A Retrospective Study about the Differences in Cardiometabolic Risk Indicators and Level of Physical Activity in Bariatric Surgery Patients from Private vs. Public Units

 , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Background
2. Methods
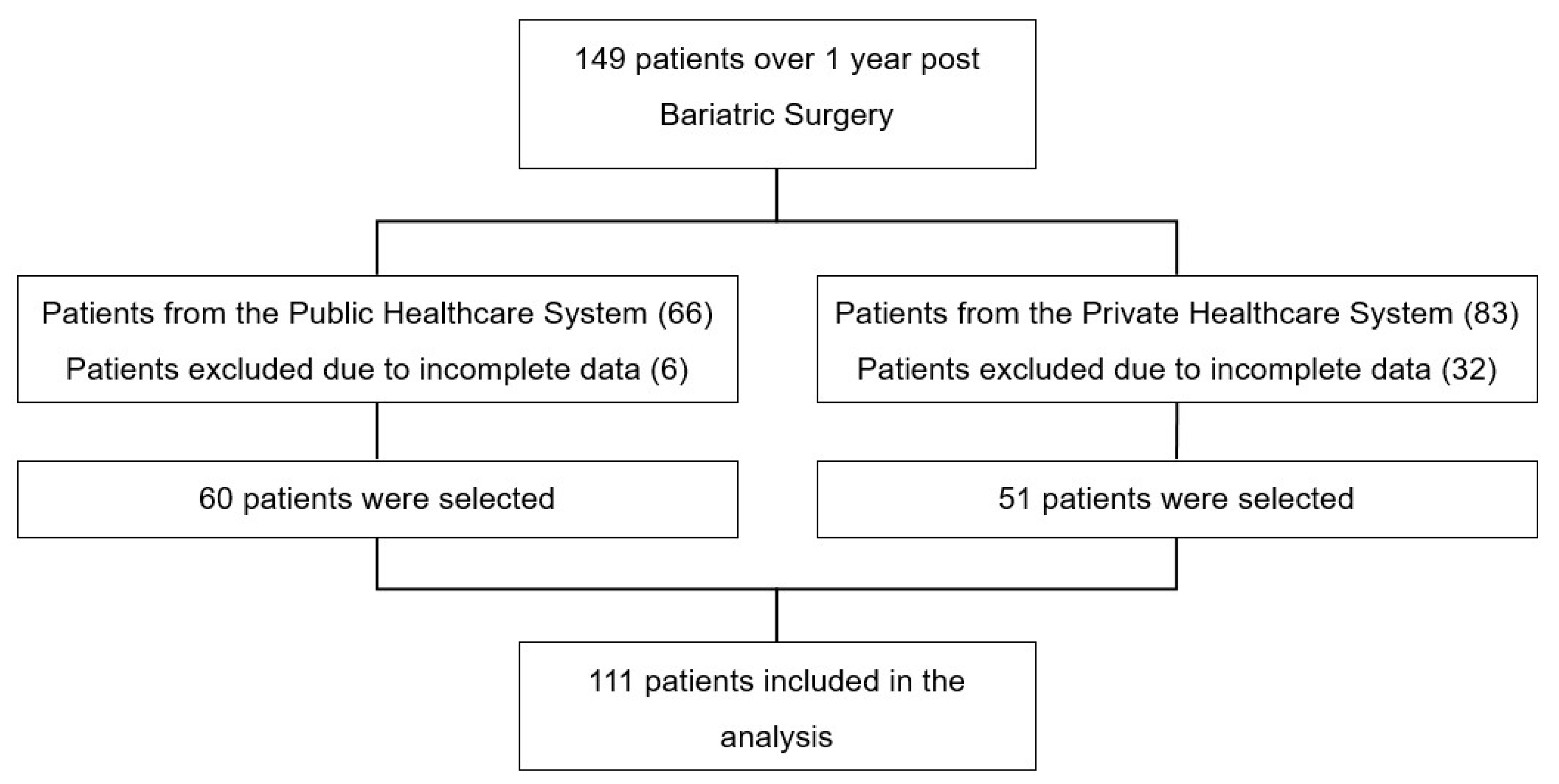
3. Sample
4. Data Collection
4.1. Anthropometrics
4.2. Comorbidities Related to Obesity
4.3. Biochemical Analysis
4.4. International Physical Activity Questionnaire (IPAQ)
4.5. Statistics
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kushner, R.F.; Kahan, S. Introduction The State of Obesity in 2017 Obesity Prevalence Disease Morbidity Models of care. Med. Clin. 2017, 102, 1–11. [Google Scholar]
- Junges, V.M.; Cavalheiro, J.M.; Fam, E.F.; Closs, V.E.; Moraes, J.F.; Gottlieb, M.G. Impact of Roux-en-Y Gastric Bypass Surgery ( RYGB ) on metabolic syndrome components and on the use of associated drugs in obese patients. Arq. De Gastroenterol. 2017, 54, 139–144. [Google Scholar] [CrossRef]
- De Oliveira, M.L.; Maria, L.; Santos, P.; Nunes, E. Direct Healthcare Cost of Obesity in Brazil: An Application of the Cost-of-Illness Method from the Perspective of the Public Health System in 2011. PLoS ONE 2015, 10, e0121160. [Google Scholar] [CrossRef]
- Márcia, S.; Kelles, B.; Machado, C.J.; Barreto, S.M. Original Article Ten-years of bariatric surgery in Brazil: In-hospital mortality rates for patients assisted by universal health system or a health maintenance organization. ABCD Arq. Bras. De Cir. Dig. 2014, 27, 261–267. [Google Scholar]
- De Carvalho, M.H.C. Citocinas, Disfunção Endotelial e Resistência à Insulina. Arq. Bras. Endocrinol. Metab. 