Multiple Linear Regression-Structural Equation Modeling Based Development of the Integrated Model of Perceived Neighborhood Environment and Quality of Life of Community-Dwelling Older Adults: A Cross-Sectional Study in Nanjing, China


Abstract
:1. Background
1.1. QoL Assessments
1.2. Neighborhood Environment and Older Adults
2. Materials and Methods
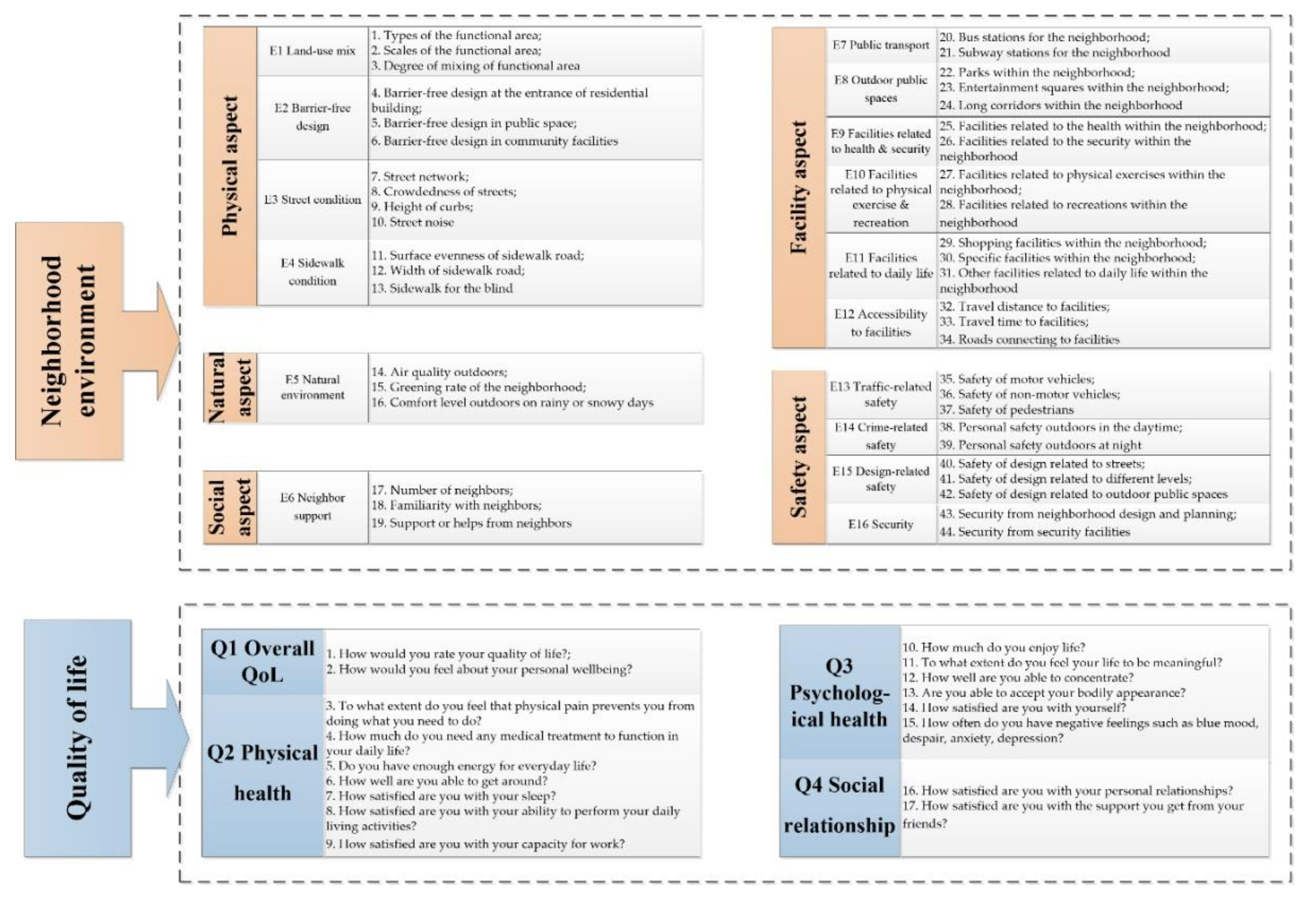
2.1. Questionnaire Design
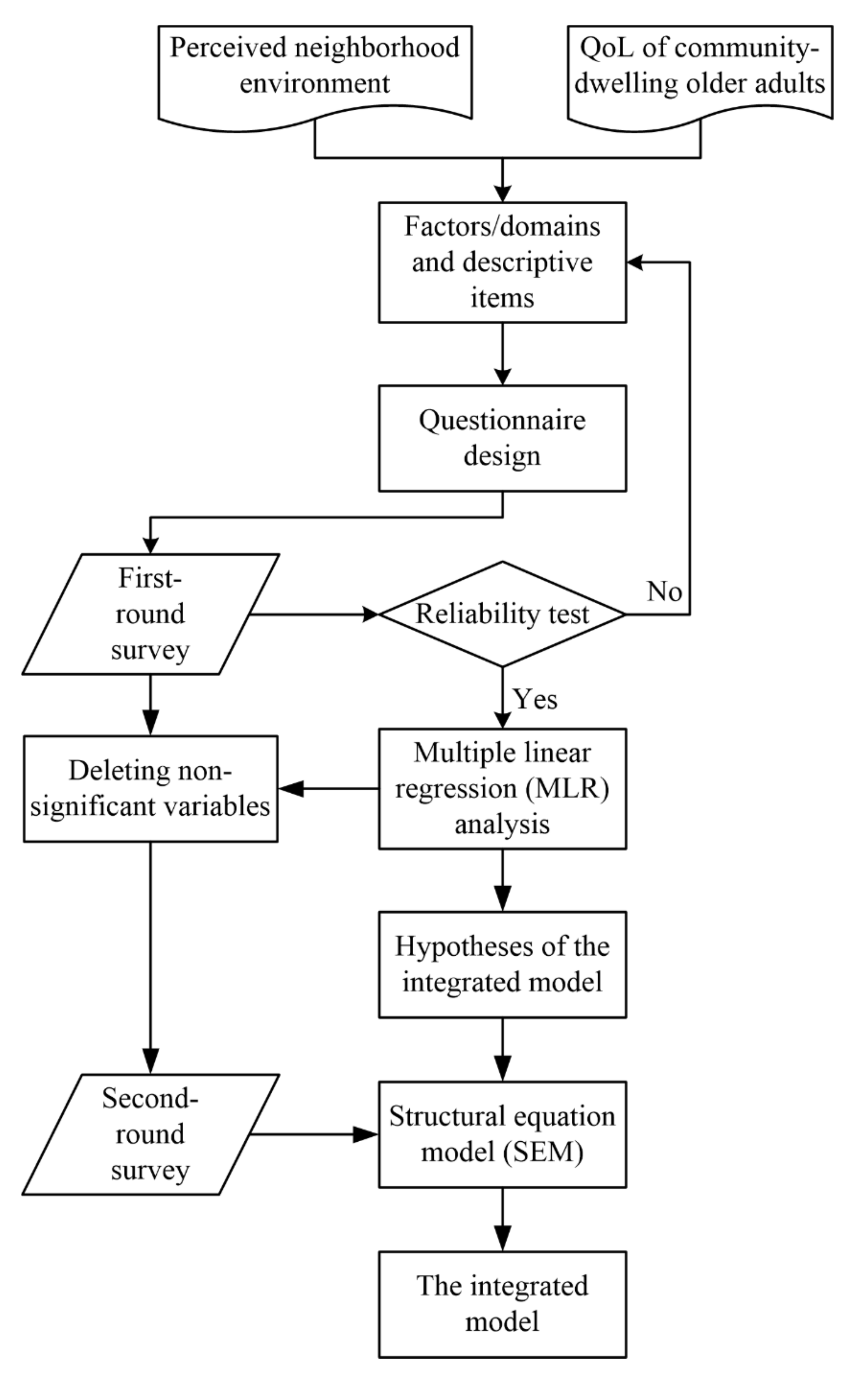
2.2. Data Analysis
2.3. Sampling and Data Collection
3. Results
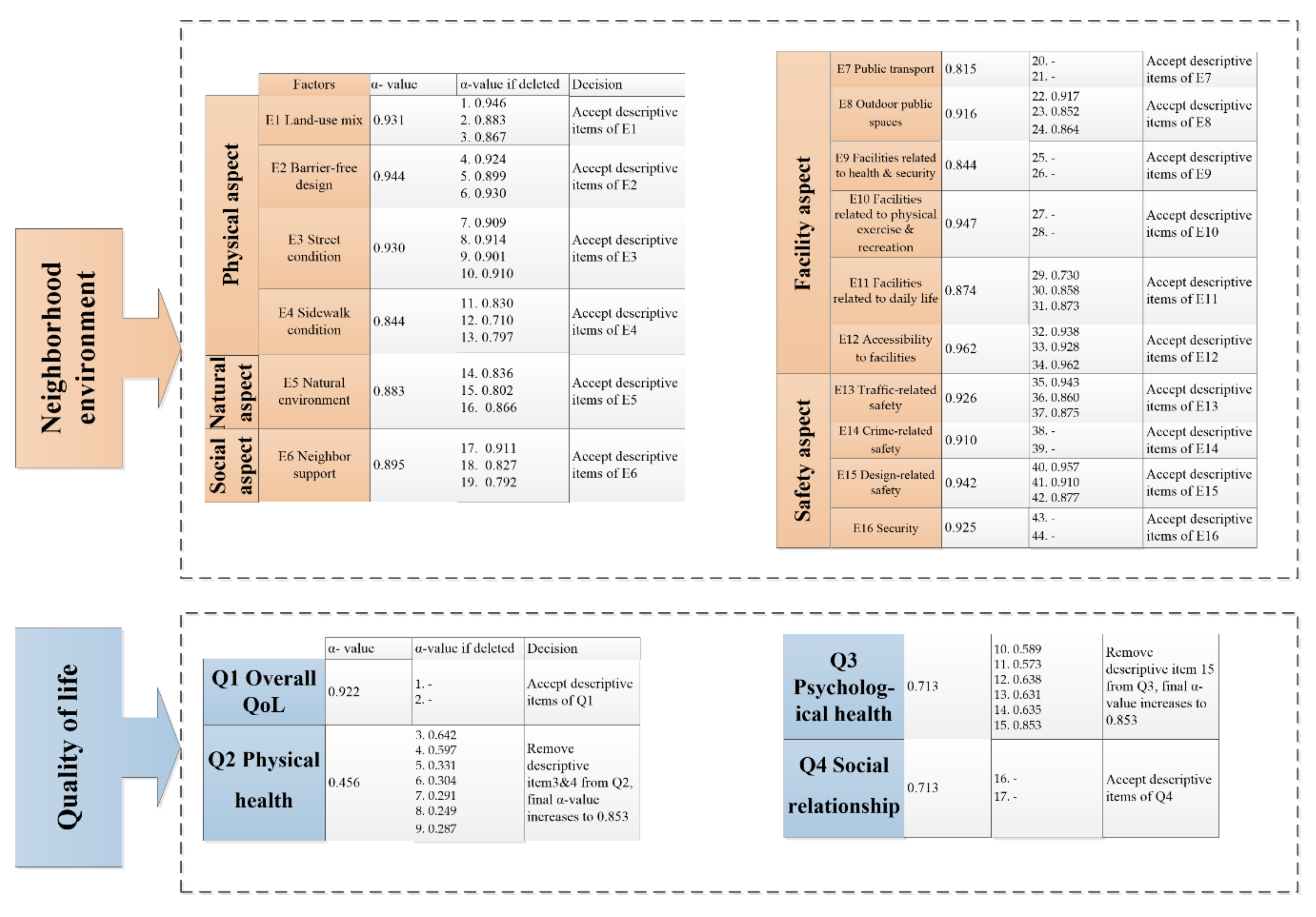
3.1. Results of Reliability Test of the Questionnaire
3.2. Results of MLR Analysis
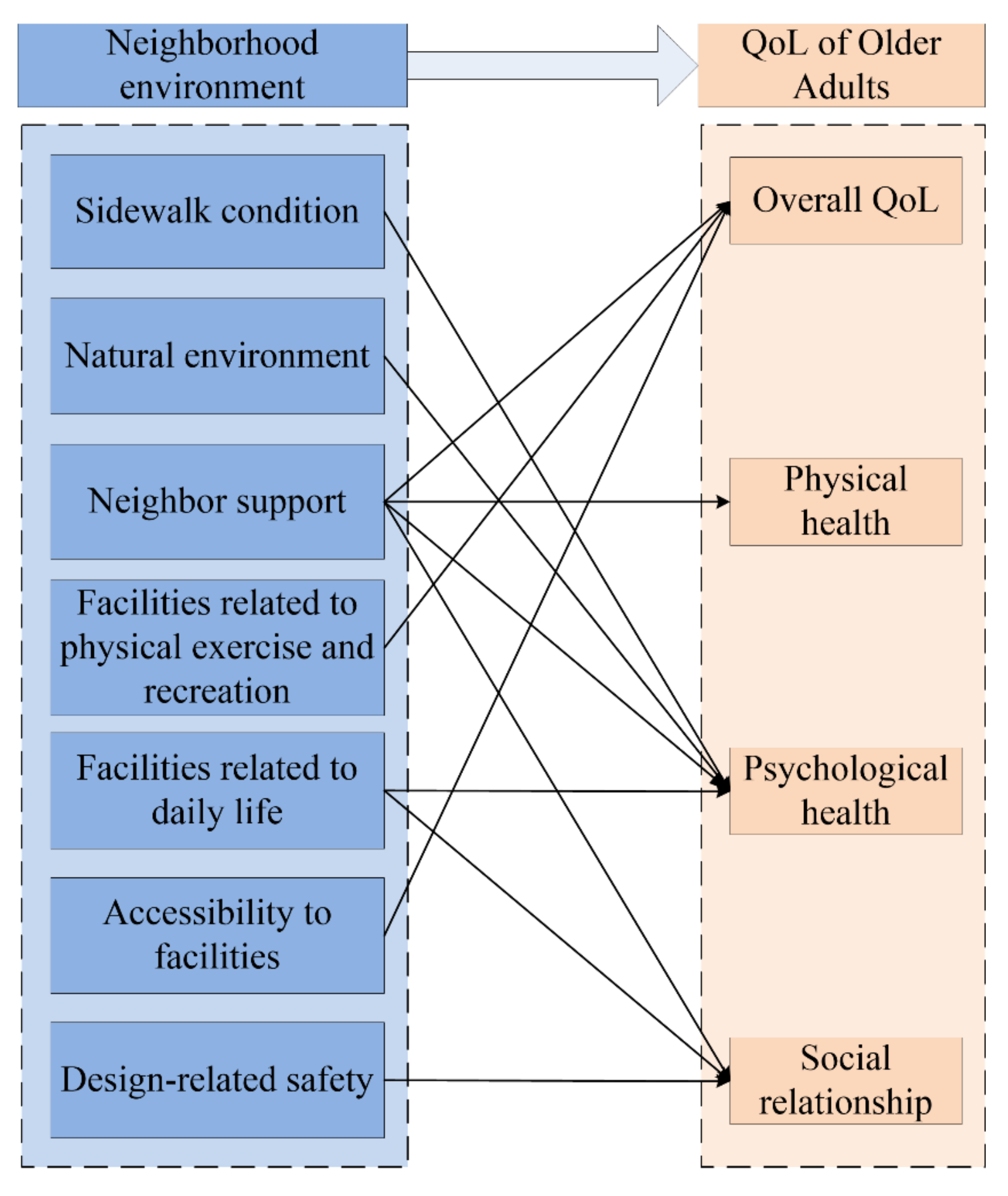
3.3. Hypothesis of the Integrated Model
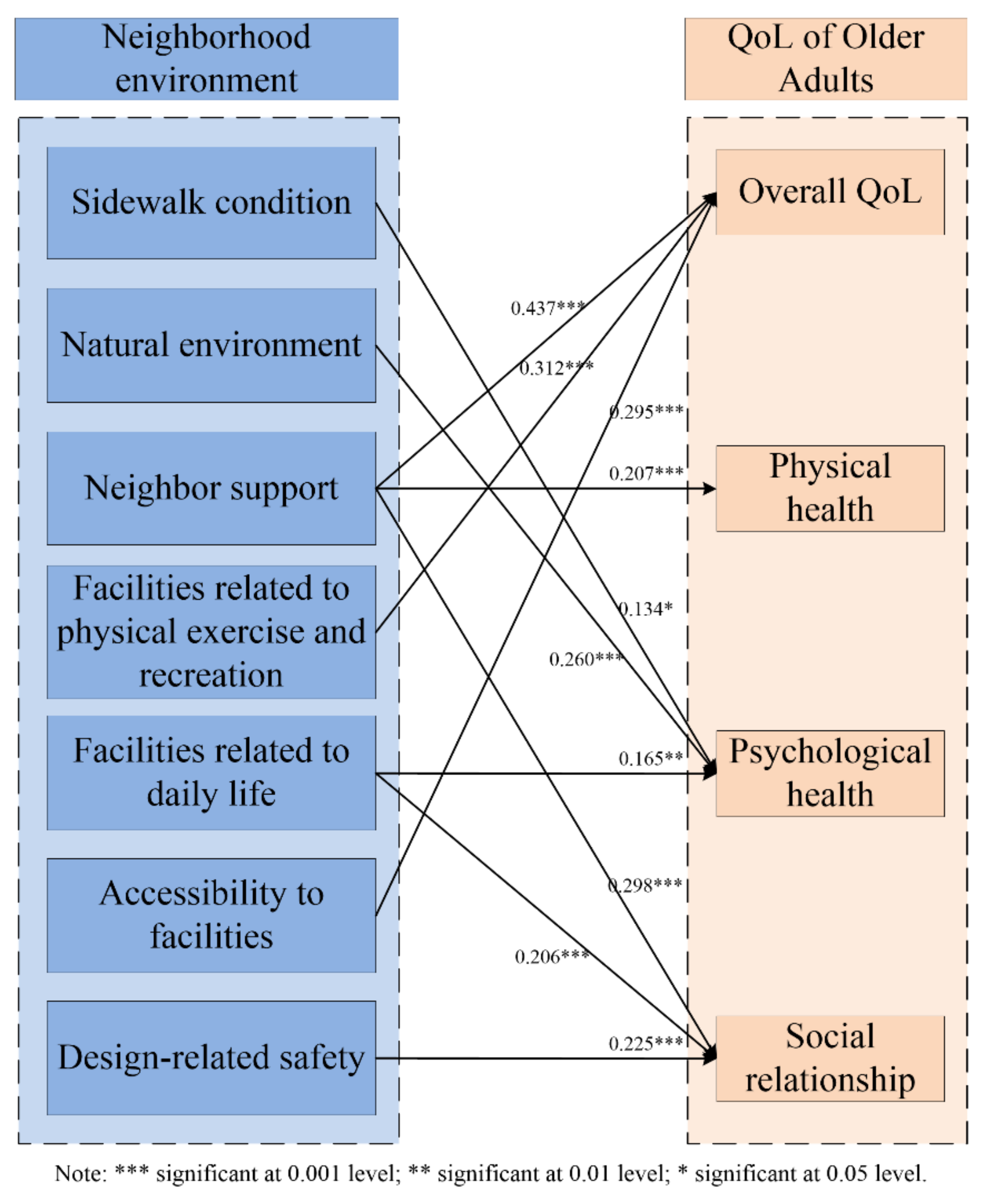
3.4. Results of SEM of the Integrated Model
4. Discussion
4.1. Physical Aspect
4.2. Natural Aspect
4.3. Social Aspect
4.4. Facility Aspect
4.5. Safety Aspect
5. Conclusions and Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations. World Population Ageing 2015; Department of Economic and Social Affairs, Population Division, Ed.; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Golant, S.M. Aging in the Right Place; Health Preofession Press: Baltimore, MD, USA, 2015. [Google Scholar]
- Chen, L.; Han, W.J. Shanghai: Front-runner of community-based elder care in China. J. Aging Soc. Policy 2016, 28, 292–307. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xu, L.; Chi, I. Perceived need for home and community-based services: Experiences of urban Chinese older adults with functional impairments. J. Aging Soc. Policy 2017, 29, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Loo, B.P.; Lam, W.W.; Mahendran, R.; Katagiri, K. How is the neighborhood environment related to the health of seniors living in Hong Kong, Singapore, and Tokyo? Some insights for promoting aging in place. Ann. Am. Assoc. Geogr. 2017, 107, 812–828. [Google Scholar] [CrossRef]
