Concentration of Healthcare Resources in China: The Spatial–Temporal Evolution and Its Spatial Drivers

Abstract
:1. Introduction
2. Methodology
2.1. Measuring HCR Concentration in China
2.2. Verification of Spatial Correlation
2.3. Types of Spatial Econometric Models and Model Construction
2.4. Variable Selection
2.5. Data Source
3. Empirical Analysis
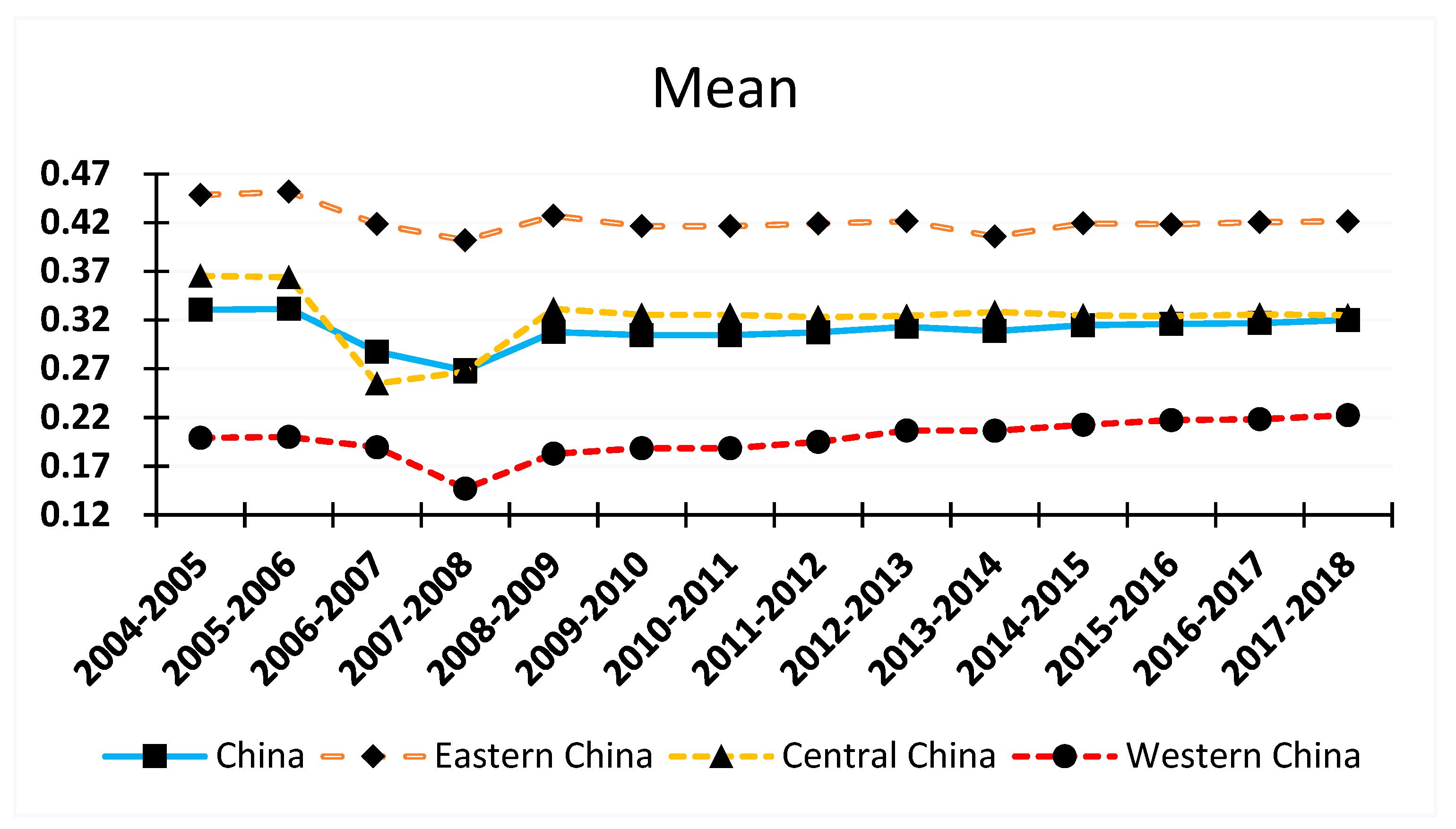
3.1. The Spatial–Temporal Evolution of HCR Concentration in China
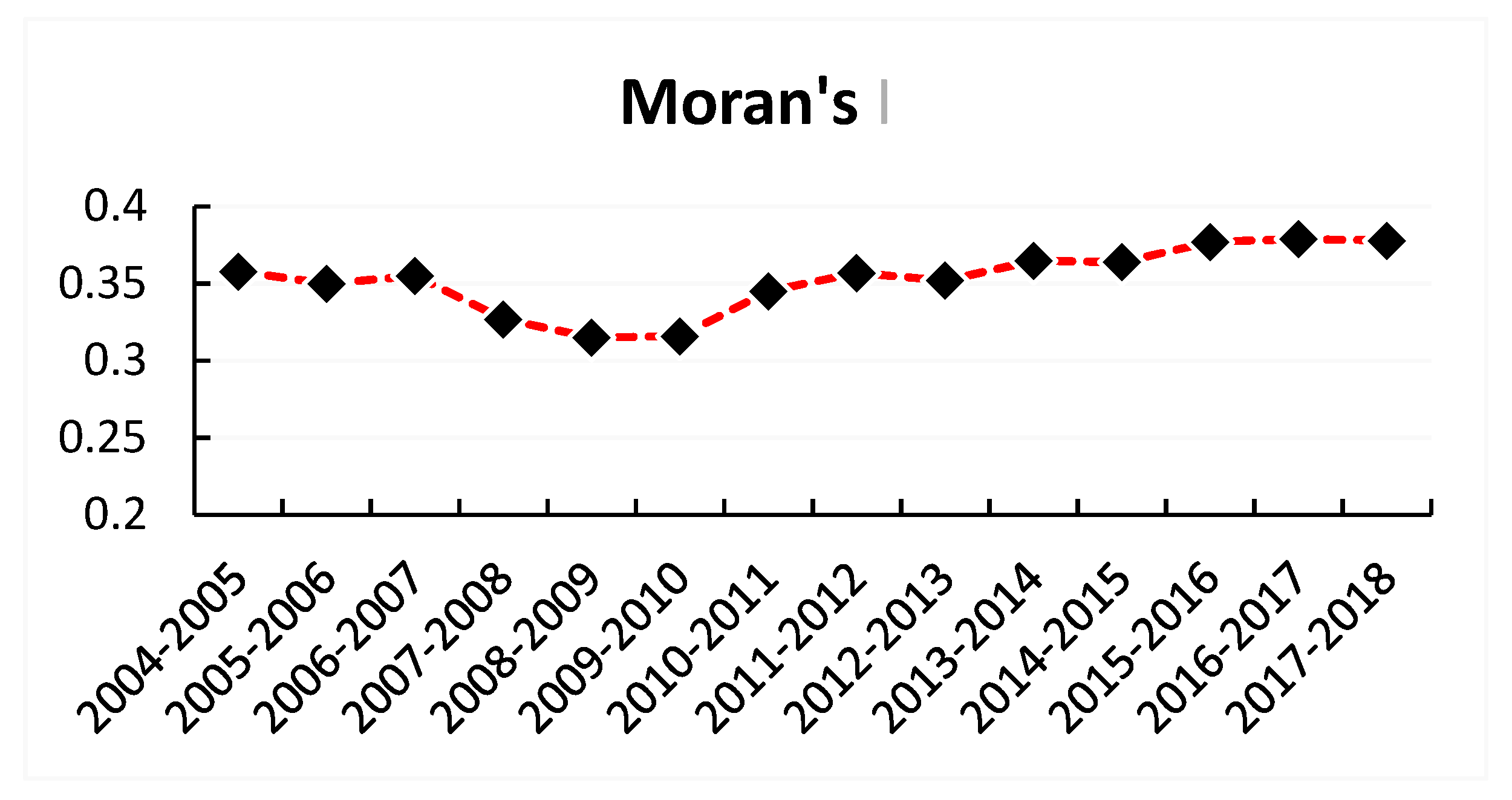
3.2. Spatial Correlation Analysis of HCR concentration in China
3.3. Determining the Spatial Econometric Model for HCR concentration in China
3.4. Robustness Test
4. Conclusions and Suggestions
Author Contributions
Funding
Conflicts of Interest
References
- Linda, D.; Fiona, C. Human Resources for Health in Fragile States. Lancet 2008, 2, 626–627. [Google Scholar]
- Winnie, C.M.; William, H.; Meng, Q.Y.; Chen, W.; Sun, X. Realignment of Incentives for Healthcare Providers in China. Lancet 2010, 375, 1120–1130. [Google Scholar]
- Fraser, B. Human Resources for Health in the Americas. Lancet 2007, 1, 179–180. [Google Scholar] [CrossRef]
- Weon-young, L.; Ian, S. The impact of Out-Of-Pocket Payments on Health Care Inequity: The Case of National Health Insurance in South Korea. Int. J. Environ. Res. Public Health 2014, 7, 7304–7318. [Google Scholar]
- William, D.; David, D.; Amy, L.; Fan, V. Political and Economic Aspects of the Transition to Universal Health Coverage. Lancet 2012, 380, 924–932. [Google Scholar]
- Winnie, C.M.; William, C.H.; Wen, C.; Hu, S.; Ma, J.; Maynard, A. Early Appraisal of China’s Huge and Complex Healthcare Reforms. Lancet 2012, 379, 833–842. [Google Scholar]
- Meng, Q.; Xu, L.; Zhang, Y.G.; Qian, J.; Cai, M.; Xin, Y.; Gao, J.; Xu, K.; Boerma, J.T.; Barber, S.L. Trends in Access to Health Services and Financial Protection in China between 2003 and 2011: A Cross-Sectional Study. Lancet 2012, 379, 805–814. [Google Scholar] [CrossRef]
- Hu, H.M.; Chen, D.W.; Gao, Q.S. Evaluation on Health Resources Allocation in Zhejiang Based on Agglomeration Degree. Chin. Health Econ. 2016, 7, 56–59. [Google Scholar]
- Gong, H.X.; Wu, Z.Y.; Wu, B.L.; Luo, Z.N. Analysis on Spatial Aggregation Feature of Health Resources in Guangdong. Chin. Health Econ. 2017, 5, 52–55. [Google Scholar]
