Sarcoid-Like Granulomatous Disease: Pathologic Case Series in World Trade Center Dust Exposed Rescue and Recovery Workers

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Pulmonary Function Testing (PFT)
2.3. CT Scans
2.4. Sample Collection, Histology and Immunohistochemistry
3. Results
3.1. Patient Demographics and Diagnoses
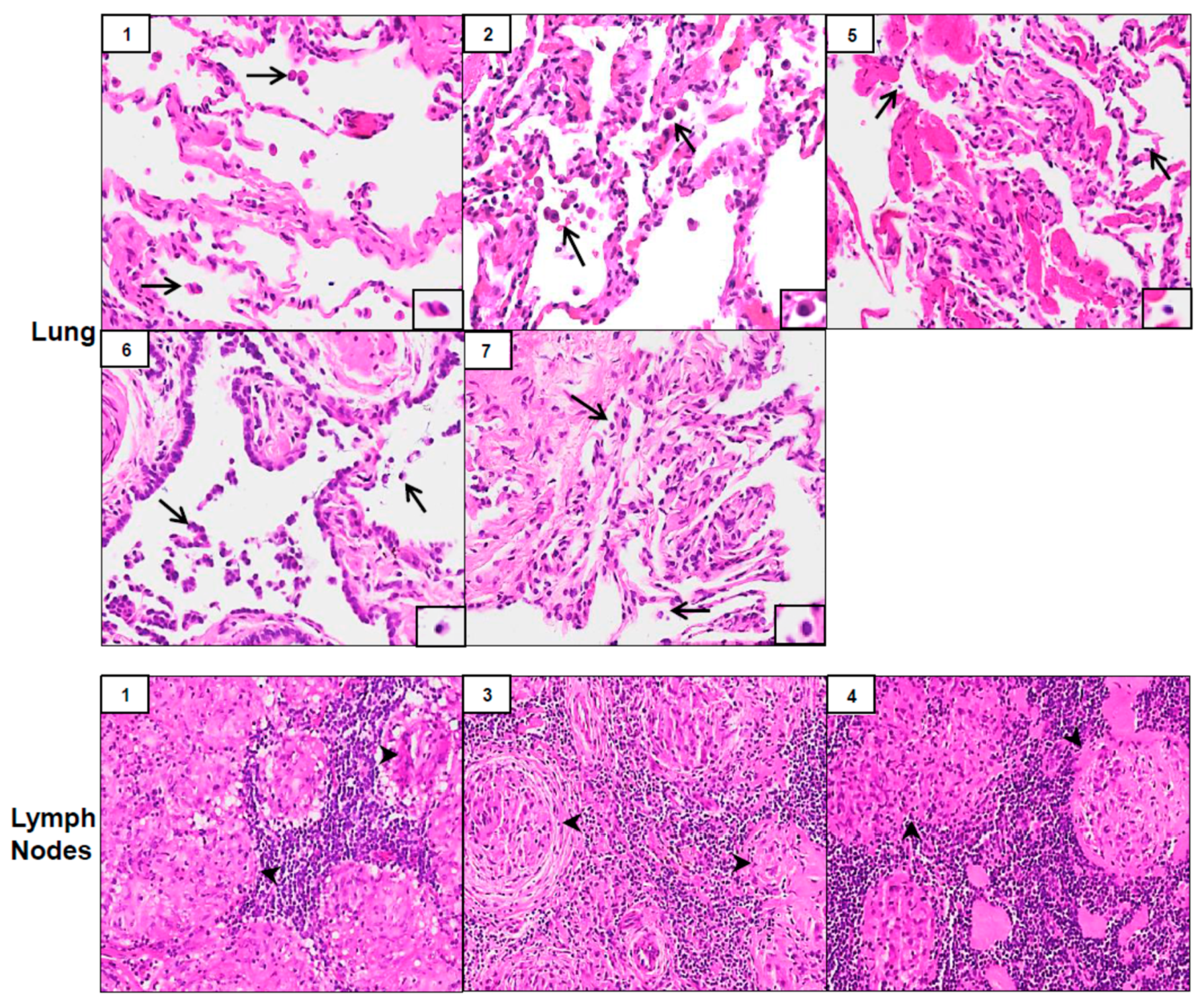
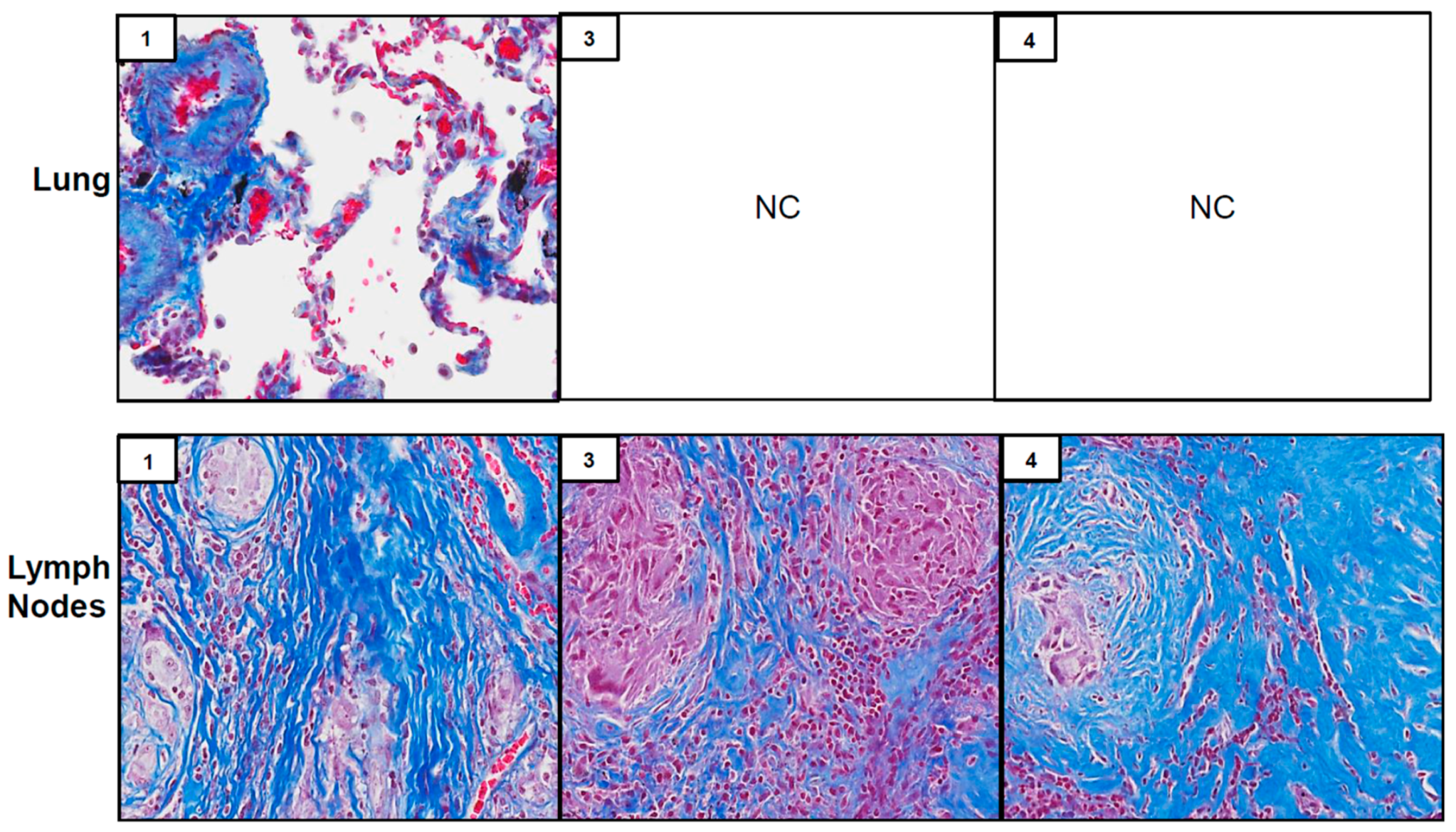
3.2. Pathological Results
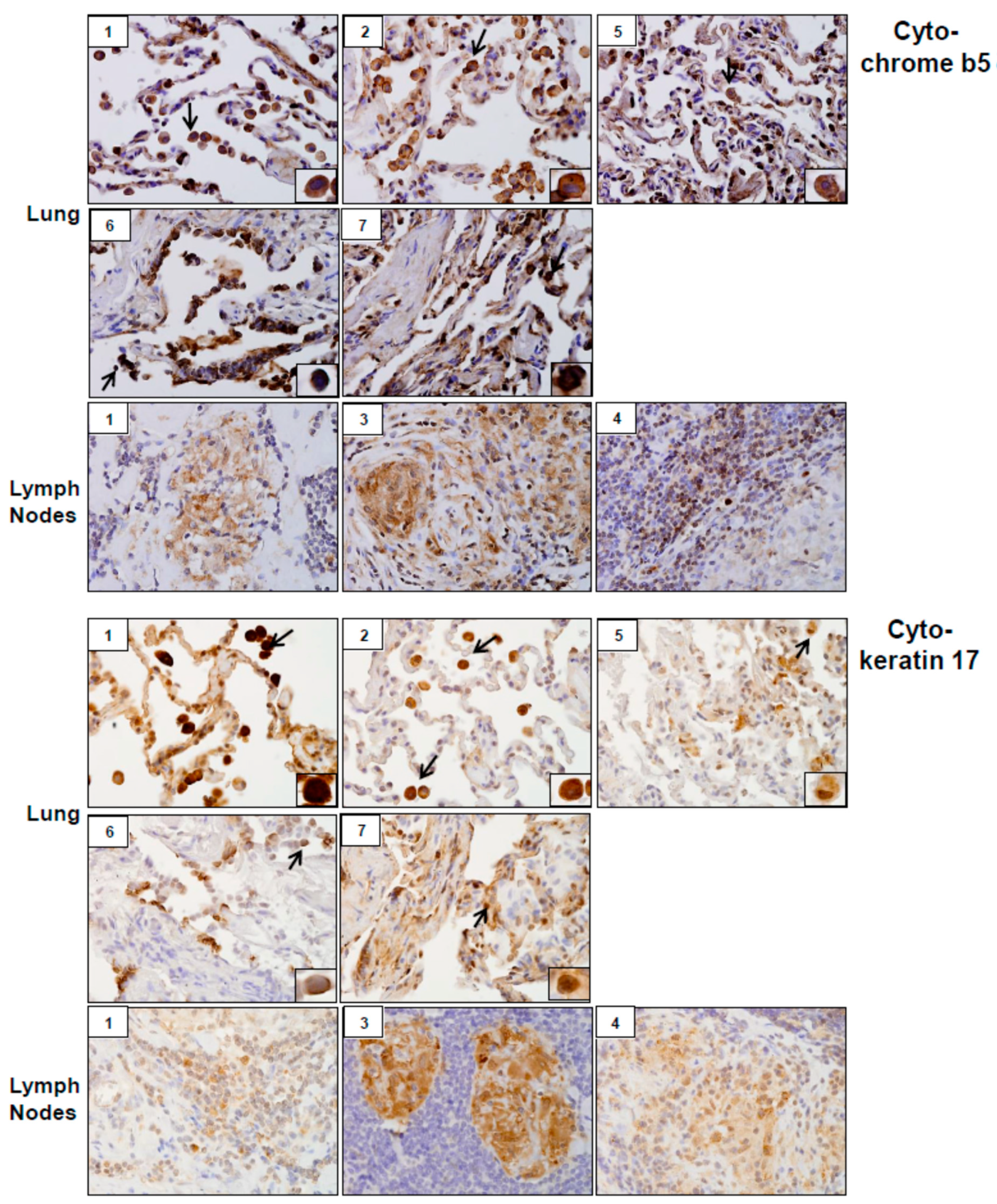
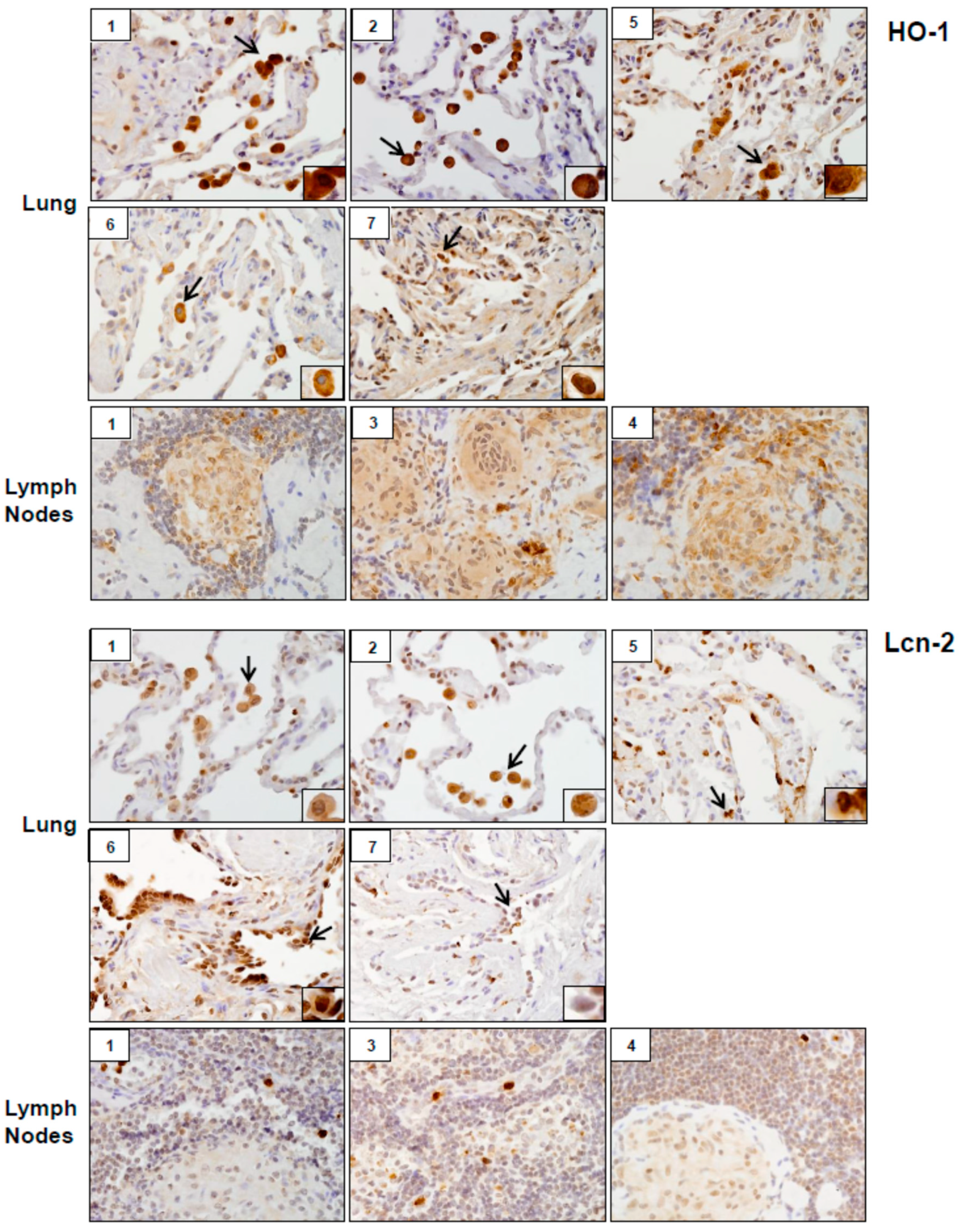
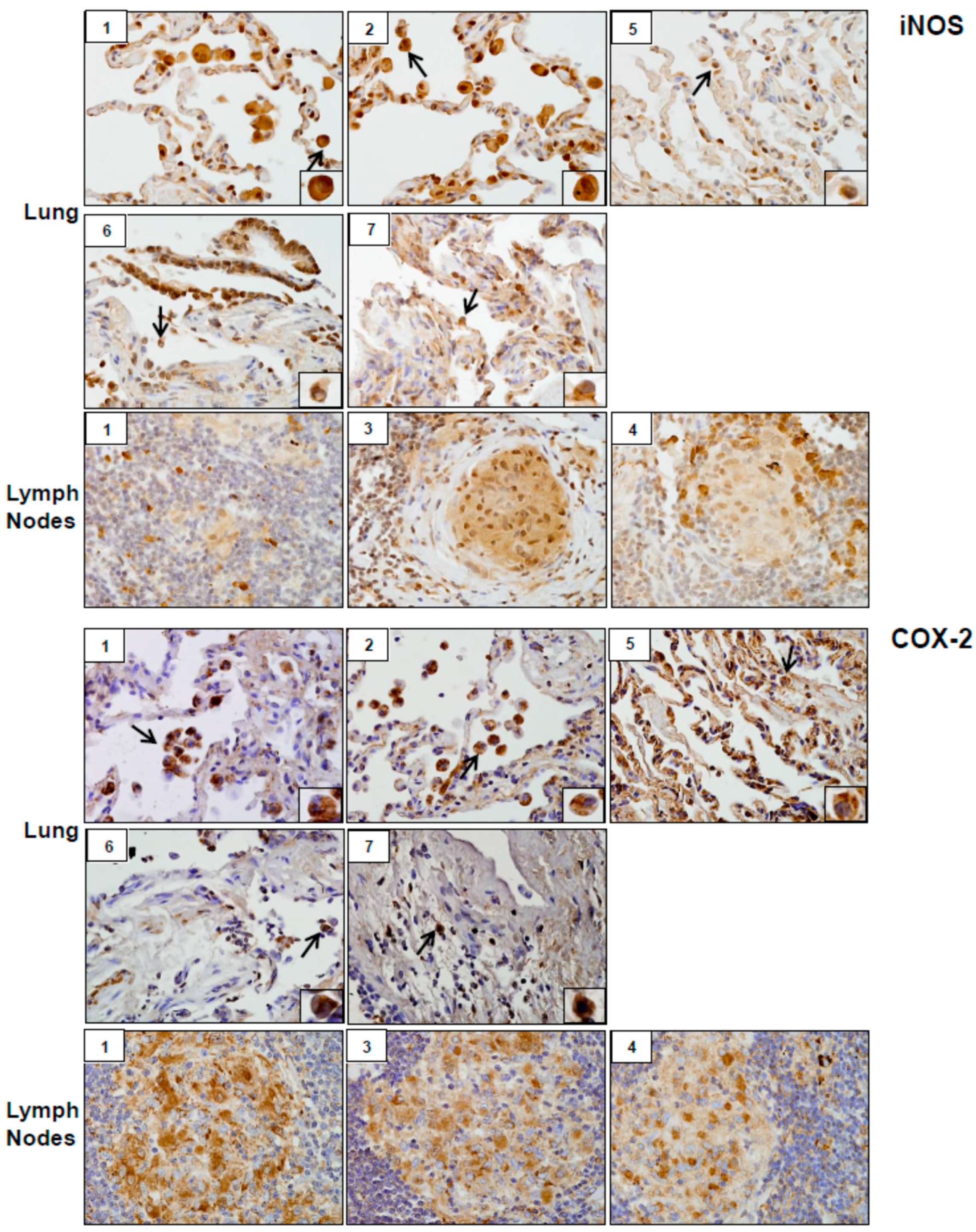
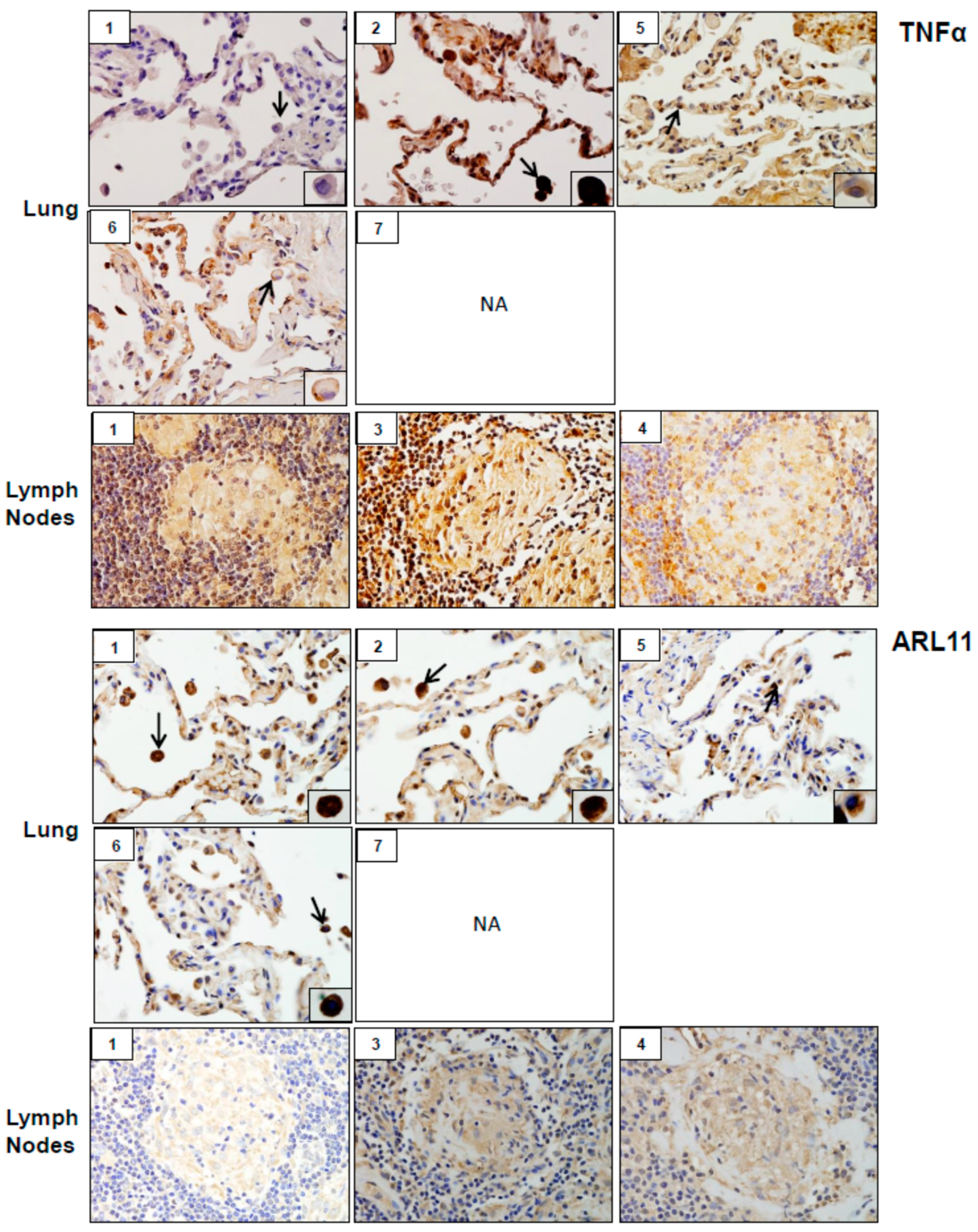
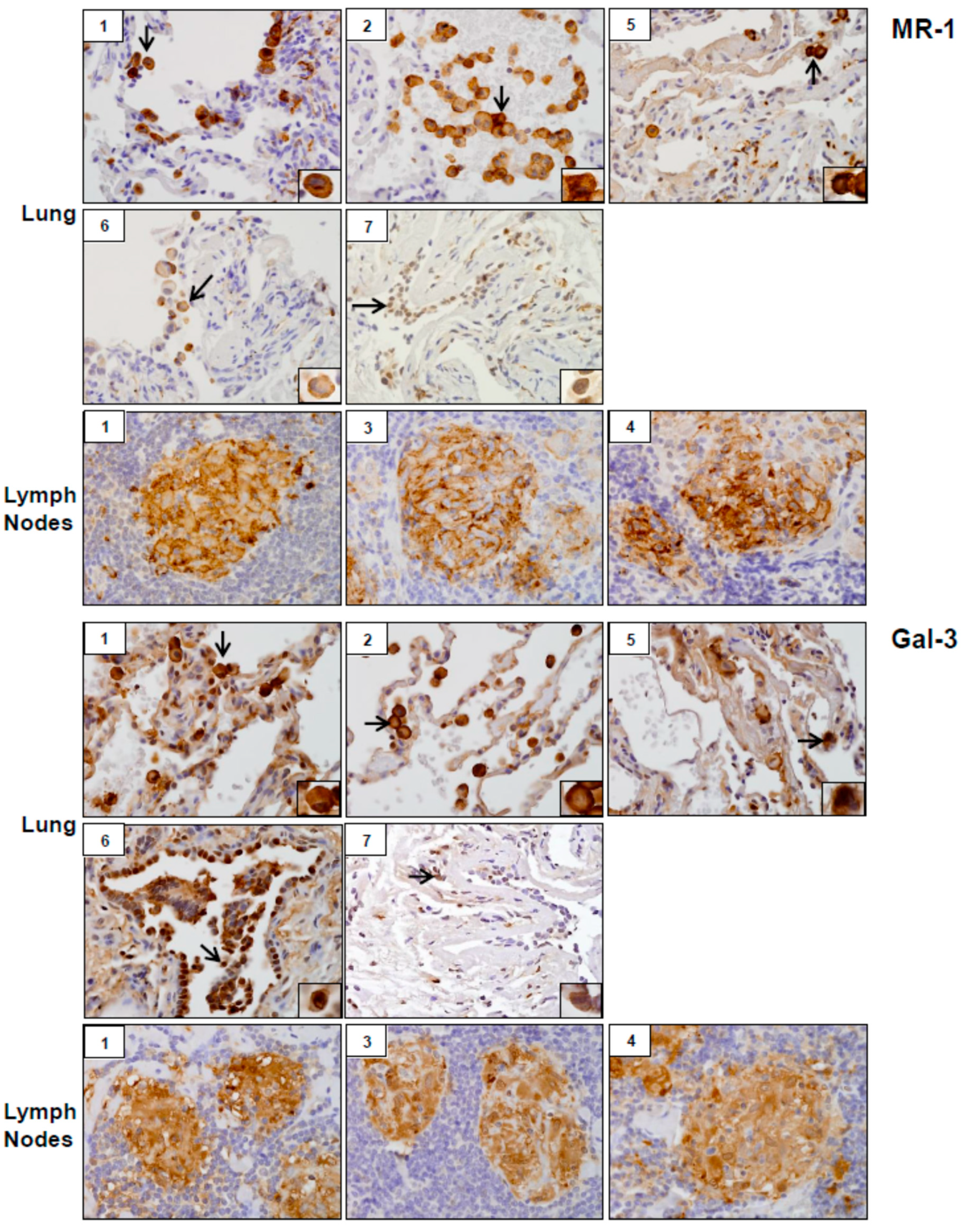
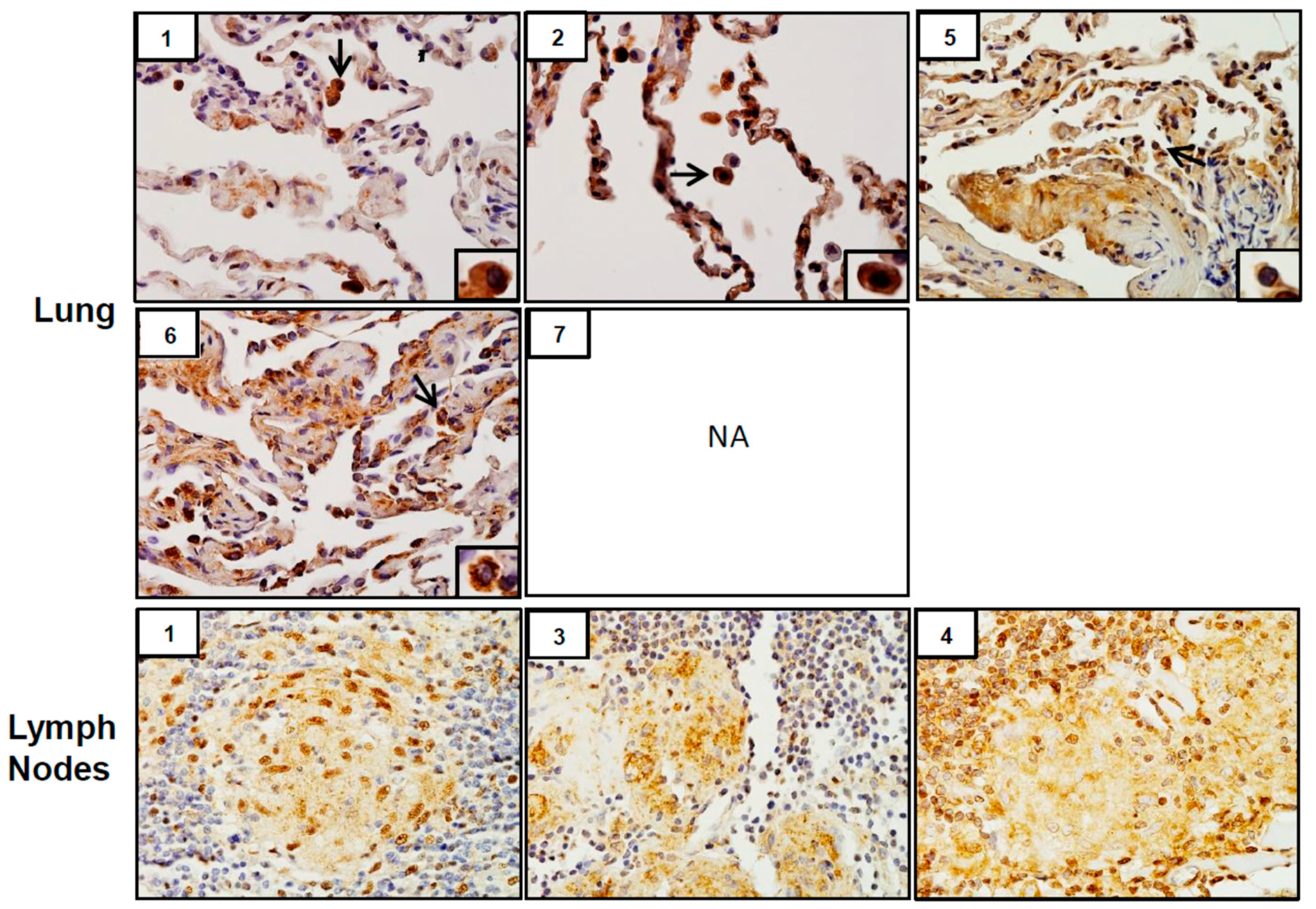
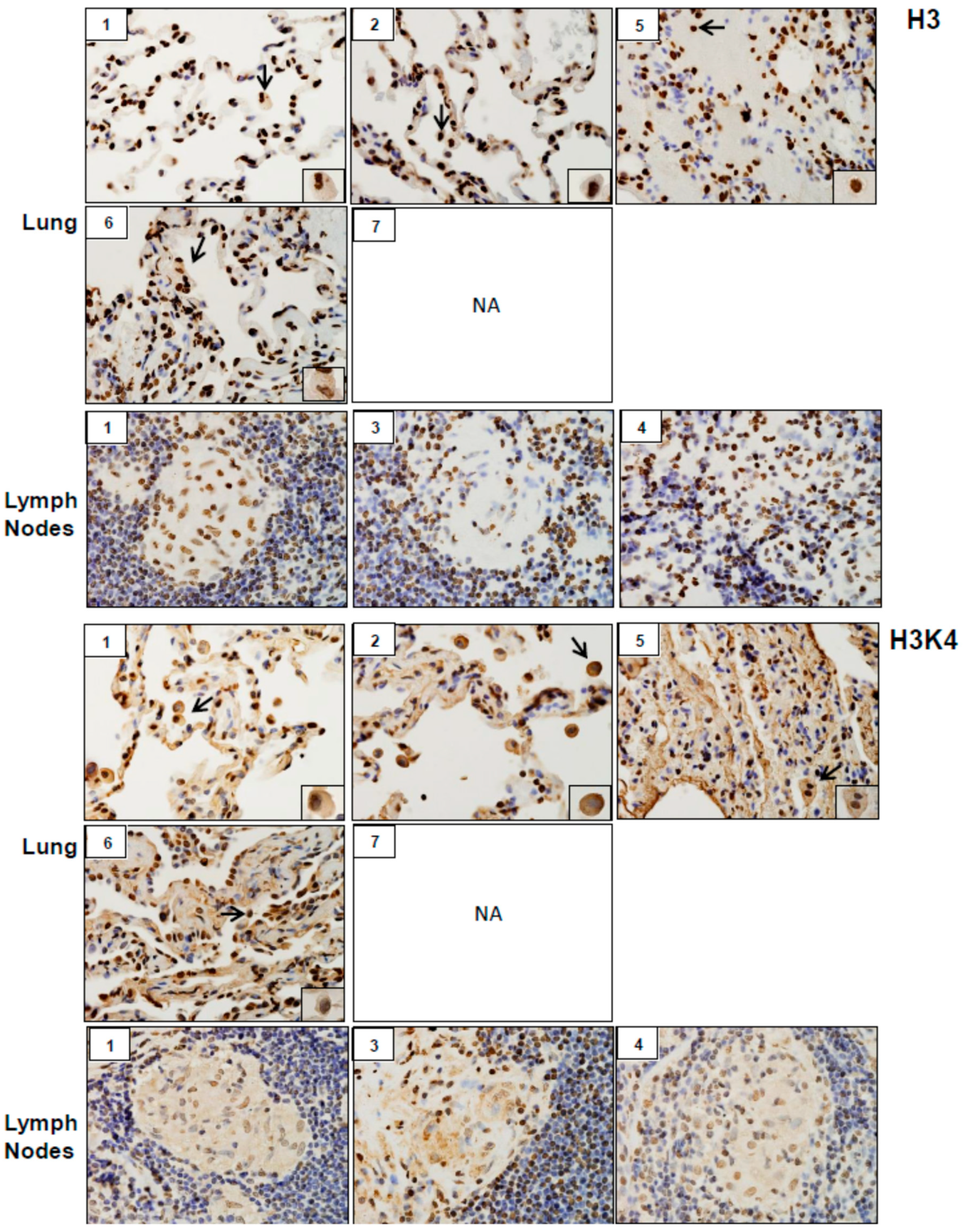
3.3. Expression of Markers of Injury, Oxidative Stress, Inflammation, Fibrosis, and Epigenetic Changes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Guidotti, T.L.; Prezant, D.; de la Hoz, R.E.; Miller, A. The evolving spectrum of pulmonary disease in responders to the World Trade Center tragedy. Am. J. Ind. Med. 2011, 54, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Wisnivesky, J.P.; Teitelbaum, S.L.; Todd, A.C.; Boffetta, P.; Crane, M.; Crowley, L.; de la Hoz, R.E.; Dellenbaugh, C.; Harrison, D.; Herbert, R.; et al. Persistence of multiple illnesses in World Trade Center rescue and recovery workers: A cohort study. Lancet 2011, 378, 888–897. [Google Scholar] [CrossRef]
- Webber, M.P.; Yip, J.; Zeig-Owens, R.; Moir, W.; Ungprasert, P.; Crowson, C.S.; Hall, C.B.; Jaber, N.; Weiden, M.D.; Matteson, E.L.; et al. Post-9/11 sarcoidosis in WTC-exposed firefighters and emergency medical service workers. Respir. Med. 2017, 132, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Lioy, P.J.; Weisel, C.P.; Millette, J.R.; Eisenreich, S.; Vallero, D.; Offenberg, J.; Buckley, B.; Turpin, B.; Zhong, M.; Cohen, M.D.; et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ. Health Perspect. 