- Loo, B.P.Y.; Mahendran, R.; Katagiri, K.; Lam, W.W.Y. Walking, neighbourhood environment and quality of life among older people. Curr. Opin. Environ. Sustain. 2017, 25, 8–13. [Google Scholar] [CrossRef]
- Chaudhury, H.; Mahmood, A.; Michael, Y.L.; Campo, M.; Hay, K. The influence of neighborhood residential density, physical and social environments on older adults’ physical activity: An exploratory study in two metropolitan areas. J. Aging Stud. 2012, 26, 35–43. [Google Scholar] [CrossRef]
- Nicklett, E.J.; Lohman, M.C.; Smith, M.L. Neighborhood environment and falls among community-dwelling older adults. Int. J. Environ. Res. Public Health 2017, 14, 175. [Google Scholar] [CrossRef] [Green Version]
- Doumit, J.; Nasser, R. Quality of life and wellbeing of the elderly in Lebanese nursing homes. Int. J. Health Care Qual. Assur. 2010, 23, 72–93. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Feeny, D.H.; Patrick, D.L. Measuring Health-related quality of life. Ann. Int. Med. 1993, 118, 622–629. [Google Scholar] [CrossRef]
- The WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- World Health Organization. WHOQOL-BREF: Introduction, Administration, Scoring and Generic Version of the Assessment (Field Trial Version); World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Engel, L.; Chudyk, A.M.; Ashe, M.C.; McKay, H.A.; Whitehurst, D.G.T.; Bryan, S. Older adults’ quality of life—Exploring the role of the built environment and social cohesion in community-dwelling seniors on low income. Soc. Sci. Med. 2016, 164, 1–11. [Google Scholar] [CrossRef]