- Tang, Q.M.; Nie, J. Research on the Medical Investment Gap, Medical Development Indexes and the Influencing Factors of the Western Region. Chin. J. Health Stat. 2015, 4, 47–49. [Google Scholar]
- Song, S.H.; Yuan, B.B.; Zhang, L.Y.; Cheng, G.; Zhu, W.; Hou, Z.; He, L.; Ma, X.; Meng, Q. Increased Inequalities in Health Resource and Access to Health Care in Rural China. Int. J. Environ. Res. Public Health 2019, 1, 49. [Google Scholar] [CrossRef] [PubMed]
- Romanillos, T.; Maneja, R.; Varga, D.; Badiella, L.; Boada, M. Protected natural Areas: In Sickness and in Health. Int. J. Environ. Res. Public Health 2018, 15, 2182. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Fan, V.Y.; Zhang, J.; Zhang, L.; Ke, Y.; Dong, Z.; Chen, L.C. China’s Human Resources for Health: Quantity, Quality and Distribution. Lancet 2008, 372, 1774–1781. [Google Scholar] [CrossRef]
- Wang, W.H.; Ekaterina, L.; Emilie, D. Public Hospitals in China is There a Variation in Patient Experience with Inpatient Care. Int. J. Environ. Res. Public Health 2019, 2, 193. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Coulter, A.; Bruster, S. The Picker Patient Experience Questionnaire: Development and Validation Using Data from In-Patient Surveys in Five Countries. Int. J. Qual. Health Care 2002, 14, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Coulter, A.; Reeves, R.; Bruster, S.; Richards, N. Properties of the Picker Patient Experience Questionnaire in a Randomized Controlled Trial of Long Versus Short Form Survey Instruments. J. Public Health Med. 2003, 25, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.P.; Park, I.Y.; Kwun, Y.C.; Tan, X. Extension of the TOPSIS Method for Decision-Making Problems under Interval-Valued Intuitionistic Fuzzy Environment. Appl. Math. Model. 2011, 5, 2544–2556. [Google Scholar]
- Wei, F.Q.; Ma, J. Analysis of the Agglomeration Degree of Health Resources in Traditional Chinese Medicine. Chin. J. Hosp. Adm. 2016, 10, 789–792. [Google Scholar]
- Wang, Y.; Fan, J.J.; Zhao, J.; Dong, Y.; Wang, Z.X. Spatial Analysis on the Utilization Efficiency of Health Resources Allocation in Shandong Province. Chin. J. Health Stat. 2015, 6, 1056–1058. [Google Scholar]