2002, 110, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.D.; Vaughan, J.M.; Garrett, B.; Prophete, C.; Horton, L.; Sisco, M.; Kodavanti, U.P.; Ward, W.O.; Peltier, R.E.; Zelikoff, J.; et al. Acute high-level exposure to WTC particles alters expression of genes associated with oxidative stress and immune function in the lung. J. Immunotoxicol. 2015, 12, 140–153. [Google Scholar] [CrossRef] [PubMed]
- Sunil, V.R.; Vayas, K.N.; Fang, M.; Zarbl, H.; Massa, C.; Gow, A.J.; Cervelli, J.A.; Kipen, H.; Laumbach, R.J.; Lioy, P.J.; et al. World Trade Center (WTC) dust exposure in mice is associated with inflammation, oxidative stress and epigenetic changes in the lung. Exp. Mol. Pathol. 2017, 102, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Herbert, R.; Moline, J.; Skloot, G.; Metzger, K.; Baron, S.; Luft, B.; Markowitz, S.; Udasin, I.; Harrison, D.; Stein, D.; et al. The World Trade Center disaster and the health of workers: Five-year assessment of a unique medical screening program. Environ. Health Perspect. 2006, 114, 1853–1858. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowley, L.E.; Herbert, R.; Moline, J.M.; Wallenstein, S.; Shukla, G.; Schechter, C.; Skloot, G.S.; Udasin, I.; Luft, B.J.; Harrison, D.; et al. “Sarcoid like” granulomatous pulmonary disease in World Trade Center disaster responders. Am. J. Ind. Med. 2011, 54, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Izbicki, G.; Chavko, R.; Banauch, G.I.; Weiden, M.D.; Berger, K.I.; Aldrich, T.K.; Hall, C.; Kelly, K.J.; Prezant, D.J. World Trade Center “sarcoid-like” granulomatous pulmonary disease in New York City Fire Department rescue workers. Chest 2007, 131, 1414–1423. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.S.; Song, Z.; Willett, M.H.; Heine, S.; Yung, R.C.; Liu, M.C.; Groshong, S.D.; Zhang, Y.; Tuder, R.M.; Moller, D.R. Serum amyloid A regulates granulomatous inflammation in sarcoidosis through Toll-like receptor-2. Am. J. Respir. Crit. Care Med. 2010, 181, 360–373. [Google Scholar] [CrossRef] [PubMed]