- Zhao, Y.; Chung, P.K. Neighborhood environment walkability and health-related quality of life among older adults in Hong Kong. Arch. Gerontol Geriatr. 2017, 73, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.Y.; Ma, G.X.; Jiang, X.Y. Impact of the built environment and care services within rural nursing homes in China on quality of life for elderly residents. Eng. Constr. Archit. Manag. 2017, 24, 1170–1183. [Google Scholar] [CrossRef]
- Koehn, S.D.; Mahmood, A.N.; Stott-Eveneshen, S. Quality of life for diverse older adults in assisted living: The centrality of control. J. Gerontol. Soc. Work 2016, 59, 512–536. [Google Scholar] [CrossRef] [PubMed]
- Parra, D.C.; Gomez, L.F.; Sarmiento, O.L.; Buchner, D.; Brownson, R.; Schimd, T.; Gomez, V.; Lobelo, F. Perceived and objective neighborhood environment attributes and health related quality of life among the elderly in Bogota, Colombia. Soc. Sci. Med. 2010, 70, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.; Parikh, N.S.; Giunta, N.; Fahs, M.C.; Gallo, W.T. The influence of neighborhood factors on the quality of life of older adults attending New York City senior centers: results from the Health Indicators Project. Qual. Life Res. 2012, 21, 123–131. [Google Scholar] [CrossRef]
- Levasseur, M.; Desrosiers, J.; Noreau, L. Relationships between environment and quality of life of older adults with physical disabilities. Phys. Occup. Ther. Geriatr. 2004, 22, 37–53. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Kubzansky, L.; Berkman, L.; Fay, M.; Kawachi, I. Neighborhood effects on the self-rated health of elders: Uncovering the relative importance of structural and service-related neighborhood environments. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2006, 61, S153–S160. [Google Scholar] [CrossRef] [Green Version]
