1. Introduction
An adequately functioning immune system is essential for the body to recognize and defend itself against exposure to external agents, including bacteria, viruses and substances (e.g., alcohol and drugs). Various environmental factors, lifestyle and behaviors can affect immune functioning, both positively and negatively [
1]. Exposure to psychological factors (e.g., stress) can also impact immune functioning. The immune system plays an important role, either positive or negative, in various diseases and disorders and is an important health determinant [
2,
3,
4,
5,
6,
7,
8,
9,
10]. For example, altered immune functioning may have a pronounced effect on normal physiological processes but is also involved in the pathology of various chronic diseases as well as certain psychiatric disorders such as depression and autism [
11,
12]. A combination of neuroinflammatory, neuroendocrine and metabolic effects can result in reduced immune functioning and subsequently have a negative impact on wellbeing and quality of life [
6,
8,
13]. To identify people at risk for disease [
14], assessing how well the immune system functions, i.e., immune fitness, is important to enable early intervention, for example.
There are several ways to evaluate immune functioning. The most frequently used involve objective qualitative and quantitative assessments in blood, e.g., counts of the type and number of immune cells, immune mediators such as cytokines, chemokines and/or antibodies [
14,
15]. Such measures are relative costly, time-consuming and invasive. Even noninvasive assessments in saliva or urine require specialist resources and can be regarded as an imposition on those being assessed. Additionally, there is usually a time delay before results are available.
Perhaps more important, these objective assessments are often not informative about how participants experience their immune fitness, or how they feel (e.g., mood or quality of life). The latter can only be determined by subjective assessments, i.e., asking the patients how they feel. These experiential factors represent the most important determinants for participants to judge if they feel sick or healthy, and consequently seek medical help or advice [
16]. These factors led us to develop a self-assessment instrument of immune fitness. This has ramifications for clinical practice, for example to determine whether further biomarker assessments are warranted.
Such a self-assessment questionnaire has multiple potential applications, since it can be used in clinical practice, for research proposes, as well as by an individual for self-assessment. The outcome of the questionnaire is not only useful to screen for an increased risk of immune-related disease but can also influence one’s decision to seek medical attention or adapt their lifestyle. The development of such a questionnaire is essential, since a growing number of chronic diseases and disorders are linked to alterations in the immune system [
17,
18].
There are several scales developed to assess immune status, including the 1-item perceived immune functioning rating, which is used as a comparator in the studies reported here. The 1-item perceived immune functioning rating has been used in several studies as a measure of current immune fitness and showed to correlate significantly to various health outcomes, including ratings of sleep disturbance, autism, general health, mental resilience and irritable bowel syndrome (IBS) [
16,
19,
20,
21,
22]. The 1-item has the advantage of being simple to administer and is currently the quickest method of determining perceived immune functioning. As a momentary assessment, however, it is by definition limited to the current perception of immune fitness. It also does not provide any information about the possible underlying cause(s) related to the outcome.
The Immune Fitness Questionnaire (IFQ) [
23] served as the basis for developing the Immune Status Questionnaire (ISQ). The IFQ does provide information about the underlying cause as it includes multiple items. A study introducing the IFQ revealed significant associations of IFQ scores with the number of general physician visits, general health and experiencing problematic internet use [
23]. Although it has not been used in clinical practice, our group used the IFQ in two of our studies [
19,
22]. This led to the identification of certain shortcomings. Specifically, the IFQ does not capture some of the common aspects of a compromised immune function, such as muscle and joint pain or the common cold. On the other hand, it does include some relatively less common items, such as meningitis, slow healing wounds and boils.
The immune system assessment questionnaire (ISAQ) was developed as an alternative scale [
24]. The ISAQ is an elaborate questionnaire with high specificity but moderate sensitivity to identify immune dysfunction. Sievers et al. [
18] altered the ISAQ to obtain the infectious disease questionnaire (or “ID screen”). The ID screen is used to investigate infectious diseases and their risk factors, rather than overall immune functioning. Although it has been more extensively validated, it is not a suitable alternative for the ISQ, largely because it specifically targets identification of infectious disease rather than overall immune status. Finally, the Sickness questionnaire (SicknessQ) of Andreasson et al. [
17] was developed to investigate symptoms of immune activation related to sickness behavior. Andreasson reported significant associations between SicknessQ scores and depression, anxiety, self-rated health and a single item of feeling sick. Despite the development of these questionnaires, a literature search did not identify any studies using the IFQ, ISAQ, the ID screen or the SicknessQ in clinical practice. This may be caused by the fact that the scales were elaborate and focusing on specific aspects of immune symptom functioning (e.g., infectious disease risk) rather than providing a global rating of general immune fitness assessed over a relevant period of time (e.g., the past year). Therefore, the aim of the current series of studies was to develop, validate and implement a short and cost-effective immune status questionnaire, with applicability in multiple settings, including clinical practice, research and self-assessment.
