efficacy | 2.70 ± 0.45 | 2.76 ± 0.40 | −0.058 | 0.954 | |
| Variable | Group | Pretest EM 1 ± SE | Posttest EM ± SE | Source | F-Value | p-Value | |
|---|---|---|---|---|---|---|---|
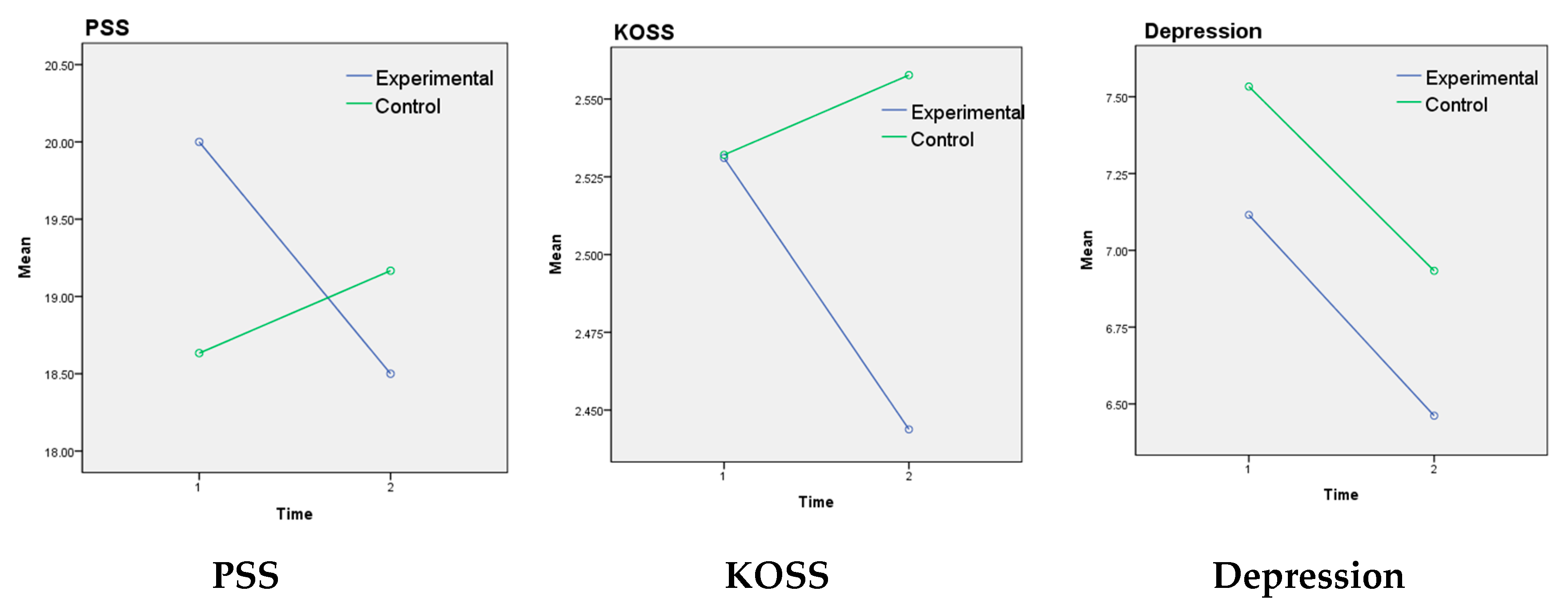
| Stress | PSS | Experimental | 20.00 ± 0.77 | 18.50 ± 0.70 | Group Time Group*Time | 0.172 0.754 3.33 | 0.680 0.389 0.037 † |
| md 2 = 1.50, p = 0.035 | |||||||
| Control | 18.63 ± 0.72 | 19.16 ± 0.65 | |||||
| md = −0.533, p = 0.485 | |||||||
| KOSS | Experimental | 2.53 ± 0.05 | 2.44 ± 0.05 | Group Time Group*Time | 0.645 1.18 3.97 | 0.425 0.282 0.050 | |
| md = 0.087, p = 0.040 | |||||||
| Control | 2.53 ± 0.05 | 2.55 ± 0.05 | |||||
| md = −0.026, p = 0.51 | |||||||
| Depression | Experimental | 7.11 ± 1.06 | 6.46 ± 0.98 | Group Time Group*Time | 0.117 1.440 0.003 | 0.734 0.235 0.959 | |
| md = 0.654, p = 0.396 | |||||||
| Control | 7.53 ± 0.99 | 6.93 ± 0.91 | |||||
| md = 0.600, p = 0.403 | |||||||
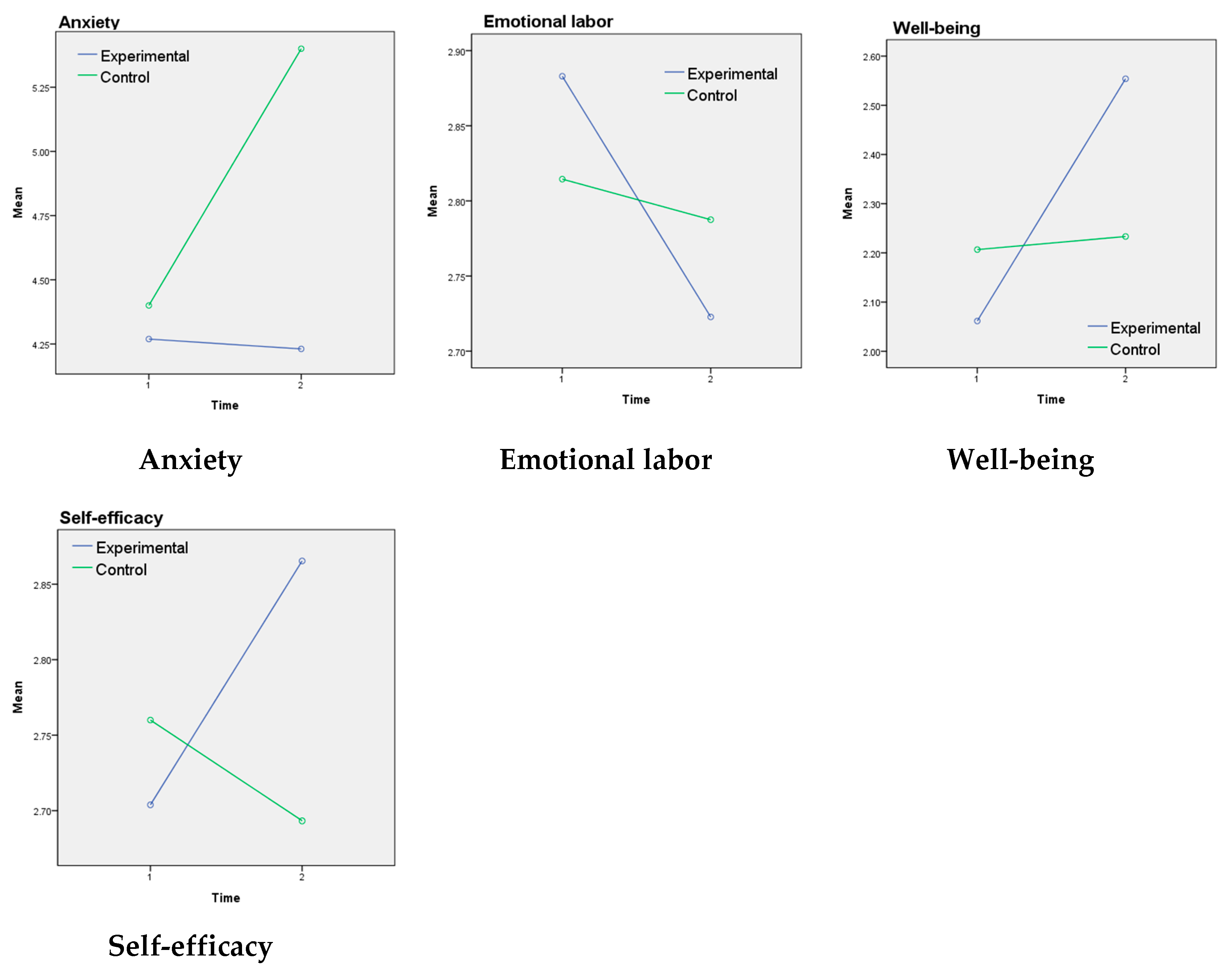
| Anxiety | Experimental | 4.26 ± 0.77 | 4.23 ± 0.86 | Group Time Group*Time | 0.412 1.040 1.212 | 0.524 0.312 0.276 | |
| md = 0.038, p = 0.966 | |||||||
| Control | 4.40 ± 0.72 | 5.40 ± 0.80 | |||||
| md = −1.00, p = 0.126 | |||||||
| Emotional labor | Experimental | 2.88 ± 0.07 | 2.72 ± 0.08 | Group Time Group*Time | 0.000 3.76 1.91 | 0.980 0.580 0.173 | |
| md = 0.160, p = 0.027 | |||||||
| Control | 2.81 ± 0.06 | 2.78 ± 0.07 | |||||
| md = 0.027, p = 0.683 | |||||||
| Well-being | Experimental | 2.06 ± 0.19 | 2.55 ± 0.20 | Group Time Group*Time | 0.133 5.06 4.07 | 0.717 0.029 0.048 | |
| md = −0.492, p = 0.005 | |||||||
| Control | 2.20 ± 0.17 | 2.23 ± 0.18 | |||||
| md = −0.027, p = 0.866 | |||||||
| Self-efficacy | Experimental | 2.70 ± 0.08 | 2.86 ± 0.08 | Group Time Group*Time | 0.094 0.977 5.65 | 0.000 0.327 0.021 | |
