Qigong-Based Therapy for Treating Adults with Major Depressive Disorder: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Quantitative Data Synthesis and Analysis
3. Results
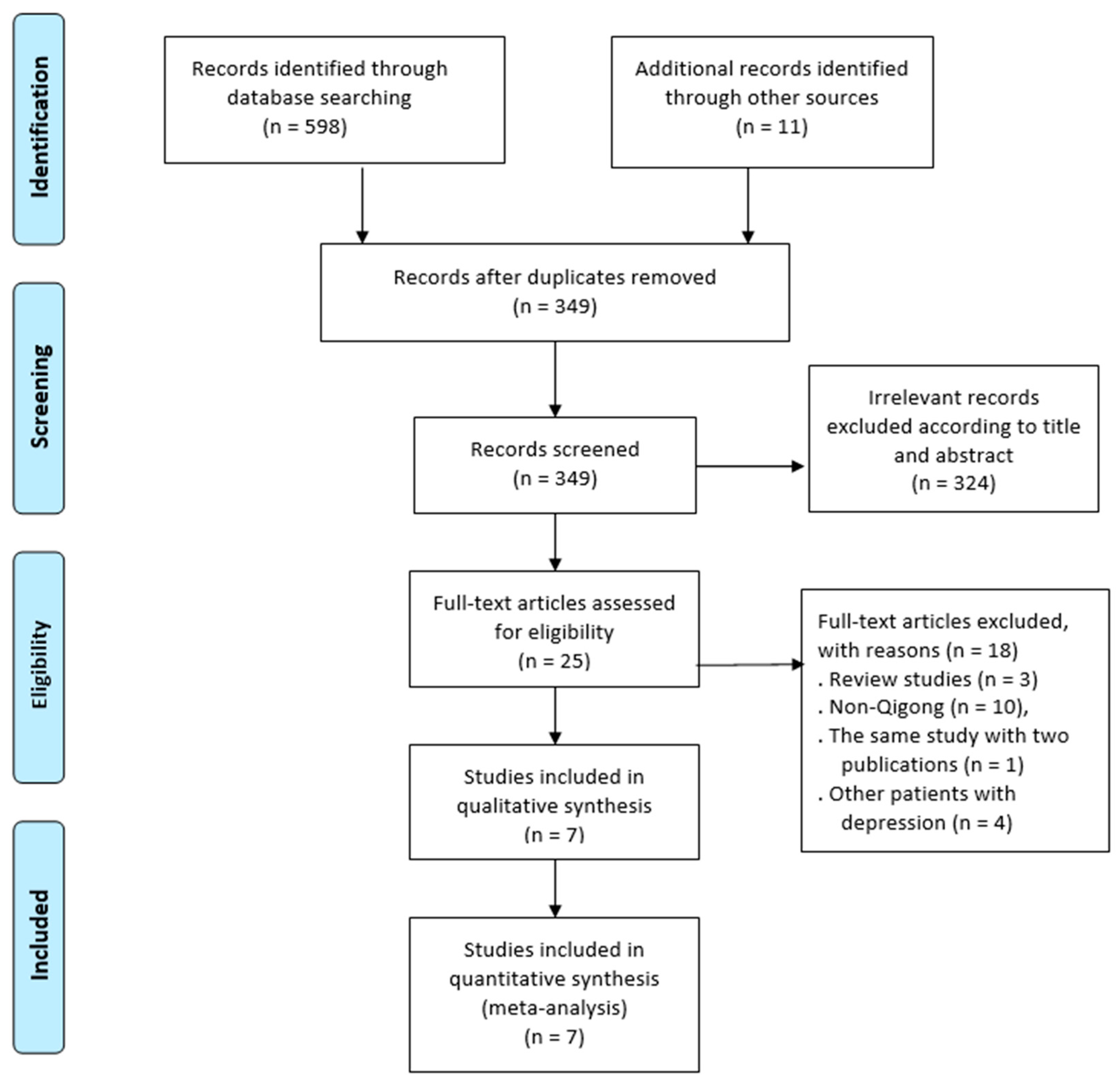
3.1. Study Selection and Characteristics
3.2. Quality Assessment
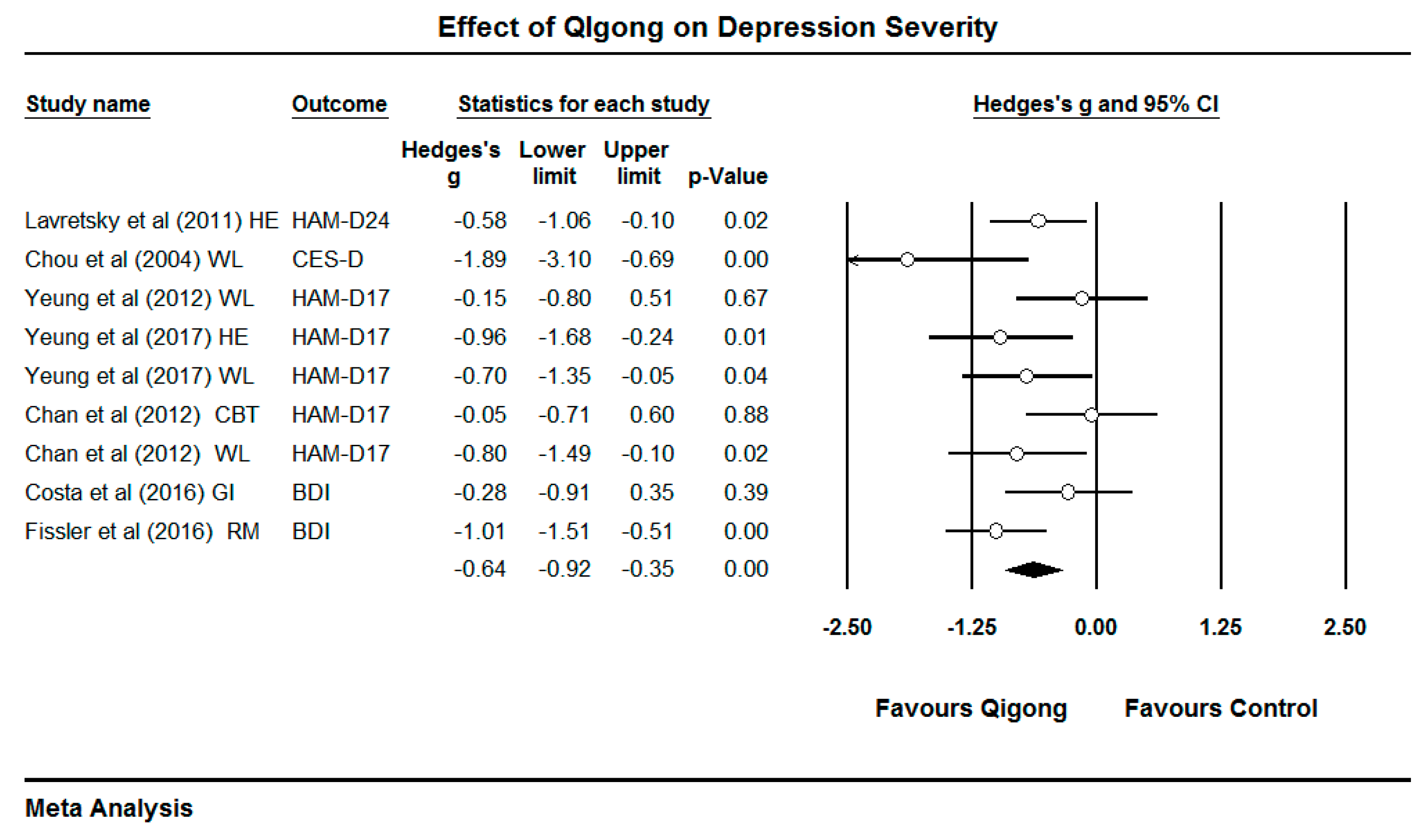
3.3. Effects of Qigong on Response Rate, Remission Rate, and Depression Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bentley, S.M.; Pagalilauan, G.L.; Simpson, S.A. Major Depression. Med. Clin. N. Am. 2014, 98, 981–1005. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depression: Let’s Talk Says WHO, as Depression Tops Lists of Causes of Ill Health. Available online: http://www.who.int/mediacentre/news/releases/2017/world-health-day/en/ (accessed on 20 January 2019).