2. Materials and Methods
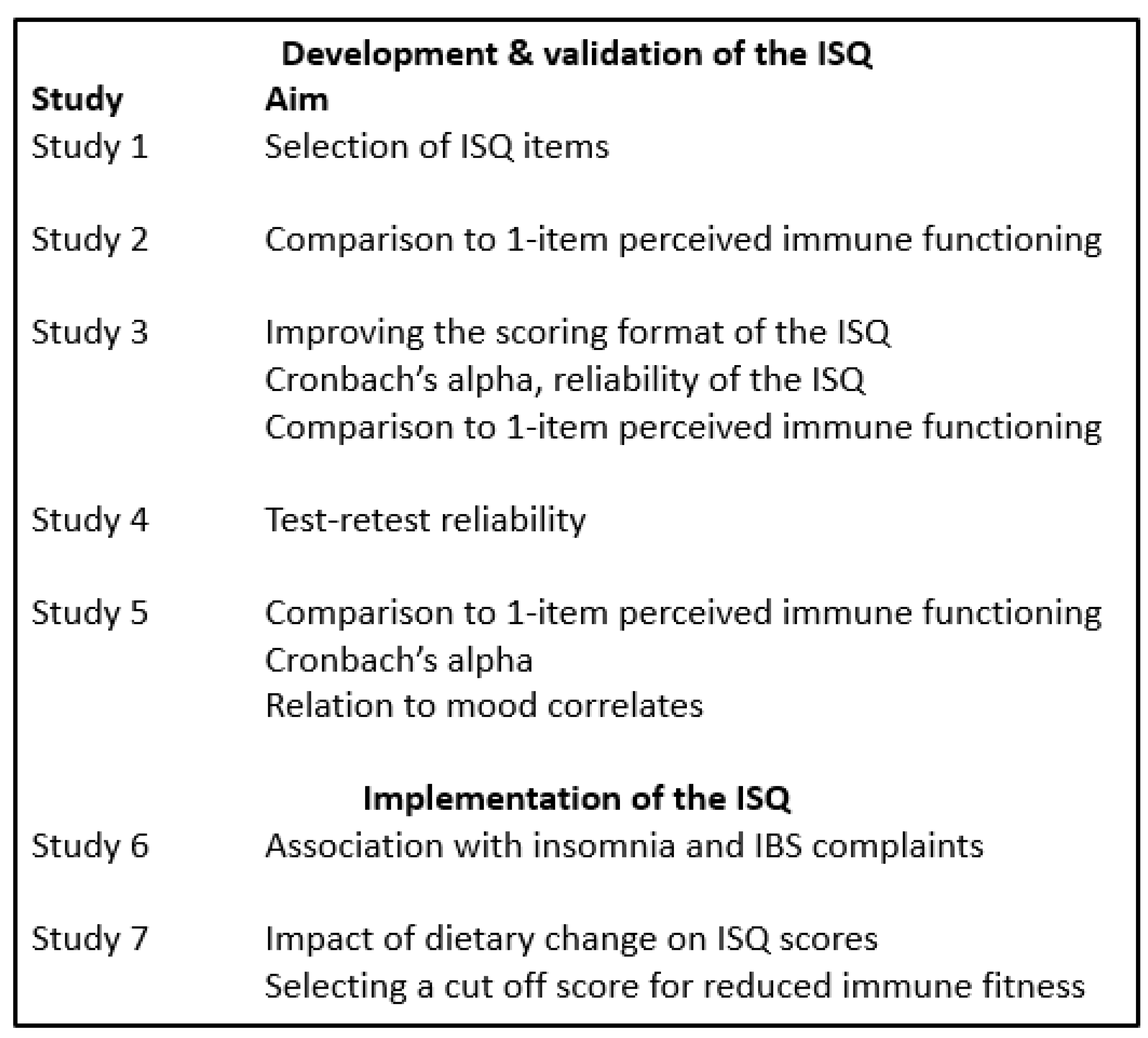
To develop and validate the ISQ, five studies were conducted. The ISQ was implemented in two subsequent studies [
25,
26]. The seven studies (summarized in
Figure 1) are detailed in following sections. The studies were conducted by Utrecht University and the Ethics Committee of the Faculty of Social and Behavioral Sciences of Utrecht University granted ethical approval (approval code FETC17-061).
