Prevalence and Predictors of Smoking among Gambian Men: A Cross-Sectional National WHO STEP Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Dependent/Outcome Variables
- “Do you currently smoke any tobacco products, such as cigarettes, cigars or pipes? (responses: Yes; No)”
- “In the past, did you ever smoke daily? (responses: Yes; No)”
2.3. Independent Covariates/Predictor Variables
2.4. Statistical Analysis
3. Results
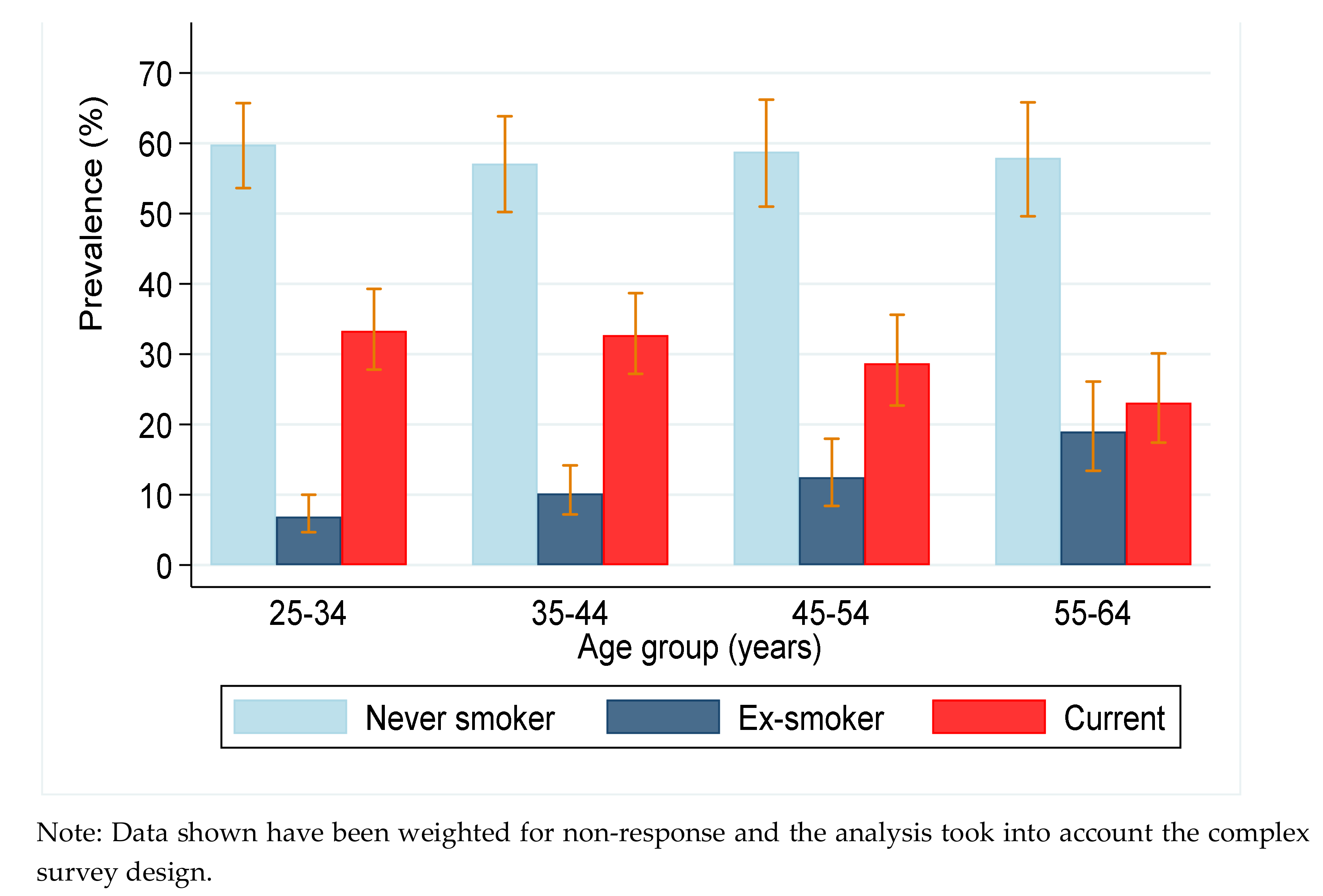
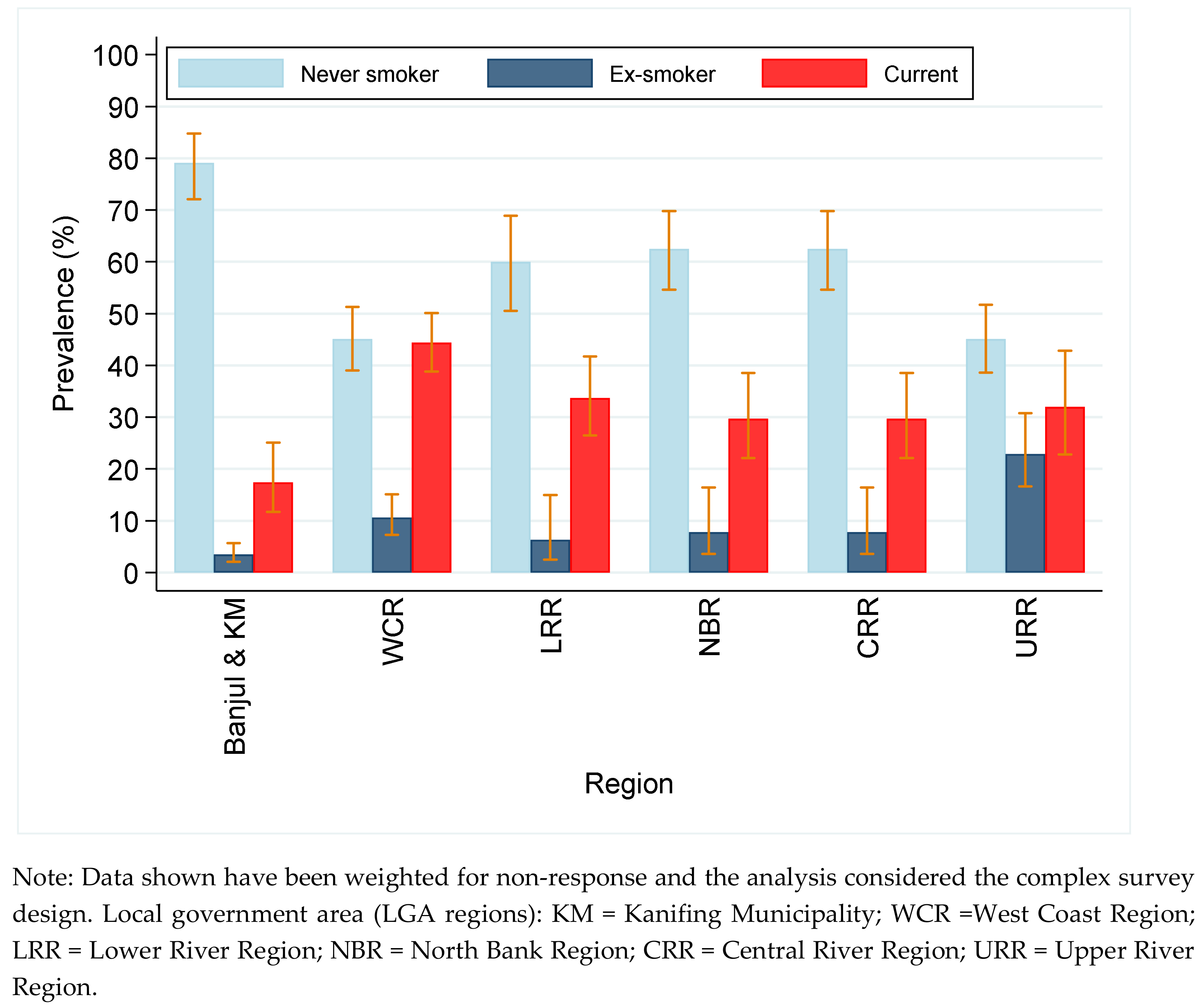
3.1. Prevalence of Smoking among Men
3.2. Multivariate Regression Analysis of Factors Associated with Current and Ex-Smoking
4. Discussion
4.1. Policy Recommendations
4.2. Strengths and Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bilano, V.; Gilmour, S.; Moffiet, T.; d’Espaignet, E.T.; Stevens, G.A.; Commar, A.; Tuyl, F.; Hudson, I.; Shibuya, K. Global trends and projections for tobacco use, 1990–2025: An analysis of smoking indicators from the WHO Comprehensive Information Systems for Tobacco Control. Lancet 2015, 385, 966–976. [Google Scholar] [CrossRef]
- Chandora, R.; Song, Y.; Chaussard, M.; Palipudi, K.M.; Lee, K.A.; Ramanandraibe, N.; Asma, S. Youth access to cigarettes in six sub-Saharan African countries. Prev. Med. 2016, 91, S23–S27. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Report on the Global Tobacco Epidemic, 2013: Enforcing Bans on Tobacco Advertising, Promotion and Sponsorship; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Hiscock, R.; Bauld, L.; Amos, A.; Fidler, J.A.; Munafo, M. Socioeconomic status and smoking: A review. Ann. N. Y. Acad. Sci. 2012, 1248, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Belvin, C.; Britton, J.; Holmes, J.; Langley, T. Parental smoking and child poverty in the UK: An analysis of national survey data. BMC Public Health 2015, 15, 507. [Google Scholar] [CrossRef] [PubMed]