- Kirsch, I.; Deacon, B.J.; Huedo-Medina, T.B.; Scoboria, A.; Moore, T.; Johnson, B. Initial severity and antidepressant benefits: A meta-analysis of data submitted to the Food and Drug Administration. PLoS Med. 2008, 5, e45. [Google Scholar] [CrossRef] [PubMed]
- Turner, E.H.; Matthews, A.M.; Linardatos, E. Selective publication of antidepressant trials and its influence on apparent efficacy. N. Engl. J. Med. 2008, 358, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Leichsenring, F.; Steinert, C.; Hoyer, J. Psychotherapy versus pharmacotherapy of depression: What’s the evidence? Z. Psychosom. Med. Psychother. 2016, 62, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Pigott, E.; Leventhal, M.; Alter, G.; Boren, J. Efficacy and effectiveness of antidepressants: Current status of research. Psychother. Psychosom. 2010, 79, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, C.; Hansen, L.; Simonsen, E.; Gluud, C. The effect of adding psychodynamic therapy to antidepressants in patients with major depressive disorder. A systematic review of randomized clinical trials with meta-analyses and trial sequential analyses. J. Affect. Disord. 2012, 137, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, J.C.; Hansen, J.L.; Storebø, O.J.; Simonsen, E.; Gluud, C. The effects of cognitive therapy versus ‘no intervention’ for major depressive disorder. PLoS ONE 2011, 6, e28299. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.X.; Chen, K.W.; Kinser, P.A.; Chan, J.; Ren, Z. Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin exercise for stroke rehabilitation: A systematic review with meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 600. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Hui, S.; Hu, X.; Chan, J.; Wang, C.; Boyden, S.; Sun, L.; Wang, H. Mindfulness-based Baduanjin exercise for depression and anxiety in people with physical or mental illnesses: A systematic review and meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Boyden, S.D.; Wang, H. A systematic review and meta-analysis of mindfulness-based (Baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Cui, Y.; Li, T. Effect of Health-Qigong on spinal mobility and disease activity in people with ankylosing spondylitis. Trav. Hum. 2017, 80, 1585–1597. [Google Scholar]
- Zou, L.; Pan, Z.; Yeung, A.; Talwar, S.; Wang, C.; Liu, Y.; Shu, Y.; Chen, X.; Thomas, G.A. A review study on the beneficial effects of Baduanjin. J. Altern. Complment. Med. 2017, 24, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.J.; Chen, K.W. Chinese Medical Qigong (College Textbook); Singing Dragon: London, UK; Philadelphia, PA, USA, 2010. [Google Scholar]
- Zou, L.; Zhang, Y.J.; Liu, Y.; Tian, X.P.; Xiao, T.; Liu, X.L.; Yeung, A.; Liu, J.; Wang, W.Q.; Yang, Q. The Effects of Tai Chi Chuan Versus Core Stability Training on Lower-Limb Neuromuscular Function in Aging Individuals with Non-Specific Chronic Lower Back Pain. Medicina 2019, 55, 60. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Yu, D. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trials Degener. Dis. 2017, 2, 46–52. [Google Scholar]
- Zou, L.; Wang, C.; Tian, Z.; Wang, Z.; Shu, Y. Effect of Yang-Style Tai Chi on gait parameters and musculoskeletal flexibility in healthy Chinese older women. Sports 2017, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z. Tai chi for health benefits in patients with multiple sclerosis: A systematic review. PLOS ONE 2017, 12, e0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; SasaKi, J.; Wang, H. A systematic review and meta-analysis Baduanjin Qigong for health benefits: Randomized controlled trials. Evid. Based Cmplement. Alternat. Med. 2017, 2017, e4548706. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Han, J.; Tsang, W.; Yeung, A.; Hui, S.S.; Tsang, W.W.N.; Ren, Z.; Wang, L. Effects of Tai Chi on lower limb proprioception in adults aged over 55: A systematic review ad meta-analysis. Arch. Phys. Med. Rehabil. 2018. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Li, T. Traditional Chinese exercise intervention improves symptoms in a patient with ankylosing spondylitis: A case study. Int. J. Adv. Res. 2017, 5, 888–895. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.; Zeng, N.; Wang, C.; Sun, L. A Systematic Review with Meta-Analysis of Mindful Exercises on Rehabilitative Outcomes among post-stroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yeung, A.; Xiao, T.; Tian, X.; Kong, Z.; Zou, L.; Wang, X. Chen-Style Tai Chi for Individuals (Aged 50 Years Old or Above) with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 517. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xie, H.; Liu, M.; Wang, Z.; Zou, L.; Yeung, A.S.; Hui, S.-C.; Yang, Q. The Effects of Tai Chi on Heart Rate Variability in Older Chinese Individuals with Depression. Int. J. Environ. Res. Public Health 2018, 15, 2771. [Google Scholar] [CrossRef] [PubMed]