- Cummins, S.; Curtis, S.; Diez-oux, A.V.; Macintyre, S. Understanding and Representing, Pace in Health Research: A Relational Approach. Soc. Sci. Med. 2007, 9, 1825–1838. [Google Scholar] [CrossRef]
- Propper, C.; Upward, R. Need, Equity and the NHS: The Distribution of Health Care Expenditure 1974–1987. Fisc. Stud. 1992, 2, 1–21. [Google Scholar] [CrossRef]
- Xie, H.M.; Pan, J. An Overview of Measurement Methods for Spatial Accessibility of Health Services. Chin. J. Health Stat. 2016, 2, 353–356. [Google Scholar]
- Lesage, J.; Pace, R.K. Introduction to Spatial Econometrics; CRC Press: Baca Raton, FL, USA, 2009; pp. 189–210. [Google Scholar]
- Corrado, L.; Fingleton, B. Where is the Economics in Spatial Economics? J. Reg. Sci. 2012, 2, 210–239. [Google Scholar] [CrossRef]
- Elhorst, J.P. Applied Spatial Economics: Raising the Bar. Spat. Econ. Anal. 2010, 1, 9–28. [Google Scholar] [CrossRef]
- Lee, L.F.; Yu, J. Estimation of Spatial Autoregressive Panel Data Models with Fixed Effects. J. Econom. 2010, 2, 165–185. [Google Scholar] [CrossRef]
- Yu, J.N. Utilization Efficiency and Spatial Spillover Effect of Health Resources among Provinces in China. J. Guizhou Univ. 2017, 5, 63–69. [Google Scholar]
- Adolf, W. Marshall’s Principles of Economics. Q. J. Econ. 1891, 3, 319–338. [Google Scholar]
- Zhang, X.; Gong, S.H. The Influence of Public Finance Expenditure Structure on Health Resources Allocation Efficiency. Lingnan J. 2014, 5, 101–106. [Google Scholar]
- Parent, O.; Lesage, P.J. Using the Variance Structure of the Conditional Autoregressive Spatial Specification to Model Knowledge Spillovers. J. Appl. Econ. 2008, 23, 235–256. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Primal Indicator | Secondary Indicators | Weights |
|---|---|---|
| Concentration of Healthcare Resources | Number of Hospitals | 0.126 |
| Number of Community Health Service Centers/Stations | 0.175 | |
| Number of Certified Physician Assistants | 0.083 | |
| Number of Certified Physicians | 0.081 | |
| Number of Registered Nurses | 0.079 | |
| Number of Managers in Medical Institutions | 0.076 | |
| Number of Workers in Medical Institutions | 0.085 | |
| Number of Healthcare Practitioners/1000 People | 0.085 | |
| Total Assets of Health Institutions (RMB 1000) | 0.093 | |
| Number of Hospital Beds/1000 People | 0.118 |