- Facco, M.; Cabrelle, A.; Calabrese, F.; Teramo, A.; Cinetto, F.; Carraro, S.; Martini, V.; Calzetti, F.; Tamassia, N.; Cassatella, M.A.; et al. TL1A/DR3 axis involvement in the inflammatory cytokine network during pulmonary sarcoidosis. Clin. Mol. Allergy 2015, 13, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hena, K.M.; Yip, J.; Jaber, N.; Goldfarb, D.; Fullam, K.; Cleven, K.; Moir, W.; Zeig-Owens, R.; Webber, M.P.; Spevack, D.M.; et al. Clinical Course of Sarcoidosis in World Trade Center-Exposed Firefighters. Chest 2018, 153, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Schnerch, J.; Prasse, A.; Vlachakis, D.; Schuchardt, K.L.; Pechkovsky, D.V.; Goldmann, T.; Gaede, K.I.; Muller-Quernheim, J.; Zissel, G. Functional Toll-Like Receptor 9 Expression and CXCR3 Ligand Release in Pulmonary Sarcoidosis. Am. J. Respir. Cell Mol. Biol. 2016, 55, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Wiken, M.; Idali, F.; Al Hayja, M.A.; Grunewald, J.; Eklund, A.; Wahlstrom, J. No evidence of altered alveolar macrophage polarization, but reduced expression of TLR2, in bronchoalveolar lavage cells in sarcoidosis. Respir. Res. 2010, 11, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valeyre, D.; Prasse, A.; Nunes, H.; Uzunhan, Y.; Brillet, P.Y.; Muller-Quernheim, J. Sarcoidosis. Lancet 2014, 383, 1155–1167. [Google Scholar] [CrossRef]
- Safirstein, B.H.; Klukowicz, A.; Miller, R.; Teirstein, A. Granulomatous pneumonitis following exposure to the World Trade Center collapse. Chest 2003, 123, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Fubini, B.; Hubbard, A. Reactive oxygen species (ROS) and reactive nitrogen species (RNS) generation by silica in inflammation and fibrosis. Free Radic. Biol. Med. 2003, 34, 1507–1516. [Google Scholar] [CrossRef]