2.1. Study 1: Development of the ISQ
Study 1 aimed at developing a shortened immune functioning questionnaire compared with the IFQ. Based on discussion of the scientific literature [
1] we added 4 new items to the IFQ, and it was determined which of the 23 items are relevant to predict overall immune fitness. The aim was to develop a shortened questionnaire that includes sufficient questions to have a predictive validity of at least 85% of the adapted 23-item IFQ questionnaire. The participants were Dutch students and young adults, 18 to 30 years old. They were approached via an online advertisement on Facebook, to take the online survey in SurveyMonkey. A total of
n = 258 Dutch adults completed the survey. Their mean (SD) age was 22.9 (3.4) years old. Perceived immune functioning was assessed using the IFQ [
19]. The IFQ items include “sore throat”, “headaches”, “flu”, “runny nose”, “coughing”, “cold sores”, “boils”, “mild fever”, “warts/verrucas”, ““pneumonia”, “bronchitis”, “sinusitis”, “sudden high fever”, “ear infection”, “diarrhea”, “meningitis”, “eye infection”, “sepsis” and “long healing injuries”. The four extra items were “shortness of breath”, “skin problems (e.g. acne & eczema)”, “muscle and joint pain” and “common cold”. Items were scored on a 5-point Likert scale ranging from 1 (“never”) to 5 (“frequently experienced”). The scoring of three items of the original IFQ (flu, pneumonia and meningitis) was changed from a 5-point Likert-scale to a yes/no question. Scoring of the items with a yes/no answer was 0 points for “no”. A “yes” for flu gave 2 points, while a “yes” for meningitis and pneumonia gave 4 points. The sum score of all items yielded an overall IFQ score ranging from 20 to 110, with higher scores indicating a poorer immune status. Participants were also asked to rate their current perceived immune status and perceived general health status, respectively, on a scale from 0 (very poor) to 10 (excellent) [
16]. They further reported whether or not they experienced reduced immune fitness (i.e., a lowered immune functioning level compared to normal) at the moment of participation and whether or not they had a chronic disease (using a “yes”/“no” question format).
2.2. Study 2: Comparison of ISQ with 1-Item Perceived Immune Functioning and General Health
Study 2 investigated the relationship between a 1-item rating of current perceived immune functioning and a 1-item rating of current general health with the shortened immune functioning questionnaire of Study 1. The participants were Dutch students and other young adults, 18 to 30 years old. They were approached via an online advertisement on Facebook, to take the online survey in SurveyMonkey. The shortened IFQ consisted of 7 representative immune associated symptoms and diseases derived from the regression analysis of Study 1 (“sudden high fever”, “diarrhea”, “headache”, “skin problems (e.g. acne & eczema)”, “muscle and joint pain”, “common cold” and “coughing”). These items were scored on a 5-point Likert scale ranging from 1 to 5 (scale ranging from “never” to “frequently experienced”). This yielded an overall immune fitness score ranging from 7 to 35, with higher scores indicating a poorer immune status. Moreover, participants were asked to complete two 1-item questions, in order to rate their perceived immune functioning and perceived general health on a scale from 0 (very poor) to 10 (excellent) [
16]. They further reported whether they experienced a lowered immune functioning at the moment of participation and whether they had a chronic disease.