| Variables | Unit | Indicator | Observations | Mean | Max | Min | SD |
|---|---|---|---|---|---|---|---|
| Concentration of HCRs | / | / | 434 | 0.309 | 0.752 | 0.01 | 0.171 |
| Economic Development (GDP) | RMB 1 Billion | Regional GDP | 434 | 1562.597 | 8970.523 | 22.034 | 1517.425 |
| Population Size (Pop) | Million | Year-end population | 434 | 43.0715 | 111.6900 | 2.7635 | 27.2375 |
| Urbanization Level (Urb) | % | % of urban land to total land area | 434 | 51.55 | 89.60 | 20.85 | 14.82 |
| Education (Stu) | Number | Number of students in colleges and universities in the region | 434 | 525,563.11 | 2,015,345.00 | 55.00 | 478,440.99 |
| Annual Salary (Wag) | RMB | Average annual salary in the healthcare industry | 434 | 36,225.85 | 183,362.23 | 3648.97 | 20,969.68 |
| Fiscal Expenditure on Healthcare (Exp) | RMB 1 Billion | Fiscal expenditure on health care | 434 | 20.177 | 130.756 | 0.435 | 19.698 |
| Data Range Region | China | Eastern China | Central China | Western China | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2004 | 2010 | 2017 | 2004 | 2010 | 2017 | 2004 | 2010 | 2017 | 2004 | 2010 | 2017 | |
| >0.4 | 35.5 | 29.0 | 25.8 | 25.8 | 22.6 | 19.4 | 6.5 | 3.2 | 3.2 | 3.2 | 3.2 | 3.2 |
| 0.2–0.4 | 41.9 | 45.2 | 48.4 | 6.5 | 9.7 | 9.7 | 19.4 | 19.4 | 22.6 | 16.1 | 16.1 | 16.1 |
| <0.2 | 22.6 | 25.8 | 25.8 | 3.2 | 3.2 | 6.5 | 0 | 3.2 | 0 | 19.4 | 19.4 | 19.4 |
| Objectives | Methods | Results | p-value |
|---|---|---|---|
| Form of Spatial Dependence (lag, error, or both) | LM test no spatial lag | 11.5026 *** | 0.001 |
| Robust LM test no spatial lag | 29.2864 *** | 0.000 | |
| LM test no spatial error | 186.0900 *** | 0.000 | |
| Robust LM test no spatial error | 1.3849 | 0.680 | |
| Selection of Spatial Econometric Model (SAR, SEM, and SDM) | Wald spatial lag | 203.8738 *** | 0.000 |
| LR spatial lag | 136.0359 *** | 0.000 | |
| Wald spatial error | 220.1195 *** | 0.000 | |
| LR spatial error | 354.2586 *** | 0.000 |
| Statistics | Random Effect | Spatial Fixed Effect | Temporal Fixed Effect | Spatiotemporal Fixed Effects |
|---|---|---|---|---|
| R2 | 0.6806 | 0.7574 | 0.7535 | 0.8512 |
| Log-likelihood | 437.6806 | 471.3144 | 487.4108 | 520.7912 |
| Observation | 434 | 434 | 434 | 434 |
| Variable | China | Eastern China | Central China | Western China | |