- Xin, Y.; Qian, J.; Xu, L.; Tang, S.; Gao, J.; Critchley, J.A. The impact of smoking and quitting on household expenditure patterns and medical care costs in China. Tob. Control 2009, 18, 150–155. [Google Scholar] [CrossRef]
- Wang, H.; Sindelar, J.L.; Busch, S.H. The impact of tobacco expenditure on household consumption patterns in rural China. Soc. Sci. Med. 2006, 62, 1414–1426. [Google Scholar] [CrossRef]
- John, R.M.; Sung, H.Y.; Max, W.B.; Ross, H. Counting 15 million more poor in India, thanks to tobacco. Tob. Control 2011, 20, 349–352. [Google Scholar] [CrossRef]
- John, R.M.; Mamudu, H.M.; Liber, A.C. Socioeconomic implications of tobacco use in Ghana. Nicotine Tob. Res. 2012, 14, 1205–1212. [Google Scholar] [CrossRef]
- Haustein, K.O. Smoking and poverty. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 312–318. [Google Scholar] [CrossRef]
- WHO. Tobacco and Poverty: A Vicious Circle; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- The United Nations. Sustainable Development Goals; The United Nations: New York, NY, USA, 2015. [Google Scholar]
- Jallow, I.K.; Britton, J.; Langley, T. Prevalence and determinants of tobacco use among young people in The Gambia. BMJ Glob. Health 2017, 2, e000482. [Google Scholar] [CrossRef]
- Manneh, E. A Global Youth Tobacco Survey (GYTS) Country Report 2008; Government of The Gambia: Banjul, The Gambia, 2008.
- Gambia Bureau of Statistics. The Gambia 2018 Multiple Indicator Cluster SurveySurvey Findings Report; Gambia Bureau of Statistics: Banjul, The Gambia, 2019.
- World Health Organization—Noncommunicable Diseases (NCD) Country Profiles. 2018. Available online: https://www.who.int/nmh/publications/ncd-profiles-2018/en/ (accessed on 25 July 2019).
- Jallow, I.K.; Britton, J.; Langley, T. Exploration of policy makers’ views on the implementation of the Framework Convention on Tobacco Control in The Gambia: A qualitative study. Nicotine Tob. Res. 2019, 21, 1652–1659. [Google Scholar] [CrossRef] [PubMed]