2.3. Study 3: Modifying ISQ Scoring
Study 3 investigated the effect of modifying the Likert scale for questionnaire responses in order to improve the format of the ISQ. This was based on feedback from participants of Study 1 and 2, who sometimes struggled to differentiate between responding “once or twice” and “occasionally”. Similarly, the difference between “regularly” and “frequently” was unclear to some participants. Therefore, Study 3 investigated the utility of an alternative scoring for the ISQ. Dutch students, 18–30 years old, were approached at the campus of Utrecht University, and invited to complete the survey on paper. The ISQ derived from Study 1 scored items on a 5-point Likert scale ranging from 1 to 5 with never, once or twice, occasionally, regularly and frequently experienced as anchors (overall scoring range 7 to 35, with higher scores representing poorer immune fitness). The alternative ISQ rated the same 7 immune associated symptoms and diseases in the ISQ on a 5-point Likert scale ranging from 0 to 4 with never, sometimes, regularly, often and (almost) always as anchors. Thus, the ISQ scores range from 0 to 28, with higher scores representing a poorer immune status. Again, 1-item perceived immune functioning and general health were assessed and participants indicated whether they experienced a lowered immune functioning at the moment of participation and whether they had a chronic disease.
2.4. Study 4: Test–Retest Reliability of the ISQ
Study 4 investigated the test–retest reliability of the ISQ. Dutch students, 18–30 years old, were approached at the beginning of a lecture at Utrecht University, and invited to complete a short survey on paper, consisting of the ISQ and some demographic questions. Eight or ten days later the same students were approached at the beginning of another lecture and invited to complete the survey again. A total of 53 students completed the two surveys.
2.5. Study 5: Exploration Health Correlates of the ISQ in an International Sample
Study 5 investigated the association of the final ISQ with two 1-item scales of perceived immune functioning, as well as various health aspects in an international young adult sample. A total of 333 young adults (18–30 years old), either at work or on holiday in Fiji, completed the ISQ. The participants originated from various countries around the world. They completed the ISQ as part of a larger study on alcohol consumption, health and immune fitness. Current perceived immune functioning and general health were rated on 1-item scales ranging from 0 (very poor) to 10 (excellent). The past year’s stress, anxiety, depression, anger/hostility, being active and fatigue were assessed on 11-point scales ranging from 0 (absent) to 10 (extreme).
2.6. Study 6: Relationship of ISQ with Irritable Bowel Syndrome (IBS) Complaints in an Insomnia Sample
An online survey was conducted among 487 Dutch adults with insomnia complaints [
25]. As previous research suggested a relationship between reduced immune fitness and having IBS complaints [
22], in this study the ISQ was related to scores on the Birmingham IBS Symptoms Questionnaire [
27]. The scale comprises subscales rating the severity of constipation, pain and diarrhea complaints. In addition, perceived current immune functioning was rated on a 1-item scale ranging from 0 (very poor) to 10 (excellent).
2.7. Study 7: ISQ Scores in Dutch Participants with Poor Versus Normal Health: The Impact of Dietary Change
Study 7 examined the ISQ before and after a dietary change in a Dutch adult sample with “poor health” or “normal health” [
26]. A survey was conducted among Dutch adults to evaluate their health status before and after the start of consuming raw fermented milk (RFM) products [
26]. They were recruited at a Dutch farm where they bought RFM products. The RFM product was labeled with an invitation flyer to complete an online survey. As part of the survey the ISQ was completed. The ISQ was completed retrospectively, assessing the participant’s immune status before and after switching to consuming RFM. In addition, 1-item perceived immune functioning was rated for the same time periods. Participants were allocated to the “poor health” group in case they reported reduced immune resistance or suffered from a chronic disease before the start of consuming RFM products. Other participants were allocated to the “normal health” group. Other variables of interest were sex and living location (rural versus urban).
2.8. Data Analysis
Statistical analysis was performed using SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY, USA: IBM Corp.). For each study, the mean and standard deviation (SD) for each variable was computed. Data were examined for the whole sample, and sex differences were explored as well, using independent t-tests or Chi-squared tests.
For study 1, a stepwise linear regression analysis was conducted to investigate which items significantly impacted the total IFQ score and should be included in the ISQ. The model should predict the IFQ score for at least 85%. For Studies 2 and 3, a Spearman correlation analysis was conducted to investigate the relationship between the ISQ and the 1-item perceived immune functioning and general health scores. In all text and tables throughout the manuscript Spearman’s rho is referred to as “r”. In Study 3, reliability analysis was conducted by computing Cronbach’s alpha, Spearman–Brown split-half, the average inter-item correlation, and the average item-total correlation. In Study 4, data from two different test occasions on which the same sample completed the ISQ were compared using nonparametric independent samples Mann–Whitney U tests, and a Spearman correlation analysis was conducted to investigate test-retest reliability.