2006, 50, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Rasera, I.; Luque, A.; Junqueira, S.M.; Brasil, N.C.; Andrade, P.C. Effectiveness and Safety of Bariatric Surgery in the Public Healthcare System in Brazil: Real-World Evidence from a High-Volume Obesity Surgery Center. Obes. Surg. 2017, 27, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Avenell, A.; Bolland, M.; Hudson, J.; Stewart, F.; Robertson, C.; Sharma, P.; Fraser, C.; MacLennan, G. Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: Systematic review and meta-analysis. BMJ 2017, 359, 4849. [Google Scholar] [CrossRef] [PubMed]
- Sousa, P.; Bastos, A.P.; Venâncio, C.; Vaz, A.R.; Brandao, I.; Costa, J.M.D.; Machado, P.; Conceição, E. Compreender a Sintomatologia Depressiva após a Cirurgia Bariátrica: O Papel do Peso, da Alimentação e da Imagem Corporal. Acta Med. Port. 2014, 27, 450–458. [Google Scholar] [CrossRef]
- Santos, H.D.N.; Lima, J.M.S.; de Souza, M.F.C. Estudo comparativo da evolução nutricional de pacientes candidatos à cirurgia bariátrica assistidos pelo Sistema Único de Saúde e pela Rede Suplementar de Saúde. Ciência Saúde Coletiva 2014, 19, 1359–1365. [Google Scholar] [CrossRef]
- Ali, M.R.; Fuller, W.D.; Rasmussen, J. Detailed description of early response of metabolic syndrome after laparoscopic Roux-en-Y gastric bypass. Surg. Obes. Relat. Dis. 2009, 5, 346–351. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Rev. Esp. Salud. Publica 2008, 82, 251–259. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Andrada, P.; Valentí, V.; Rotellar, F.; Silva, C.; Catalán, V.; Rodríguez, A.; Ramírez, B.; Moncada, R.; Escalada, J.; et al. Dissociation of body mass index, excess weight loss and body fat percentage trajectories after 3 years of gastric bypass: Relationship with metabolic outcomes. Int. J. Obes. 2017, 41, 1379–1387. [Google Scholar] [CrossRef]
- Saúde. AN de. Dados e Indicadores de saúde. Dados e Indicadores Saúde [s.d.]. Available online: http://www.ans.gov.br/perfil-do-setor/dados-e-indicadores-do-setor (accessed on 14 August 2019).