- Chisha, Z.; Janneh, M.L.; Ross, H. Consumption of legal and illegal cigarettes in the Gambia. Tob. Control 2019. [Google Scholar] [CrossRef] [PubMed]
- Walraven, G.E.; Nyan, O.A.; Van Der Sande, M.A.; Banya, W.A.; Ceesay, S.M.; Milligan, P.J.; McAdam, K.P. Asthma, smoking and chronic cough in rural and urban adult communities in The Gambia. Clin Exp Allergy 2001, 31, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- WHO. STEPS: A framework for surveillance. In The WHO STEPwise Approach to Surveillance of Non-Communicable Diseases (STEPS); World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Cham, B.; Scholes, S.; Ng Fat, L.; Badjie, O.; Mindell, J.S. Burden of hypertension in The Gambia: Evidence from a national World Health Organization (WHO) STEP survey. Int. J. Epidemiol. 2018, 47, 860–871. [Google Scholar] [CrossRef]
- WHO. Ten years of the WHO STEPwise approach to chronic disease risk factor surveillance (STEPS): Challenges and opportunities (WHO Consultation). In Review of International Experience in NCD Prevention & Control; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Armstrong, T.; Bonita, R. Capacity building for an integrated noncommunicable disease risk factor surveillance system in developing countries. Ethn. Dis. 2003, 13 (Suppl. 2), S13–S18. [Google Scholar]
- Riley, L.; Guthold, R.; Cowan, M.; Savin, S.; Bhatti, L.; Armstrong, T.; Bonita, R. The World Health Organization STEPwise approach to noncommunicable disease risk-factor surveillance: Methods, challenges, and opportunities. Am. J. Public Health 2016, 106, 74–78. [Google Scholar] [CrossRef]
- WHO. WHO STEPS surveillance manual. In The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Gambia Bureau of Statistics. The Gambia 2013 Population and Housing Census Preliminary Results; Gambia Bureau of Statistics: Serrekunda, The Gambia, 2013.