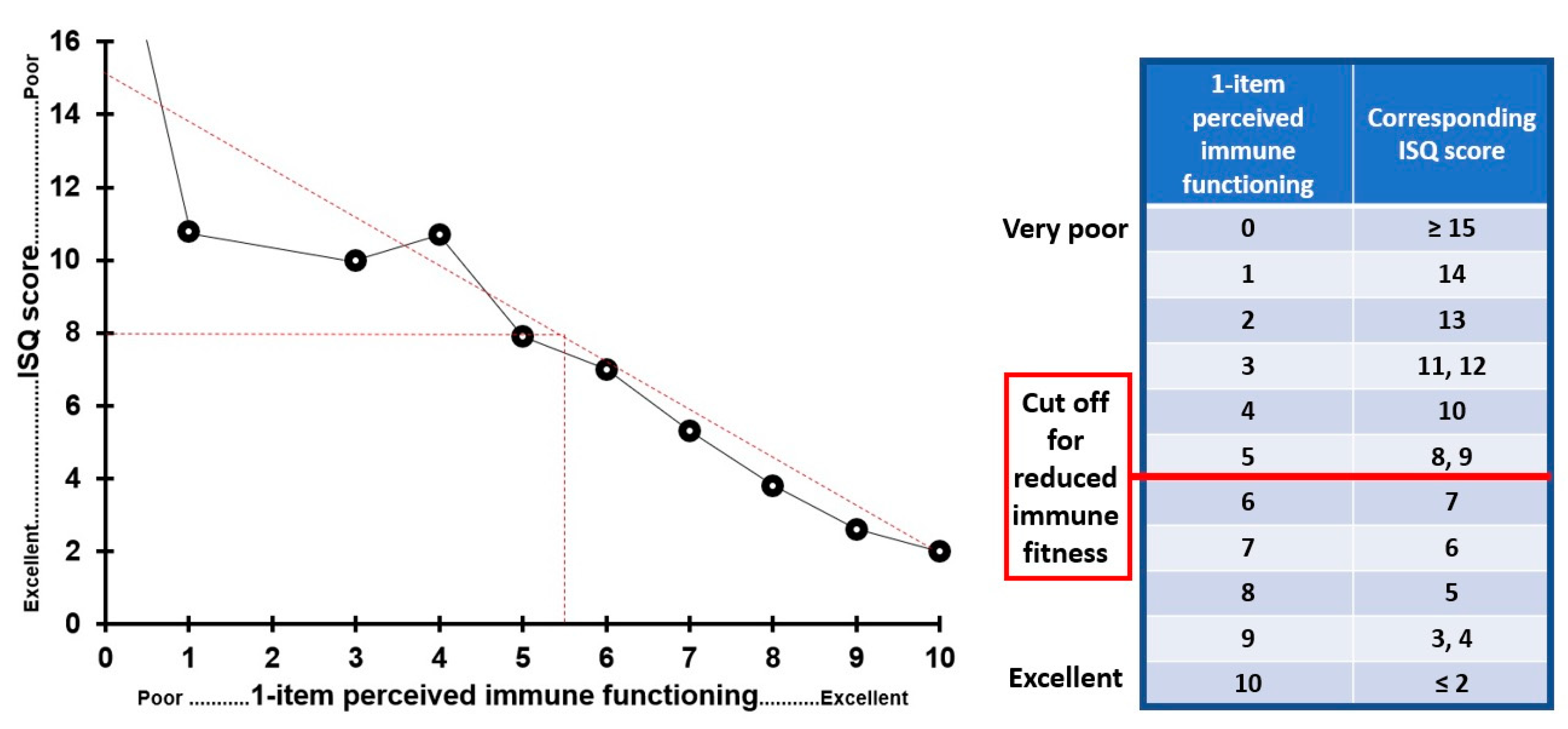
In Study 5, the ISQ was tested in an international sample and scores were correlated (Spearman’s rho) with the assessed health outcomes (e.g., depression and stress). In Study 6, ISQ scores were correlated with IBS outcomes by computing nonparametric Spearman’s rho correlations. Differences between men and women, between those formally diagnosed with insomnia and those with self-reported insomnia complaints, and between those reporting sleep initiation or sleep maintenance problems, or both, were computed using nonparametric independent samples Mann–Whitney U tests. In Study 7, ISQ scores were compared (1) before versus after the dietary change, (2) between men and women, (3) between participants with a “poor” and “normal” health and (4) between rural and urban living location, using nonparametric independent samples Mann–Whitney U tests. Outcomes were considered significant if p < 0.05. In addition, to determine a cut off point for reduced immune functioning, a direct comparison was made via linear data fitting, between ISQ scores and 1-item perceived immune functioning scores. For the 1-item perceived immune functioning scale, reduced immune fitness is assumed if a score below 5.5 is obtained. The corresponding ISQ score is proposed as ISQ cut off point for reduced immune functioning.