- Buchner, A.; Paul, F.; Erdfelder, E.; Albert-Georg, L. G*Power 3.1 (manual): A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Diário Oficial da União. Available online: http://www.in.gov.br/web/guest/materia/-/asset_publisher/Kujrw0TZC2Mb/content/id/22175085/do1-2016-01-13-resolucao-n-2-131-de-12-de-novembro-de-2015-22174970 (accessed on 27 June 2019).
- Silva-Neto, E.F.; Vázquez, C.M.P.; Soares, F.M.; Silva, D.G.; De Souza, M.F.C.; Barbosa, K.B.F. Cirurgia bariátrica reverte risco metabólico em pacientes assistidos em nível ambulatorial. Arq. Bras. Cir. Dig. 2014, 27, 38–42. [Google Scholar] [CrossRef]
- Farinholt, G.N.; Carr, A.D.; Chang, E.J.; Ali, M.R. A call to arms: Obese men with more severe comorbid disease and underutilization of bariatric operations. Surg. Endosc. 2013, 27, 4556–4563. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Guibu, I.A.; Moraes, J.C.D.; Guerra Junior, A.A.; Costa, E.A.; Acurcio, F.D.A.; Costa, K.S.; Karnikowski, M.G.D.O.; Soeiro, O.M.; Leite, S.N.; Álvares, J. Main characteristics of patients of primary health care services in Brazil. Rev. De Saude Publica 2017, 51, 17. [Google Scholar] [CrossRef]
- Brasil, M.D.S. Vigitel Brazil 2016: Surveillance of risk and protective factors for chronic diseases by telephone survey: Estimates of sociodemographic frequency and distribution of risk and protective factors for chronic diseases in the capitals of the 26 Brazilian sta. Minist. Health Braz. 2017. [Google Scholar] [CrossRef]
- Myers, C.A.; Slack, T.; Martin, C.K.; Broyles, S.T.; Heymsfield, S.B. Regional disparities in obesity prevalence in the United States: A spatial regime analysis. Obesity 2015, 23, 481–487. [Google Scholar] [CrossRef]
- Passeri, C.R.; Andrade, J.A.C.D.C.; Tomal, K.T.; Pracucho, E.M.; Campos, L.P.D.; Sales-Peres, S.H.D.C. Masticatory function of obese candidates to Bariatric Surgery from distinct socioeconomic. ABCD. Arq. Bras. De Cir. Dig. 2016, 29, 53–58. [Google Scholar] [CrossRef]
- Brazil Ministry of Health (Brasil Ministério da Saúde). Food Guide for the Brazilian Population; Department of Primary Care BM of HS of HCD of BA: Brasília, Brasil, 2014.