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- Joint WHO/FAO Expert Consultation. Diet, Nutrition and the Prevention of Chronic Diseases; WHO Technical Report Series, No. 916; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Lichtenstein, A.H.; Appel, L.J.; Brands, M.; Carnethon, M.; Daniels, S.; Franch, H.A.; Karanja, N.; Franklin, B.; Harris, W.S.; Lefevre, M.; et al. Diet and lifestyle recommendations revision 2006: A scientific statement from the American Heart Association Nutrition Committee. Circulation 2006, 114, 82–96. [Google Scholar] [CrossRef]
- WHO. Global Physical Activity Questionnaire (GPAQ) Analysis Guide; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Siziya, S.; Babaniyi, O.; Songolo, P.; Nsakashalo-Senkwe, M. Prevalence and correlates for tobacco smoking among persons aged 25 years or older in Lusaka urban district, Zambia. J. Public Health Epidemiol. 2011, 3, 43–48. [Google Scholar]
- Zyaambo, C.; Babaniyi, O.; Songolo, P.; Muula, A.S.; Rudatsikira, E.; Siziya, S. Prevalence and predictors of smoking in a mining town in Kitwe, Zambia: A 2011 population-based survey. Health 2013, 5, 1021–1025. [Google Scholar] [CrossRef]
- Olusegun Babaniyi, M.B.B.S.; Muula, A.S.; Emmanuel Rudatsikira, M.D. Prevalence and correlates for smoking among persons aged 25 years or older in two rural districts of Zambia. Int. J. Child. Health Hum. Dev. 2014, 7, 187. [Google Scholar]
- Houehanou, Y.C.; Lacroix, P.; Mizehoun, G.C.; Preux, P.M.; Marin, B.; Houinato, D.S. Magnitude of cardiovascular risk factors in rural and urban areas in Benin: Findings from a nationwide STEPS survey. PLoS ONE 2015, 10, e0126441. [Google Scholar] [CrossRef]
- Maimela, E.; Alberts, M.; Modjadji, S.E.; Choma, S.S.; Dikotope, S.A.; Ntuli, T.S.; Van Geertruyden, J.P. The Prevalence and Determinants of Chronic Non-Communicable Disease Risk Factors amongst Adults in the Dikgale Health Demographic and Surveillance System (HDSS) Site, Limpopo Province of South Africa. PLoS ONE 2016, 11, e0147926. [Google Scholar] [CrossRef]
- Coa, K.I.; Augustson, E.; Kaufman, A. The Impact of Weight and Weight-Related Perceptions on Smoking Status Among Young Adults in a Text-Messaging Cessation Program. Nicotine Tob. Res. 2018, 20, 614–619. [Google Scholar] [CrossRef]
- Jain, P.; Danaei, G.; Manson, J.E.; Robins, J.M.; Hernan, M.A. Weight gain after smoking cessation and lifestyle strategies to reduce it. Epidemiology 2019. [Google Scholar] [CrossRef]
- The Government of The Gambia. The Gambia Prohibation of smoking (Public Places) Act; The Government of The Gambia: Banjul, The Gambia, 1998.
- Tobacco Conrol Laws: Legislation by Country. Available online: https://www.tobaccocontrollaws.org/legislation/country/gambia/summary (accessed on 16 December 2018).
- The Government of The Gambia. Tobacco Control Regulations 2019; The Government of The Gambia: Banjul, The Gambia, 2019.