- Chaudhury, H.; Campo, M.; Michael, Y.; Mahmood, A. Neighbourhood environment and physical activity in older adults. Soc. Sci. Med. 2016, 149, 104–113. [Google Scholar] [CrossRef]
- Mooney, S.J.; Joshi, S.; Cerda, M.; Kennedy, G.J.; Beard, J.R.; Rundle, A.G. Contextual correlates of physical activity among older adults: A neighborhood environment-wide association study (NE-WAS). Cancer Epidemiol. Biomark. Prev. 2017, 26, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.Y.; Wong, G.H.; Lum, T.Y.; Lou, V.W.; Ho, A.H.; Luo, H.; Tong, T.L. Neighborhood support network, perceived proximity to community facilities and depressive symptoms among low socioeconomic status Chinese elders. Aging Mental Health 2016, 20, 423–431. [Google Scholar] [CrossRef]
- Fernández-Carro, C.; Módenes, J.A.; Spijker, J. Living conditions as predictor of elderly residential satisfaction. A cross-European view by poverty status. Eur. J. Ageing 2015, 12, 187–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, T.; Chen, Y.; Zhu, J.; Liu, P. Effect of air pollution and rural-urban difference on mental health of the elderly in China. Iran. J. Public Health 2015, 44, 1084–1094. [Google Scholar] [PubMed]
- Zhang, Z.; Zhang, J. Perceived residential environment of neighborhood and subjective well-being among the elderly in China: A mediating role of sense of community. J. Environ. Psychol. 2017, 51, 82–94. [Google Scholar] [CrossRef] [Green Version]
- Yan, B.; Gao, X.; Lyon, M. Modeling satisfaction amongst the elderly in different Chinese urban neighborhoods. Soc. Sci. Med. 2014, 118, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.H.; Li, S.H.; Sung, W.Y. The study of perceived environment and its relation to senior citizen’s physical activity behavior intention. J. Bus. Res. 2016, 69, 2259–2264. [Google Scholar] [CrossRef]