| md = −0.162, p = 0.025 | |||||||
| Control | 2.76 ± 0.07 | 2.69 ± 0.08 | |||||
| md = 0.067, p = 0.313 | |||||||
| Satisfaction Item | N (%) | Users’ Experience | |
|---|---|---|---|
| Satisfaction with the app | Dissatisfied | 8 (30.8) |
|
| Satisfied | 18 (69.2) | ||
| Does this app raise your stress management awareness? | Decreased | 0 (0) | |
| No change | 11(42.3) | ||
| Improved | 15 (57.7) | ||
| Does this app increase your stress management knowledge? | Decreased | 2 (7.7) | |
| No change | 12 (46.2) | ||
| Improved | 12 (46.2) | ||
| Does this app improve your attitude toward stress management? | Decreased | 2 (7.7) | |
| No change | 10 (38.5) | ||
| Improved | 14 (53.8) | ||
| Does this app provide stress motivation for management? | Decreased | 0 (0) | |
| No change | 10 (38.5) | ||
| Improved | 16 (61.5) | ||
| Does this app bring behavioral change in stress management? | Decreased | 4 (15.4) | |
| No change | 10 (38.5) | ||
| Improved | 12 (46.1) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, W.J.; Jo, H.H. Evaluation of the Effectiveness of Mobile App-Based Stress-Management Program: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4270. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214270
Hwang WJ, Jo HH. Evaluation of the Effectiveness of Mobile App-Based Stress-Management Program: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(21):4270. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214270
Chicago/Turabian StyleHwang, Won Ju, and Hyun Hee Jo. 2019. "Evaluation of the Effectiveness of Mobile App-Based Stress-Management Program: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 21: 4270. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16214270