- Rimal, B.; Greenberg, A.K.; Rom, W.N. Basic pathogenetic mechanisms in silicosis: Current understanding. Curr. Opin. Pulm. Med. 2005, 11, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Valavanidis, A.; Vlachogianni, T.; Fiotakis, K.; Loridas, S. Pulmonary Oxidative Stress, Inflammation and Cancer: Respirable Particulate Matter, Fibrous Dusts and Ozone as Major Causes of Lung Carcinogenesis through Reactive Oxygen Species Mechanisms. Int. J. Environ. Res. Public Health 2013, 10, 3886–3907. [Google Scholar] [CrossRef] [PubMed]
- Laskin, D.L.; Sunil, V.R.; Gardner, C.R.; Laskin, J.D. Macrophages and tissue injury: Agents of defense or destruction? Ann. Rev. Pharmacol. Toxicol. 2011, 51, 267–288. [Google Scholar] [CrossRef] [PubMed]
- Platko, K.; Lebeau, P.; Austin, R.C. MAPping the kinase landscape of macrophage activation. J. Biol. Chem. 2018, 293, 9910–9911. [Google Scholar] [CrossRef] [PubMed]
- Sunil, V.R.; Francis, M.; Vayas, K.N.; Cervelli, J.A.; Choi, H.; Laskin, J.D.; Laskin, D.L. Regulation of ozone-induced lung inflammation and injury by the beta-galactoside-binding lectin galectin-3. Toxicol. Appl. Pharmacol. 2015, 284, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.K.; Lee, S.G.; Lee, J.Y.; Nam, H.Y.; Lee, W.K.; Lee, K.H.; Kim, H.J.; Lim, Y. Silica induces human cyclooxygenase-2 gene expression through the NF-kappaB signaling pathway. J. Environ. Pathol. Toxicol. Oncol. 2005, 24, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Christophi, G.P.; Caza, T.; Curtiss, C.; Gumber, D.; Massa, P.T.; Landas, S.K. Gene expression profiles in granuloma tissue reveal novel diagnostic markers in sarcoidosis. Exp. Mol. Pathol. 2014, 96, 393–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawasaki, H. A mechanistic review of silica-induced inhalation toxicity. Inhal. Toxicol. 2015, 27, 363–377. [Google Scholar] [CrossRef] [PubMed]