4. Discussion
The ISQ is a short and practical scoring form and useful for clinical practice and research requiring a quick screening of a participant’s immune status of the past 12 months. In a series of studies, the ISQ was developed and validated. The final ISQ consists of 7 items rating past year’s immune status, by inquiring about the incidence of specific immune−related complaints. The combined scores on the items correlated significantly, albeit modest, with perceived immune fitness and several psychological corelates, such as stress and depression.
The IFQ [
19] served as the basis for developing the ISQ. Based on scientific literature, several items were added. Subsequently, the new listing was shortened into the ISQ. Significant correlations of ISQ scores were found with the 1−item perceived immune functioning rating and a variety of health outcomes. The strengths of this research include the extensive validation in different studies. The ISQ is particularly useful in situations with time constraints, where the use of extensive questionnaires is not appropriate. The ISQ is also multi−applicable, since it can be used both in the clinic as for the individual as self−assessment in research surveys and screening in clinical trials.
Across studies, even though statistically significant, the magnitude of the observed sex differences in ISQ scores is small around 1 or less on a scale ranging from 0 to 28. Therefore, the observed differences in ISQ scores between men and women do not seem to have great clinical relevance. Whereas Studies 1–5 contained primarily healthy participants, Study 7 had a larger subsample of participants reporting having a chronic disease. ISQ scores (before the dietary change) differed significantly between those with chronic diseases (i.e., “poor health” status) and healthy participants (i.e., “normal health” status).
To have a validated cut−off point at which a certain ISQ score indicates poor immune status and/or warrants further medical investigation would be of great value as it will significantly enhance the applicability of the ISQ in clinical practice. Using the original ISQ data (scoring range 0 to 28, i.e., before applying the final scoring format) suggests that a cut−off point for “poor” immune status should be 8 (see
Figure 7). Indeed, the chronic disease group in Study 7 had an ISQ scores of around 8, whereas the “normal health” groups had a raw ISQ score around 4. These findings are also in line with Study 5, which showed that insomnia patients with IBS complaints had average ISQ scores ranged from 8 to 10, depending on the nature of sleep complaints. With the final scoring format of the ISQ (scoring range 0 to 10), a cut off of an “original” ISQ score of 8 corresponds to a “final” ISQ score of 5. Thus, ISQ scores < 6 are thought to indicate a poor past year’s immune status.