- Kachan, D.; Olano, H.; Tannenbaum, S.L.; Annane, D.W.; Mehta, A.; Arheart, K.L.; Fleming, L.E.; Yang, X.; McClure, L.A.; Lee, D.J. Prevalence of mindfulness practices in the US Workforce: National Health Interview Survey. Prev. Chronic. Dis. 2017, 14, 160034. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Chan, J.; Cheung, J.; Zou, L. Qigong and Tai-Chi for mood regulation. Focus Am. Psychiatr. Publ. 2018, 16, 40–47. [Google Scholar] [CrossRef]
- Taylor, E.; Taylor-Piliae, R. The effects of Tai Chi on physical and psychosocial function among persons with multiple sclerosis: A systematic review. Complement. Ther. Med. 2017, 31, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Kim, Y.; Chuang, W.; Lee, M.S. Tai Chi for disease activity and flexibility in patients with ankylosing spondylitis—A controlled clinical trial. Evid. Based Cmplement. Alternat. Med. 2008, 5, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Pittler, M.; Shin, B.; Ernst, E. Tai Chi for osteoporosis: A systematic review. Osteoporos. Int. 2008, 19, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Bai, Z.; Guan, Z.; Fan, Y.; Liu, C.; Yang, K.; Ma, B.; Wu, B. The effects of Qigong for adults with chronic pain: Systematic review and meta-analysis. Am. J. Chin. Med. 2015, 43, 1525–1539. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.; Choic, S.; Inamor, A.; Rosenthal, D.; Yeung, A. Effects of Qigong on depression: A systematic review. Evid. Based Complement. Alternat. Med. 2013, 2013, e134737. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.; Lavretsky, H. Tai Chi and Qigong for the treatment and prevention of mental disorders. Psychiatric. Clin. N. Am. 2013, 36, 109–119. [Google Scholar]
- Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.-C. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Ho, R.; Chung, K.; Chong, W.; Yao, T.; Ng, S.; Chan, C. Qigong exercise alleviates fatigue, anxiety, and depressive symptoms, improves sleep quality, and shortens sleep latency in persons with chronic fatigue syndrome-like illness. Evid. Based Complement. Alternat. Med. 2014, 2014, e106048. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.; PRISMA-Group. Preferred Reporting Items for Systematic Review and Meta-Analysis protocols (PRISMA) 2015 statement. PLoS Med. 2009, 6, e1000097. [Google Scholar]
- Zhang, Y.; Li, C.; Zou, L.; Liu, X.; Song, W. The Effects of Mind-Body Exercise on Cognitive Performance in Elderly: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 2791. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.; Hopker, S. The effectiveness of exercise as an intervention in the management of depression: A systematic review and meta-regression analysis of randomized controlled trials. BMJ 2001, 322, 763. [Google Scholar] [CrossRef]
- Tsang, H.; Chan, E.; Cheung, W. Effects of mindful and non-mindful exercises on people with depression: A systematic review. Br. J. Clin. Psychol. 2008, 47, 302–322. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, C.; Hahn, S.; Torgerson, D.J.; Waston, J.; Bland, J.M. Adequacy and reporting of allocation concealment: Review of recent trials published in four general medical journals. BMJ 2005, 330, 1057–1058. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Feng, R.; Kim, D.; Wayne, P.; Yeh, G.; Baer, L.; Lee, O.; Denninger, J.; Fricchione, G.; Alpert, J.; Fava, M. A pilot, randomized controlled study of Tai Chi with passive and active controls in the treatment of depressed Chinese Americans. J. Clin. Psychiatry 2017, 78, e522–e528. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Wong, Q.; Sze, S. A Chinese Chan-based mind-body intervention for patients with depression. J. Affect. Disord. 