- Arya, S.B.; Kumar, G.; Kaur, H.; Kaur, A.; Tuli, A. ARL11 regulates lipopolysaccharide-stimulated macrophage activation by promoting mitogen-activated protein kinase (MAPK) signaling. J. Biol. Chem. 2018, 293, 9892–9909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guglani, L.; Gopal, R.; Rangel-Moreno, J.; Junecko, B.F.; Lin, Y.; Berger, T.; Mak, T.W.; Alcorn, J.F.; Randall, T.D.; Reinhart, T.A.; et al. Lipocalin 2 regulates inflammation during pulmonary mycobacterial infections. PLoS ONE 2012, 7, e50052. [Google Scholar] [CrossRef] [PubMed]
- Francis, M.; Groves, A.M.; Sun, R.; Cervelli, J.A.; Choi, H.; Laskin, J.D.; Laskin, D.L. Editor’s Highlight: CCR2 Regulates Inflammatory Cell Accumulation in the Lung and Tissue Injury following Ozone Exposure. Toxicol. Sci. 2017, 155, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Menoret, A.; Kumar, S.; Vella, A.T. Cytochrome b5 and cytokeratin 17 are biomarkers in bronchoalveolar fluid signifying onset of acute lung injury. PLoS ONE 2012, 7, e40184. [Google Scholar] [CrossRef] [PubMed]
- Laskin, D.L.; Malaviya, R.; Laskin, J.D. Role of Macrophages in Acute Lung Injury and Chronic Fibrosis Induced by Pulmonary Toxicants. Toxicol. Sci. 2018. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Atochina-Vasserman, E.; Abramova, H.; George, B.; Manoj, V.; Scott, P.; Gow, A. Role of NOS2 in pulmonary injury and repair in response to bleomycin. Free Radic. Biol. Med. 2016, 91, 293–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; He, C.H.; Yang, D.S.; Nguyen, T.; Cao, Y.; Kamle, S.; Lee, C.M.; Gochuico, B.R.; Gahl, W.A.; Shea, B.S.; et al. Galectin-3 Interacts with the CHI3L1 Axis and Contributes to Hermansky-Pudlak Syndrome Lung Disease. J. Immunol. 2018, 200, 2140–2153. [Google Scholar] [CrossRef] [PubMed]
- Bonham, C.A.; Strek, M.E.; Patterson, K.C. From granuloma to fibrosis: Sarcoidosis associated pulmonary fibrosis. Curr. Opin. Pulm. Med. 2016, 22, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Patterson, K.C.; Strek, M.E. Pulmonary fibrosis in sarcoidosis. Clinical features and outcomes. Ann. Am. Thorac. Soc. 2013, 10, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Zissel, G.; Prasse, A.; Muller-Quernheim, J. Immunologic response of sarcoidosis. Semin. Respir. Crit. Care Med. 2010, 31, 390–403. [Google Scholar] [CrossRef]