|---|---|---|---|---|---|
| Direct Effect | GDP | 0.000002 *** (4.339) | 0.000003 ** (2.427) | 0.000007 ** (2.047) | 0.000007 *** (5.777) |
| Pop | 0.000037 *** (11.220) | 0.000027 *** (3.417) | 0.000034 ** (2.411) | 0.000034 *** (8.809) | |
| Urb | 0.004388 *** (9.049) | 0.001679 * (1.669) | 0.009106 ** (2.296) | 0.001228 *** (2.695) | |
| Stu | 0.000000 * (1.881) | 0.000000 * (1.910) | 0.000000 * (1.678) | 0.000000 (1.604) | |
| Wag | 0.000002 *** (3.488) | 0.000007 *** (4.401) | 0.000003 (0.732) | 0.000001 ** (2.082) | |
| Exp | 0.000000 *** (3.606) | 0.000000 *** (3.865) | −0.000000 (−0.392) | 0.000000 (0.222) | |
| Indirect Effect | GDP | −0.000002 ** (−2.152) | −0.000004 *** (−2.730) | −0.000009 *** (−2.601) | −0.000011 *** (−6.824) |
| Pop | −0.000012 ** (−2.156) | 0.000015 (1.473) | 0.000001 (0.039) | −0.000020 *** (3.607) | |
| Urb | 0.000152 (0.203) | 0.002032 * (1.673) | −0.005185 (−1.303) | 0.003092 *** (4.878) | |
| Stu | −0.000000 (−1.103) | 0.000000 (0.191) | 0.000000 (0.435) | −0.000000 (−0.318) | |
| Wag | −0.000004 *** (−3.640) | −0.000008 *** (3.880) | 0.000003 (0.696) | −0.000002 *** (−2.754) | |
| Exp | −0.000000 ** (−2.486) | −0.000000*** (−2.730) | 0.000000 (0.183) | 0.000000 (0.068) | |
| Overall Effect | GDP | 0.000001 (0.855) | −0.000001 (−0.927) | −0.000002** (−2.027) | −0.000004 *** (−3.354) |
| Pop | 0.000025 *** (5.035) | 0.000043 *** (6.075) | 0.000035 *** (8.568) | 0.000014 *** (3.142) | |
| Urb | 0.004540 *** (8.999) | 0.003711 *** (5.464) | 0.003921 *** (7.468) | 0.004320*** (9.868) | |
| Stu | 0.000000 (0.577) | 0.000000* (1.945) | 0.000000 * (1.860) | −0.000000 (−0.895) | |
| Wag | −0.000001 * (1.949) | −0.000001(−0.669) | 0.000000 (0.040) | −0.000001 * (−1.747) | |
| Exp | −0.000000 (−0.319) | 0.000000 (0.237) | −0.000000 (−0.586) | 0.000000 (0.279) | |
| Variables | China | Eastern China | Central China | Western China | |
|---|---|---|---|---|---|
| Direct Effect | GDP | 0.000002 *** (4.554) | 0.000002 * (1.900) | 0.000006 ** (2.349) | 0.000006 *** (6.743) |
| Pop | 0.000032 *** (14.189) | 0.000022 *** (3.978) | 0.000029 ** (2.500) | 0.000030 *** (8.023) | |
| Urb | 0.003965 *** (10.057) | 0.001408 * (1.805) | 0.006763 ** (2.348) | 0.002035 *** (2.709) | |