It may be argued that the relatively low internal consistency, as measured with Cronbach’s alpha, is a limitation of the ISQ. However, this observation was expected and does not invalidate the ISQ. It is common that scales with a low number of unique items have a low Cronbach’s alpha [
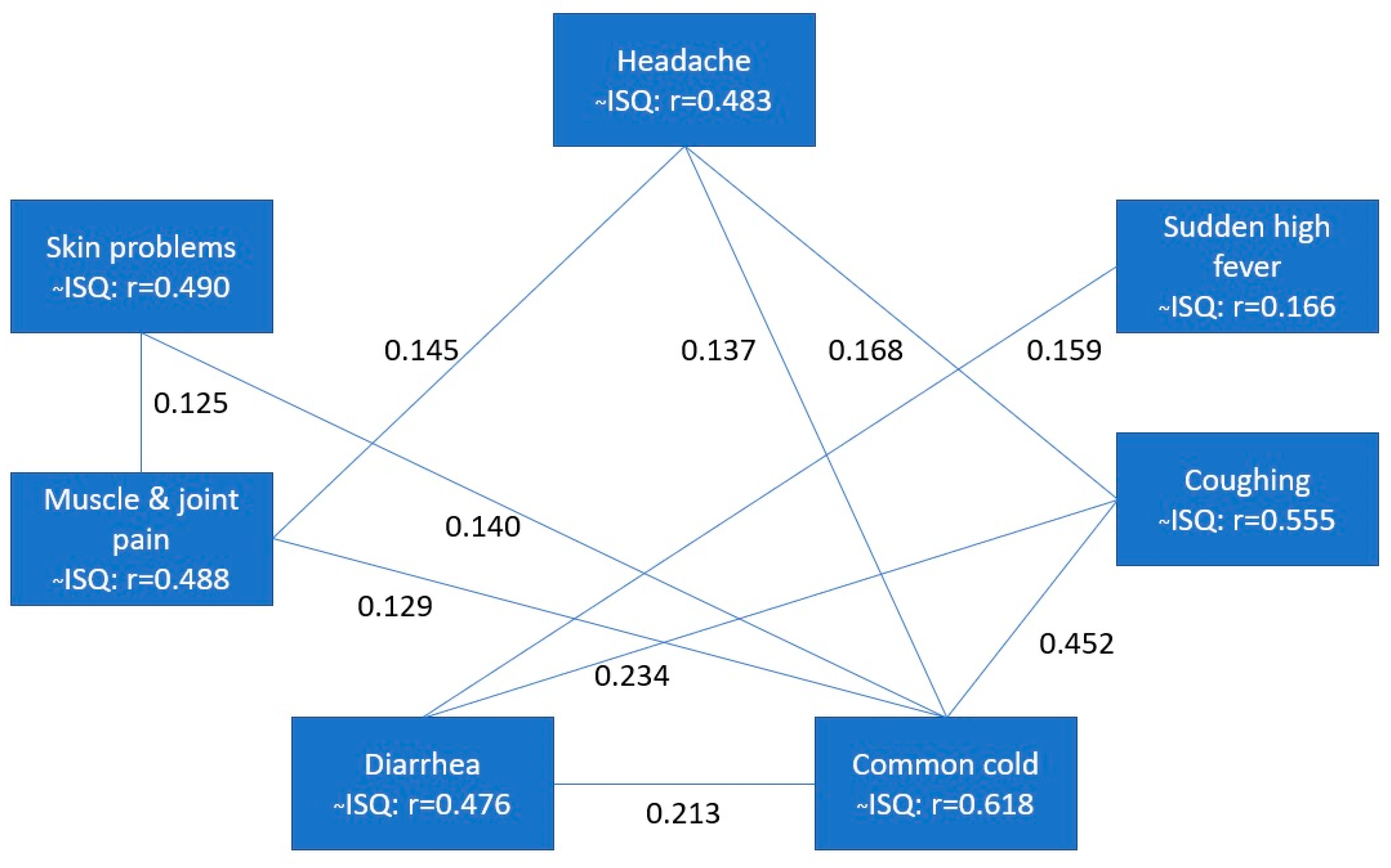
28]. This reflects the fact that immune status is a broad concept that is defined by many factors. The expression of various diseases and health complaints may contribute to it. The 7 items of the ISQ are all unique predictors of the broad concept of immune status, and correlational analysis revealed that their interrelationship is therefore low. Only the items coughing and common cold are stronger related (r = 0.452), but individually can contribute independently from each other. This can be explained by the fact that coughing is associated with a wide assortment of assortment of clinical associations and etiologies including the common cold [
29]. The observed correlations in the current study between mood outcomes and ISQ were low to moderate, while at the same time these mood outcomes are often highly interrelated. This further underlines that immune fitness is a complex concept that can be independently influenced by a large number of immune−related variables.
Finally, additional validation studies should be conducted to improve our understanding of the ISQ, and to determine how the self−rated immune functioning scores relate to objective biomarkers of immune fitness. For example, ISQ scores could be related to biomarkers of immune functioning, such as blood cytokine levels. In this context, previous research has shown significant correlations between self−rated health and immune biomarkers in both patients [
30] and healthy volunteers [
31,
32,
33]. However, another study revealed that perception of immune functioning was unrelated to immune biomarkers, including serum antibodies and blood lymphocytes [
34]. Similar to our studies, the authors did find a strong relationship between perceived immune functioning and (changes in) mood. Together, up to now research investigating the relationship between objective and subjective assessments of immune functioning yielded inconsistent results. Therefore, evaluating the association of ISQ scores in relation to immune biomarkers will be the aim of future research.

 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