- Lewis, K.H.; Edwards-Hampton, S.A.; Ard, J.D. Disparities in Treatment Uptake and Outcomes of Patients with Obesity in the USA. Curr. Obes. Rep. 2016, 5, 282–290. [Google Scholar] [CrossRef]
- Marcon, E.R.; Baglioni, S.; Bittencourt, L.; Lopes, C.L.N. What Is the Best Treatment before Bariatric Surgery? Exercise, Exercise and Group Therapy, or Conventional Waiting: A Randomized Controlled Trial. Obes. Surg. 2017, 27, 763–773. [Google Scholar] [CrossRef]
- Borisenko, O.; Colpan, Z.; Dillemans, B.; Funch-jensen, P.; Hedenbro, J.; Ahmed, A.R. Clinical Indications, Utilization, and Funding of Bariatric Surgery in Europe. Obes. Surg. 2015, 25, 1408–1416. [Google Scholar] [CrossRef]
- Gushiken, C.S.; Salate, D.; Vulcano, B.; Tardivo, A.P.; Vieira, C.; Leite, D.S.; Oliveira, M. Evolução da perda de peso entre indivíduos da fila de espera para a cirurgia bariátrica em um ambulatório multidisciplinar de atenção secundária à saúde. Medicina 2010, 43, 20–28. [Google Scholar] [CrossRef]
- Schmatz, R.; Bitencourt, M.R.; Patias, L.D.; Beck, M.; Alvarez, G.D.C.; Zanini, D.; Gutierres, J.M.; Diehl, L.N.; Pereira, L.B.; Leal, C.A.; et al. Clinica Chimica Acta Evaluation of the biochemical, in fl ammatory and oxidative pro fi le of obese patients given clinical treatment and bariatric surgery. Clin. Chim. Acta 2017, 465, 72–79. [Google Scholar] [CrossRef]
- Mulla, C.M.; Middelbeek, R.J.; Patti, M. Mechanisms of weight loss and improved metabolism following bariatric surgery. Ann. N. Y. Acad. Sci. 2018, 1411, 53–64. [Google Scholar] [CrossRef]
- Andersson, D.P.; Wahrenberg, H.; Toft, E.; Qvisth, V.; Löfgren, P.; Hertel, K.; Leijonhufvud, B.-M.; Thorell, A.; Näslund, E.; Arner, P. Waist circumference to assess reversal of insulin resistance following weight reduction after bariatric surgery: Cohort and cross-sectional studies. Int. J. Obes. 2013, 38, 438–443. [Google Scholar] [CrossRef]
- Szczuko, M.; Komorniak, N.; Hoffmann, M.; Walczak, J.; Jaroszek, A.; Kowalewski, B.; Kaseja, K.; Jamioł-Milc, D.; Stachowska, E. Body Weight Reduction and Biochemical Parameters of the Patients After, R.Y.G.B and SG Bariatric Procedures in 12-Month Observation. Obes. Surg. 2017, 27, 940–947. [Google Scholar] [CrossRef]
- Schiavon, C.A.; Bersch-Ferreira, A.C.; Santucci, E.V.; Oliveira, J.D.; Torreglosa, C.R.; Bueno, P.T.; Frayha, J.C.; Santos, R.N.; Damiani, L.P.; Noujaim, P.M.; et al. Effects of bariatric surgery in obese patients with hypertension: The GATEWAY randomized trial. Circulation 2018, 137, 1132–1142. [Google Scholar] [CrossRef]
- Nassour, I.; Almandoz, J.P.; Adams-Huet, B. Metabolic syndrome remission after Roux-en-Y gastric bypass or sleeve gastrectomy. Diabetes Metab. Syndr. Obes. 2017, 10, 393–402. [Google Scholar] [CrossRef]
- Hemmingsson, E.; Uddén, J.; Neovius, M. No Apparent Progress in Bioelectrical Impedance Accuracy: Validation Against Metabolic Risk and DXA. Obesity 2009, 17, 183–187. [Google Scholar] [CrossRef]