- WHO. Framework Convention on Tobacco Control; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Nargis, N.; Manneh, Y.; Krubally, B.; Jobe, B.; Ouma, A.E.; Tcha-Kondor, N.; Blecher, E.H. How effective has tobacco tax increase been in the Gambia? A case study of tobacco control. BMJ Open 2016, 6, e010413. [Google Scholar] [CrossRef]
- The Government of The Gambia. The Tobacco Control Act 2016; The Government of The Gambia: Banjul, Gambia, 2016.
- DeBry, S.C.; Tiffany, S.T. Tobacco-Induced neurotoxicity of adolescent cognitive development (TINACD): A proposed model for the development of impulsivity in nicotine dependence. Nicotine Tob. Res. 2008, 10, 11–25. [Google Scholar] [CrossRef]
- Stead, L.F.; Lancaster, T. Interventions for preventing tobacco sales to minors. Cochrane Database Syst. Rev. 2005. [Google Scholar] [CrossRef]
- Asare, S.; Stoklosa, M.; Drope, J.; Larsen, A. Effects of Prices on Youth Cigarette Smoking and Tobacco Use Initiation in Ghana and Nigeria. Int. J. Environ. Res. Public Health 2019, 16, 3114. [Google Scholar] [CrossRef]
- Brinn, M.P.; Carson, K.V.; Esterman, A.J.; Chang, A.B.; Smith, B.J. Mass media interventions for preventing smoking in young people. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Wakefield, M.; Flay, B.; Nichter, M.; Giovino, G. Effects of anti-smoking advertising on youth smoking: A review. J. Health Commun. 2003, 8, 229–247. [Google Scholar] [CrossRef]
- Henriksen, L.; Dauphinee, A.L.; Wang, Y.; Fortmann, S.P. Industry sponsored anti-smoking ads and adolescent reactance: Test of a boomerang effect. Tob. Control 2006, 15, 13–18. [Google Scholar] [CrossRef]
- Bates, C.; Watkins, P.; McNeill, A. Danger: PR in the Playground: Tobacco Industry Initiatives on Youth Smoking. Action on Smoking and Health: London, UK, 2000. [Google Scholar]
- Lee, K.A.; Palipudi, K.M.; English, L.M.; Ramanandraibe, N.; Asma, S. Secondhand smoke exposure and susceptibility to initiating cigarette smoking among never-smoking students in selected African countries: Findings from the Global Youth Tobacco Survey. Prev. Med. 2016, 91, S2–S8. [Google Scholar] [CrossRef]
- Albers, A.B.; Biener, L.; Siegel, M.; Cheng, D.M.; Rigotti, N. Household smoking bans and adolescent antismoking attitudes and smoking initiation: Findings from a longitudinal study of a Massachusetts youth cohort. Am. J. Public Health 2008, 98, 1886–1893. [Google Scholar] [CrossRef]
- Hald, J.; Overgaard, J.; Grau, C. Evaluation of objective measures of smoking status—A prospective clinical study in a group of head and neck cancer patients treated with radiotherapy. Acta Oncol. 2003, 42, 154–159. [Google Scholar] [CrossRef] [Green Version]
- Brathwaite, R.; Addo, J.; Smeeth, L.; Lock, K. A Systematic Review of Tobacco Smoking Prevalence and Description of Tobacco Control Strategies in Sub-Saharan African Countries; 2007 to 2014. PLoS ONE 2015, 10, e0132401. [Google Scholar] [CrossRef]
- Addo, J.; Smeeth, L.; Leon, D.A. Smoking patterns in Ghanaian civil servants: Changes over three decades. Int. J. Environ. Res. Public Health 2009, 6, 200–208. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Model I (Age Adjusted) | Model II (Fully Adjusted) | |||
|---|---|---|---|---|
| Ex-Smoker | Current-Smoker | Ex-Smoker | Current-Smoker | |
| Variable | a RRR(95% CI) | a RRR(95% CI) | ARRR (95% CI) | ARRR (95% CI) |