| Stu | 0.000000 * (1.775) | 0.000000 * (1.952) | 0.000000 (1.605) | 0.000000 (1.357) | |
| Wag | 0.000002 *** (4.987) | 0.000006 *** (5.237) | 0.000003 (0.895) | 0.000001 ** (2.226) | |
| Exp | 0.000000 *** (3.025) | 0.000000 *** (4.345) | −0.000000 (−0.674) | 0.000000 (0.451) | |
| Indirect Effect | GDP | −0.000002 ** (−2.235) | −0.000003 *** (−3.793) | −0.000007 *** (−2.987) | −0.000009 *** (−9.856) |
| Pop | −0.000010 ** (−2.038) | 0.000012 (1.008) | 0.000001 (0.821) | −0.000017 *** (−3.998) | |
| Urb | 0.000137 (0.508) | 0.001907 (1.409) | −0.004925 (−1.465) | 0.002645 *** (5.458) | |
| Stu | −0.000000 (−0.934) | 0.000000 (0.803) | 0.000000 (0.653) | −0.000000 (−0.985) | |
| Wag | −0.000005 *** (−4.578) | −0.000007*** (−4.936) | 0.000003 (0.803) | −0.000002 *** (−3.783) | |
| Exp | −0.000000 ** (−2.079) | −0.000000 *** (−3.785) | 0.000000 (0.907) | 0.000000 (0.708) | |
| Overall Effect | GDP | 0.000001 (0.923) | −0.000000 (−1.005) | −0.000001 ** (−2.154) | −0.000003 *** (−3.674) |
| Pop | 0.000023 *** (5.872) | 0.000037 *** (9.008) | 0.000029 *** (9.654) | 0.000010 *** (2.985) | |
| Urb | 0.003908 *** (9.356) | 0.002901 *** (6.459) | 0.004528 *** (8.485) | 0.003958 *** (7.592) | |
| Stu | 0.000000 (0.782) | 0.000000 * (1.788) | 0.000000 * (1.900) | −0.000000 (−0.706) | |
| Wag | −0.000001 * (−1.687) | −0.000001 (−0.892) | 0.000000 (0.140) | −0.000001 * (−1.876) | |
| Exp | −0.000000 (−0.875) | 0.000000 (0.450) | −0.000000 (−0.765) | 0.000000 (0.682) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Q.; Luo, K. Concentration of Healthcare Resources in China: The Spatial–Temporal Evolution and Its Spatial Drivers. Int. J. Environ. Res. Public Health 2019, 16, 4606. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234606
Guo Q, Luo K. Concentration of Healthcare Resources in China: The Spatial–Temporal Evolution and Its Spatial Drivers. International Journal of Environmental Research and Public Health. 2019; 16(23):4606. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234606
Chicago/Turabian StyleGuo, Qingbin, and Kang Luo. 2019. "Concentration of Healthcare Resources in China: The Spatial–Temporal Evolution and Its Spatial Drivers" International Journal of Environmental Research and Public Health 16, no. 23: 4606. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234606