- Clarke, P.J.; Weuve, J.; Barnes, L.; Evans, D.A.; Mendes de Leon, C.F. Cognitive decline and the neighborhood environment. Ann. Epidemiol. 2015, 25, 849–854. [Google Scholar] [CrossRef] [Green Version]
- Dujardin, C.; Lorant, V.; Thomas, I. Self-assessed health of elderly people in Brussels: Does the built environment matter? Health Plan 2014, 27, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Vogt, S.; Mielck, A.; Berger, U.; Grill, E.; Peters, A.; Doring, A.; Holle, R.; Strobl, R.; Zimmermann, A.K.; Linkohr, B.; et al. Neighborhood and healthy aging in a German city: Distances to green space and senior service centers and their associations with physical constitution, disability, and health-related quality of life. Eur. J. Ageing 2015, 12, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Li, D.; Ahrentzen, S.; Feng, H. Exploring the inner relationship among neighborhood environmental factors affecting quality of life of older adults based on SLR–ISM method. J. Hous. Built. Environ. 2019, 1–28. [Google Scholar] [CrossRef]
- Zhang, F.; Li, D. How the urban neighborhood environment influences the quality of life of Chinese community-dwelling older adults: An influence model of “NE-QoL”. Sustainability 2019, 11, 5739. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: International Version; Pearson Education: London, UK, 2009. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Li, X.N.; Chen, W.P.; Cundy, A.B.; Chang, A.C.; Jiao, W.T. Analysis of influencing factors on public perception in contaminated site management: Simulation by structural equation modeling at four sites in China. J. Environ. Manag. 2018, 210, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M. Structural Equation Model: Orperation and Application of AMOS; Chongqing University Press: Chongqing, China, 2010. [Google Scholar]