| Age Group | ||||
| 25–34 | Reference | Reference | Reference | Reference |
| 35–44 | 1.55(0.94–2.55) | 1.03(0.77–1.38) | 2.26(1.18–4.35) * | 1.11(0.81–1.52) |
| 45–54 | 1.84(1.11–3.05) * | 0.88(0.60–1.28) | 2.12(1.15–3.93) * | 0.93(0.62–1.39) |
| 55–64 | 2.84(1.69–4.78) *** | 0.72(0.46–1.12) | 3.76(1.79–7.87) *** | 0.78(0.50–1.21) |
| Ethnicity | ||||
| Mandinka | Reference | Reference | Reference | Reference |
| Wollof | 1.15(0.55–2.40) | 0.62(0.39–1.02) | 1.04(0.41–2.63) | 0.65(0.38–1.11) |
| Fula | 1.06(0.64–1.76) | 1.26(0.84–1.90) | 0.80(0.44–1.43) | 1.14(0.73–1.76) |
| Jola | 0.45(0.14–1.42) | 1.13(0.76–1.70) | 0.62(0.24–1.61) | 1.07(0.68–1.68) |
| Others | 0.57(0.25–1.29) | 0.71(0.45–1.12) | 0.63(0.36–1.12) | |
| Education | ||||
| ≤ 6 Years | Reference | Reference | Reference | Reference |
| 7–12 Years | 0.78(0.47–1.30) | 0.74(0.50–1.09) | 1.00(0.50–1.90) | 0.81(0.53–1.23) |
| > 12 Years | 0.51(0.21–1.22) | 0.72(0.49–1.07) | 0.61(0.25–1.51) | 0.97(0.66–1.42) |
| Residence (Rurality) | ||||
| Urban | Reference | Reference | Reference | Reference |
| Semi urban | 2.77(1.57–4.88) *** | 1.28(0.76–2.15) | 1.27(0.63–2.59) | 0.91(0.53–1.56) |
| Rural | 2.18(1.18–4.03) ** | 1.56(1.05–2.33) * | 0.84(0.38–1.87) | 0.92(0.62–1.37) |
| Servings of fruits & vegs | ||||
| ≥ 5/day | Reference | Reference | Reference | Reference |
| < 5/day | 1.11(0.55–2.26) | 1.13(0.78–1.67) | 0.99(0.47–2.04) | 1.14(0.78–1.68) |
| Physical activity | ||||
| ≥ 600METS/week | Reference | Reference | Reference | Reference |
| < 600METS/week | 0.26(0.14–0.47) *** | 0.26(0.13–0.51) *** | 0.42(0.17–1.07) | 0.77(0.42–1.43) |
| BMI c | ||||
| Normal weight | Reference | Reference | Reference | Reference |
| Underweight | 1.71(0.97–3.02) | 1.71(1.18–2.48) *** | 2.00(1.17–3.42) ** | 1.41(0.91–2.17) |
| Overweight | 0.81(0.47–1.40) | 0.53(0.38–0.74) ** | 0.60(0.30–1.17) | 0.53(0.36–0.77) *** |
| Obese | 0.58(0.26–1.32) | 0.52(0.32–0.84) ** | 0.41(0.14–1.19) | 0.64(0.35–1.17) |
| Waist circumference d | ||||
| Normal | Reference | Reference | Reference | Reference |
| High | 1.44(0.92–2.27) | 0.74(0.42–1.26) | 1.96(1.26–3.04) ** | 0.73(0.42–1.28) |
| Hypertension e | ||||
| No (normotensive) | Reference | Reference | Reference | Reference |
| Yes (diagnosed) | 3.99(1.94–8.20) *** | 1.02(0.49–2.11) | 2.64(1.12–6.23) *** | 1.14(0.523–2.47) |
| Yes (undiagnosed) | 1.61(0.86–3.02) | 1.06(0.76–1.48) | 1.76(0.88–3.51) | 1.10(0.44–1.50) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cham, B.; Scholes, S.; Groce, N.E.; Mindell, J.S. Prevalence and Predictors of Smoking among Gambian Men: A Cross-Sectional National WHO STEP Survey. Int. J. Environ. Res. Public Health 2019, 16, 4719. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234719
Cham B, Scholes S, Groce NE, Mindell JS. Prevalence and Predictors of Smoking among Gambian Men: A Cross-Sectional National WHO STEP Survey. International Journal of Environmental Research and Public Health. 2019; 16(23):4719. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234719
Chicago/Turabian StyleCham, Bai, Shaun Scholes, Nora E. Groce, and Jennifer S. Mindell. 2019. "Prevalence and Predictors of Smoking among Gambian Men: A Cross-Sectional National WHO STEP Survey" International Journal of Environmental Research and Public Health 16, no. 23: 4719. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234719