- Hillerdal, G.; Nou, E.; Osterman, K.; Schmekel, B. Sarcoidosis: Epidemiology and prognosis. A 15-year European study. Am. Rev. Respir. Dis. 1984, 130, 29–32. [Google Scholar] [PubMed]
- Ungprasert, P.; Crowson, C.S.; Matteson, E.L. Smoking, obesity and risk of sarcoidosis: A population-based nested case-control study. Respir. Med. 2016, 120, 87–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchet, M.R.; Israel-Assayag, E.; Cormier, Y. Inhibitory effect of nicotine on experimental hypersensitivity pneumonitis in vivo and in vitro. Am. J. Respir. Crit. Care Med. 2004, 169, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, G.; Di Bona, D.; Belluzzo, F.; Macchia, L. Immunological and non-immunological mechanisms of allergic diseases in the elderly: Biological and clinical characteristics. Immun. Ageing 2017, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Martin-Romero, C.; Santos-Alvarez, J.; Goberna, R.; Sanchez-Margalet, V. Human leptin enhances activation and proliferation of human circulating T lymphocytes. Cell. Immunol. 2000, 199, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Mattoli, S.; Kleimberg, J.; Stacey, M.A.; Bellini, A.; Sun, G.; Marini, M. The role of CD8+ Th2 lymphocytes in the development of smoking-related lung damage. Biochem. Biophys. Res. Commun. 1997, 239, 146–149. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Number (%) | SGD Number (%) | Other Diseases Number (%) |
|---|---|---|---|
| Gender | |||
| Male | 7 (100) | 5 (100) | 2 (100) |
| Female | 0 (0) | 0 (0) | 0 (100) |
| Age | |||
| <50 | 4 (57) | 4 (80) | (0) |
| 50–59 | 1 (14) | 1 (20) | 0 (0) |
| 60–69 | 2 (29) | 0 (0) | 2 (100) |
| Race/Ethnicity | |||