- Whitfield, G.P.; Carlson, S.A.; Ussery, E.N.; Watson, K.B.; Adams, M.A.; James, P.; Brownson, R.C.; Berrigan, D.; Fulton, J.E. Environmental supports for physical activity, national health interview survey—2015. Am. J. Prev. Med. 2018, 54, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Brenner, A.B.; Clarke, P.J. Difficulty and independence in shopping among older Americans: more than just leaving the house. Disabil. Rehabil. 2019, 41, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Ruengtam, P. Factor analysis of built environment design and management of residential communities for enhancing the wellbeing of elderly people. Proc. Eng. 2017, 180, 966–974. [Google Scholar] [CrossRef]
- Soma, Y.; Tsunoda, K.; Kitano, N.; Jindo, T.; Tsuji, T.; Saghazadeh, M.; Okura, T. Relationship between built environment attributes and physical function in Japanese community-dwelling older adults. Geriatr. Gerontol. Int. 2017, 17, 382–390. [Google Scholar] [CrossRef]
- Liu, X. General description of sparial accessibility. Urb. Transp. China 2007, 6, 36–43. [Google Scholar]
- Ingram, D.R. The concept of accessibility: A search for an operational form. Reg. Stud. 1971, 5, 101–107. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Information of Respondents | Options | Frequency | Percentage |
|---|---|---|---|
| Age | 60–69 | 296 | 65.05% |
| 70–79 | 68 | 14.95% | |
| ≥80 | 91 | 20.00% | |
| Gender | Female | 223 | 49.01% |
| Male | 232 | 50.99% | |
| Type of community | Commercial housing | 245 | 53.85% |
| Affordable housing | 125 | 27.47% | |
| Self-built housing | 69 | 15.16% | |
| Others | 16 | 3.52% | |
| Who they live with | Live alone | 38 | 8.35% |
| Live with partner | 284 | 62.42% | |
| Live with children | 117 | 25.71% | |