- Dixon, J.B.; Bhasker, A.G.; Lambert, G.W.; Lakdawala, M. Leg to leg bioelectrical impedance analysis of percentage fat mass in obese patients—Can it tell us more than we already know? Surg. Obes. Relat. Dis. 2016, 12, 1397–1402. [Google Scholar] [CrossRef]
- Bond, D.S.; Phelan, S.; Wolfe, L.G.; Evans, R.K.; Meador, J.G.; Kellum, J.M.; Maher, J.W.; Wing, R.R. Becoming Physically Active after Bariatric Surgery is Associated with Improved Weight Loss and Health-related Quality of Life. Obesity 2009, 17, 78–83. [Google Scholar] [CrossRef]
- Fontana, A.D. Bariatric Surgery Associated with Practice of Moderate to Intense Physical Activity Related to Weight Loss, Activity Level in Daily Life, Dyspnea, and Quality of Life of Sedentary Individuals with Morbid Obesity: A Prospective Longitudinal Study. Obes. Surg. 2019, 249, 2442–2448. [Google Scholar] [CrossRef]
- Pereira, C.; Monteiro, L.; Aidar, F.J.; de Matos, D.G.; de Farias Neto, J.P.; de Souza, R.F.; Sobral Sousa, A.C.; de Almeida, R.R.; Prado Nunes, M.A.; Nunes-Silva, A.; et al. Assessment of Cardiometabolic Risk Factors, Physical Activity Levels, and Quality of Life in Stratified Groups up to 10 Years after Bariatric Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1975. [Google Scholar] [CrossRef] [Green Version]
- Elbelt, U.; Schuetz, T.; Hoffmann, I.; Pirlich, M.; Strasburger, C.J.; Lochs, H. Differences of energy expenditure and physical activity patterns in subjects with various degrees of obesity. Clin. Nutr. 2010, 29, 766–772. [Google Scholar] [CrossRef]
- Jacobi, D.; Ciangura, C.; Couet, C.; Oppert, J. Physical activity and weight loss following bariatric surgery. Obes. Rev. 2010, 12, 366–377. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AORC Score | Diabetes Mellitus |
|---|---|
| 0 | Absence |
| 1 | Glucose intolerance (≥100 e < 126 mg/DL) |
| 2 | Diabetes mellitus (diagnosed) |
| 3 | Controlled with oral antidiabetic |
| 4 | Insulin therapy |
| 5 | Clinical complications |
| Dyslipidemias | |
| 0 | Absence |
| 1 | Borderline (200–239 mg/DL) |
| 2 | Conventional control (diet + physical activity) |
| 3 | Single medicinal product |
| 4 | Multiple medications |
| 5 | Uncontrolled |
| Systemic Blood Hypertension | |
| 0 | Absence |
| 1 | Borderline values (systolic: 130–139 mmHg, diastolic: 85–89 mmHg) |
| 2 | Conventional control (diet + physical activity) |
| 3 | Single medicinal product |
| 4 | Multiple medications |
| 5 | Uncontrolled |
| Variables | Total n = 111 | PUS n = 60 | PHS n = 51 | p |
|---|---|---|---|---|
| Age (years) | 39.6 ± 10.8 | 42.5 ± 9.4 | 37.4 ± 12.0 | 0.048 1 |
| Comorbidities | ||||
| SAH | 81 (73.0) | 50 (83.3) | 31 (60.8) | 0.008 2 |
| Dyslipidemia | 65 (58.6) | 39 (65.0) | 26 (51.0) | 0.135 2 |
| Diabetes Mellitus | 39 (35.1) | 27 (45.0) | 12 (23.5) | 0.018 2 |
| Admission time to the pre-surgery period (months) 2 | 10 (2; 20) | 17 (13; 28.5) | 2 (2; 6) | <0.001 2 |