| White (non-Hispanic) | 7 (100) | 5 (100) | 2 (100) |
| Black (non-Hispanic) | 0 (0) | 0 (0) | 0 (0) |
| Hispanic | 0 (0) | 0 (0) | 0 (0) |
| Smoking Status | |||
| Current | 0 (0) | 0 (0) | 0 (0) |
| Past | 4 (57) | 2 (40) | 2 (100) |
| Never | 3 (43) | 3 (60) | 0 (0) |
| BMI (kg/m2) | |||
| < 25 | 0 (0) | 0 (0) | 0 (0) |
| 25–29 | 3 (43) | 1 (20) | 2 (100) |
| 30–39 | 4 (57) | 4 (80) | 0 (0) |
| WTC Exposure Category [2] | |||
| Very High | 0 (0) | 0 (0) | 0 (0) |
| High | 3 (43) | 1 (20) | 2 (100) |
| Intermediate | 4 (57) | 4 (80) | 0 (0) |
| Low | 0 (0) | 0 (0) | 0 (0) |
| PT# | Reason for Referral | CT Impression | Biopsy | Lung Pathology | Lymph Node Pathology | Diagnosis |
|---|---|---|---|---|---|---|
| 1 | Lung nodules, mediastinal LAD | Mediastinal LAD, ground glass, sub-centimeter peripheral nodules, very mild fibrotic changes | VATS and Med | Bilateral upper lobe: Non-caseating granulomas with surrounding fibrosis | Non-caseating granulomas with surrounding fibrosis | SGD |
| 2 | Chronic cough and dyspnea | Multiple nodules | VATS | Right upper and lower lobe: Scant, poorly formed granulomas | NC | SGD |
| 3 | Hilar and mediastinal LAD and chronic bronchitis | Hilar and mediastinal LAD, apical pleural thickening | Med | NC | Non-caseating granulomas with surrounding fibrosis | SGD |
| 4 | Hilar LAD | Mediastinal and hilar LAD with bilateral pleural-based nodules | Med | NC | Non-caseating granuloma with surrounding fibrosis | SGD |
| 5 | Dyspnea and fatigue | Pulmonary nodules with mediastinal LAD | TBB | Right lower lobe: Focal areas of lung injury. (proteinaceous exudate with fibrin deposit) | NC | SGD (Diagnosed later at another medical facility) |
| 6 | Cough, dyspnea | Punctate calcified granulomas in lower lobes, bronchiectasis, mild intralobular septal thickening, scattered ground glass, mediastinal LAD | TBB | Left lower lobe: Focal interstitial fibrosis | NC | Pulmonary fibrosis and adenocarcinoma of the lung |