| Others | 16 | 3.52% | |
| Length of residence | ≤5 years | 112 | 24.62% |
| 5–10 years | 109 | 23.96% | |
| ≥10 years | 234 | 51.42% |
| Regression Equation | B | S.E. | T | Sig.T | R | R2 | F | Sig. | |
|---|---|---|---|---|---|---|---|---|---|
| Q1 Overall QoL | Constant | 1.032 | 0.208 | 4.970 | 0.000 | 0.679 | 0.462 | 53.743 | 0.000 |
| E6 | 0.384 | 0.073 | 5.244 | 0.000 | |||||
| E12 | 0.226 | 0.072 | 3.125 | 0.002 | |||||
| E10 | 0.123 | 0.060 | 2.085 | 0.038 | |||||
| Q2 Physical health | Constant | 2.454 | 0.232 | 10.581 | 0.000 | 0.324 | 0.105 | 22.538 | 0.000 |
| E6 | 0.301 | 0.064 | 4.728 | 0.000 | |||||
| Q3 Psychological health | Constant | 0.394 | 0.473 | 0.833 | 0.406 | 0.512 | 0.263 | 16.640 | 0.000 |
| E11 | 0.324 | 0.065 | 4.959 | 0.000 | |||||
| E6 | 0.151 | 0.075 | 2.009 | 0.046 | |||||
| E4 | 0.254 | 0.075 | 3.410 | 0.001 | |||||
| E5 | 0.187 | 0.078 | 2.386 | 0.018 | |||||
| Q4 Social relationship | Constant | 0.444 | 0.531 | 0.836 | 0.404 | 0.545 | 0.297 | 26.450 | 0.000 |
| E6 | 0.466 | 0.075 | 6.183 | 0.000 | |||||
| E11 | 0.268 | 0.075 | 3.577 | 0.000 | |||||
| E15 | 0.205 | 0.087 | 2.359 | 0.019 | |||||
| Fit Indices | Acceptable Range | Measured Value |
|---|---|---|
| df | − | 496 |
| x2 | − | 1253.404 |
| x2/df | <3 | 2.527 |
| GFI | >0.8 | 0.846 |
| AGFI | >0.8 | 0.836 |
| CFI | >0.9 | 0.921 |
| RMSEA | <0.08 | 0.058 |
| NNFI | >0.9 | 0.910 |
| IFI | >0.9 | 0.921 |
| Path | Beta | B | S.E. | T | Sig. |
|---|---|---|---|---|---|
| Psychological health ← Sidewalk condition | 0.134 | 0.097 | 0.041 | 2.353 | * |
| Psychological health ← Natural environment | 0.260 | 0.159 | 0.036 | 4.369 | *** |
| Overall QoL ← Neighbor support | 0.437 | 0.471 | 0.061 | 7.771 | *** |
| Social relationship ← Neighbor support | 0.298 | 0.327 | 0.075 | 4.356 | *** |