| Gender | n (%) | n (%) | n (%) | |
| Female | 80 (72.1) | 45 (75.0) | 35 (68.6) | 0.46 3 |
| Nutritional status | <0.001 3 | |||
| Overweight | 1 (0.9) | 0 | 1 (1.9) | |
| Obesity I | 27 (24.3) | 2 (3.3) | 25 (49.0) | |
| Obesity II | 48 (43.2) | 27 (45.0) | 21 (41.0) | |
| Severe obesity III | 35 (31.5) | 31 (51.6) | 4 (7.8) |
| AORC SCORE | Diabetes Mellitus | Dyslipidemia | SAH | ||||||
|---|---|---|---|---|---|---|---|---|---|
| PUS N = 60 | PHS N = 51 | p | PUS N = 60 | PHS N = 51 | p | PUS N = 60 | PHS N = 51 | p | |
| Admission | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||
| ≤2 | 40 (66.7) | 43 (84.3) | 0.033 1 | 27 (45.0) | 40 (78.4) | <0.0001 1 | 13 (21.7) | 22 (43.1) | 0.015 1 |
| ≥3 | 20 (33.3) | 8 (15.7) | 33 (55.0) | 11 (21.6) | 47 (78.3) | 29 (56.2) | |||
| Pre-surgery | |||||||||
| ≤2 | 42 (70.0) | 46 (90.2) | 0.009 1 | 31 (51.7) | 43 (84.3) | <0.000 | 13 (15.4) | 31 (3.7) | <0.001 2 |
| ≥3 | 18 (30.0) | 5 (9.0) | 29 (48.3) | 8 (15.7) | 47 (78.3) | 20 (39.2) | |||
| Post-surgery 3 months | |||||||||
| ≤2 | 56 (93.3) | 48 (94.1) | 54 (90.0) | 46 (90.2) | 0.937 1 | 42 (70.0) | 44 (86.3) | 0.067 2 | |
| ≥3 | 4 (6.7) | 3 (5.9) | 1 | 6 (10.0) | 5 (9.8) | 18 (30.0) | 17 (13.7) | ||
| Post-surgery 6 months | |||||||||
| ≤2 | 56 (93.3) | 50 (98.0) | 0.372 2 | 56 (93.3) | 47 (92.2) | 0.811 | 45 (75.0) | 46 (90.2) | 0.157 1 |
| ≥3 | 4 (6.7) | 1 (2.0) | 4 (6.7) | 4 (7.8) | 15 (25.0) | 5 (9.8) | |||
| Post-surgery 12 months | |||||||||
| ≤2 | 58 (96.7) | 50 (98.0) | 1 | 27 (45.0) | 40 (78.4) | 1 1 | 48 (80.0) | 47 (92.2) | |
| ≥3 | 2 (3.3) | 1 (2.0) | 33 (11.0) | 11 (21.6) | 12 (20.0) | 4 (7.8) | 0.069 1 | ||
| Variables | PUS N = 60 | PHS N = 51 | p |
|---|---|---|---|
| Pre-surgery Nutritional Status 1 | n (%) | n (%) | <0.0001 |
| Overweight | 0 | 1 (1.9) | |
| Obesity I | 13 (21.6) | 34 (66.6) | |
| Obesity II | 20 (33.3) | 14 (27.5) | |
| Severe Obesity III | 27 (44.9) | 2 (3.8) | |
| Post-surgery Nutritional Status 12 months 1 | <0.0001 | ||
| Eutrophic | 3 (5.0) | 9 (17.6) | |
| Overweight | 9 (31.7) | 29 (56.9) | |
| Obesity I | 9 (15.0) | 10 (19.6) | |
| Obesity II | 14 (23.3) | 2 (3.9) | |
| Severe Obesity III | 15 (24.9) | 1 (1.9) | |
| X ± DP | X ± DP | ||
| Weight loss percentage | 63.3 ± 25.6 | 80.0 ± 25.6 | 0.002 |
| Weight admission (kg) | 133.8 ± 28.1 | 114.7 ± 22.1 | <0.0001 |
| Pre-surgery weight (kg) | 126.4 ± 27.0 | 109.5 ± 19.5 | <0.0001 |
| Current weight (kg) | 90.3 ± 22.8 | 79.3 ± 16.6 | <0.0001 |
| BMI admission (Kg/m2) | 51.5 ± 9.4 | 41.1 ± 5.4 | <0.0001 |
| BMI pre-surgery (Kg/m2) | 48.7 ± 9.2 | 39.2 ± 4.4 | <0.0001 |
| Post-surgery BMI (Kg/m2) | 34.8 ± 8.7 | 28.4 ± 4.3 | <0.0001 |
| Waist circumference (cm) | 128.17 ± 15.3 | 114.3 ± 13.0 | 0.033 |
| Final waist circumference (cm) | 105.7 ± 17.6 | 99.2 ± 12.0 | 0.028 |
| Waist/initial height ratio | 0.78 ± 0.09 | 0.68 ± 0.66 | <0.0001 |
| Waist/final height ratio | 0.64 ± 0.13 | 0.59 ± 0.06 | 0.010 |