| 7 | Cough, dyspnea | Centrilobular emphysema, interstitial fibrosis. No adenopathy | TBB | Right upper lobe Unremarkable. | NC | Pulmonary fibrosis |
| PT# | Spirometry | Lung Volumes | DLCO (%) | Impression | |||
|---|---|---|---|---|---|---|---|
| FEV1 (%) | FVC (%) | FEV1/FVC (%) | VC (%) | TLC (%) | |||
| 1 | 98 | 100 | 97 | 98 | 93 | 103 | WNL |
| 2 | 100 | 104 | 96 | 103 | 109 | 104 | WNL |
| 3 | 88 | 84 | 104 | 81 | 82 | 85 | Mild RTLD |
| 4 | 98 | 94 | 104 | 83 | 73 | 69 | Mild RILD |
| 5 | 42 | 58 | 72 | 51 | 62 | 69 | Severe Mixed OLD & RILD |
| 6 | 98 | 87 | 112 | 80 | 78 | 57 | Mild RILD |
| 7 | 80 | 77 | 104 | 80 | 77 | 86 | Mild RTLD |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sunil, V.R.; Radbel, J.; Hussain, S.; Vayas, K.N.; Cervelli, J.; Deen, M.; Kipen, H.; Udasin, I.; Laumbach, R.; Sunderram, J.; et al. Sarcoid-Like Granulomatous Disease: Pathologic Case Series in World Trade Center Dust Exposed Rescue and Recovery Workers. Int. J. Environ. Res. Public Health 2019, 16, 815. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050815
Sunil VR, Radbel J, Hussain S, Vayas KN, Cervelli J, Deen M, Kipen H, Udasin I, Laumbach R, Sunderram J, et al. Sarcoid-Like Granulomatous Disease: Pathologic Case Series in World Trade Center Dust Exposed Rescue and Recovery Workers. International Journal of Environmental Research and Public Health. 2019; 16(5):815. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050815
Chicago/Turabian StyleSunil, Vasanthi R., Jared Radbel, Sabiha Hussain, Kinal N. Vayas, Jessica Cervelli, Malik Deen, Howard Kipen, Iris Udasin, Robert Laumbach, Jag Sunderram, and et al. 2019. "Sarcoid-Like Granulomatous Disease: Pathologic Case Series in World Trade Center Dust Exposed Rescue and Recovery Workers" International Journal of Environmental Research and Public Health 16, no. 5: 815. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050815