| Overall QoL ← Facilities related to physical exercise and recreation | 0.312 | 0.325 | 0.053 | 6.079 | *** |
| Psychological health ← Facilities related to daily life | 0.165 | 0.105 | 0.038 | 2.793 | ** |
| Physical health ← Neighbor support | 0.207 | 0.185 | 0.047 | 3.970 | *** |
| Overall QoL ← Accessibility to facilities | 0.295 | 0.311 | 0.055 | 5.649 | *** |
| Social relationship ← Facilities related to daily life | 0.206 | 0.192 | 0.054 | 3.588 | *** |
| Social relationship ← Design-related safety | 0.225 | 0.209 | 0.060 | 3.485 | *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, F.; Li, D. Multiple Linear Regression-Structural Equation Modeling Based Development of the Integrated Model of Perceived Neighborhood Environment and Quality of Life of Community-Dwelling Older Adults: A Cross-Sectional Study in Nanjing, China. Int. J. Environ. Res. Public Health 2019, 16, 4933. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16244933
Zhang F, Li D. Multiple Linear Regression-Structural Equation Modeling Based Development of the Integrated Model of Perceived Neighborhood Environment and Quality of Life of Community-Dwelling Older Adults: A Cross-Sectional Study in Nanjing, China. International Journal of Environmental Research and Public Health. 2019; 16(24):4933. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16244933
Chicago/Turabian StyleZhang, Fan, and Dezhi Li. 2019. "Multiple Linear Regression-Structural Equation Modeling Based Development of the Integrated Model of Perceived Neighborhood Environment and Quality of Life of Community-Dwelling Older Adults: A Cross-Sectional Study in Nanjing, China" International Journal of Environmental Research and Public Health 16, no. 24: 4933. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16244933