| PUS | PHS | |||||
|---|---|---|---|---|---|---|
| Variables | Preoperative | Postoperative 3 | Postoperative 6 | Preoperative | Postoperative 3 | Postoperative 6 |
| Fasting Blood Glucose | 90.4 ± 15.4 | 87.3 ± 13.5 | 79.7 ± 8.6 | 96.8 ± 23.3 | 85.3 ± 8.7 | 83.3 ± 5.8 |
| Triglycerides | 134.2 ± 76.7 | 110.6 ± 47.8 | 81.4 ± 30.7 | 155.9 ± 72. 3 | 112.6 ± 48.6 | 86.8 ± 24.6 |
| Total cholesterol | 182.5 ± 37.5 | 174.6 ± 35.3 | 148.3 ± 27.9 | 203.0 ± 40.2 | 175.4 ± 34.5 | 174.0 ± 30.3 |
| LDL | 111.7 ± 29.6 | 111.2 ± 29.0 | 88.7 ± 28.2 | 127.3 ± 32.8 | 113.3 ± 25.8 | 101.4 ± 29.1 |
| HDL | 45.2 ± 9.4 | 44.2 ± 10.5 | 45.0 ± 11.4 | 41.5 ± 9.0 | 40.7 ± 9.9 | 48.7 ± 13.6 |
| Variables | p * | Size of Effect (η2) | Observed Power |
|---|---|---|---|
| Time Effect for: | |||
| HDL | 0.008 | 0.090 | 0.807 |
| LDL | <0.0001 | 0.340 | 1.000 |
| total cholesterol | <0.0001 | 0.284 | 1.000 |
| Triglycerides | <0.0001 | 0.455 | 1.000 |
| Fasting glucose | <0.0001 | 0.197 | 1.000 |
| Effect between groups to: | |||
| HDL | 0.014 | 0.080 | 0.750 |
| LDL | 0.046 | 0.058 | 0.595 |
| Total cholesterol | <0.001 | 0.063 | 0.920 |
| Triglycerides | 0.363 | 0.020 | 0.225 |
| Fasting glucose | 0.057 | 0.029 | 0.563 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocha de Almeida, R.; Cândido de Souza, M.F.; Gama de Matos, D.; Monteiro Costa Pereira, L.; Batista Oliveira, V.; Menezes Oliveira, J.L.; Soares Barreto-Filho, J.A.; Almeida-Santos, M.A.; de Souza, R.F.; de Freitas Zanona, A.; et al. A Retrospective Study about the Differences in Cardiometabolic Risk Indicators and Level of Physical Activity in Bariatric Surgery Patients from Private vs. Public Units. Int. J. Environ. Res. Public Health 2019, 16, 4751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234751
Rocha de Almeida R, Cândido de Souza MF, Gama de Matos D, Monteiro Costa Pereira L, Batista Oliveira V, Menezes Oliveira JL, Soares Barreto-Filho JA, Almeida-Santos MA, de Souza RF, de Freitas Zanona A, et al. A Retrospective Study about the Differences in Cardiometabolic Risk Indicators and Level of Physical Activity in Bariatric Surgery Patients from Private vs. Public Units. International Journal of Environmental Research and Public Health. 2019; 16(23):4751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234751
Chicago/Turabian StyleRocha de Almeida, Rebeca, Márcia Ferreira Cândido de Souza, Dihogo Gama de Matos, Larissa Monteiro Costa Pereira, Victor Batista Oliveira, Joselina Luzia Menezes Oliveira, José Augusto Soares Barreto-Filho, Marcos Antonio Almeida-Santos, Raphael Fabrício de Souza, Aristela de Freitas Zanona, and et al. 2019. "A Retrospective Study about the Differences in Cardiometabolic Risk Indicators and Level of Physical Activity in Bariatric Surgery Patients from Private vs. Public Units" International Journal of Environmental Research and Public Health 16, no. 23: 4751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234751