2012, 142, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.B. A structured interview guide for the Hamilton Depression Rating Scale. Arch. Gener. Psychiatry 1988, 45, 742–747. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, A.; Lepoutre, V.; Wayne, P.; Yeh, G.; Slipp, L.; Fava, M.; Denninger, J.; Benson, H.; Fricchione, G. Tai Chi treatment for depression in Chinese Americans: A pilot study. Am. J. Phys. Med. Rehabil. 2012, 91, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Lavretsky, H.; Alstein, L.; Ercoli, O.; RIparetti-Brown, M.; Cyr, N.; Irwin, M. Complementary use of Tai Chi Chih augments escitalopram treatment of geriatric depression: A randomized controlled trial. Am. J. Geriatr. Psychiatry 2011, 19, 839–850. [Google Scholar] [CrossRef] [PubMed]
- Chou, K.; Lee, P.; Yu, E.; Macfarlane, D.; Cheng, Y.; Chan, S.; Chi, I. Effect of Tai Chi on depressive symptoms amongst Chinese older patients with depressive disorders: A randomized clinical trial. Int. J. Geriatr. Psychiatry 2004, 19, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.; Barnhofer, T. Turning towards or turning away: A comparison of mindfulness meditation and guided imagery relaxation in patients with acute depression. Behav. Cognit. Psychother. 2016, 44, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Fissler, M.; Winnebeck, E.; Schroeter, T.; Gummersbach, M.; Huntenburg, J.; Gaertner, M.; Barnhofer, T. An investigation of the effects of brief mindfulness training on self-reported interoceptive awareness, the ability to decenter, and their role in the reduction of depressive symptoms. Mindfulness 2016, 7, 1170–1181. [Google Scholar] [CrossRef]
- Matos, L.; Sousa, C.; Gonçalves, M. Qigong as a traditional vegetative biofeedback therapy: Long-term conditioning of physiological mind-body effects. BioMed Res. Int. 2015, 2015, e531789. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Characteristics of Participants | Intervention Protocol | Outcome Measured | Study Quality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patients Diagnostic Criteria, % of MDD, Study Location | Total Sample Size (DR), Female (%), Predominant Ethnicity | Age: Mean (SD) | Training Prescription | Total Training Min | Grp or Ind | Co-intervention | Outcomes (Instrument) | Concealed Allocation | Intention to Treat Analysis | Blinded | |
| Yeung et al. (2017) [41] | DSM-IV (psychiatrist), 100% of MDD, USA | 67 (25.3%), 72% female, 100% Chinese Americans | 54 (13) | Q: 2 × 60 min/week, 12 weeks (12 weeks follow-up) (Tai Chi); C1: 2 × 60 min/week (health education); C2: wait-list | 1440 | Grp | None | Remission rate, response rate, depression severity (HAM-D17 and BDI) | No | Yes | No |
| Chan et al. (2012) [42] | DSM-IV-TR (psychiatrist), 100% of MDD, China (HK) | 75 (33.3%), 80% female, 100% Chinese | Q: 47.1 (9.5) C1: 46.9 (6.5) C2: 45.4 (8.3) | Q:1 × 90 min/week 10 weeks (Shaolin movement Qigong); C1: 1 x× 90 min/week (CBT); C2: wait-list | 900 | Grp | Antidepressants | Depression severity (HAM-D17 and BDI) | Yes | No | Yes |
| Yeung et al. (2012) [45] | DSM-IV (psychiatrist), 100% of MDD, USA | 39 (5.1%), 77% female, 100% Chinese Americans | 55(10) | Q: 2 × 60 min/week, 12 weeks (Tai Chi); C: wait-list | 1440 | Grp | Antidepressants allowed | Remission rate, response rate, depression severity (HAM-D17) | Yes | Yes | Yes |
| Lavretsky et al. (2011) [46] | DSM-IV (psychiatrist), 100% of MDD, USA | 73 (6.8%), 61.6% female, 74% Caucasians and 11% African-Americans | Q: 69.1 (7.0) C: 72.0 (7.4) | Q: 1 × 120 min/week, 10 weeks (Tai Chi); C: 1 × 120 min/week (health education) | 1200 | Grp | Escitalopram/lorazepam: 10–20 mg/day | Depression severity (HAM-D24) | Yes | Yes | Yes |
| Chou et al. (2004) [47] | DSM-IV (psychiatrist), 90% of MDD, China (HK) | 14 (0%), 50% female, 100% Chinese | 72.6 (4.2) | Q: 3 × 45 min/week, 12 weeks (Tai Chi); C: wait-list | 1620 | Grp | Antidepressants or psychotherapy | Depression severity (CES-D) | No | Yes | Yes |
| Costa et al. (2016) [48] | DSM-IV (psychiatrist), 100% of MDD, UK | 40 (7.5%), 74% female, 74% Caucasians and 16% African-Americans | Q: 39 (1.2) C: 38 (9.7) | Q: 1 × 60min/week (Grp) + 6 × 30 min/week (Ind), 1 week (static Qigong); C: same dosage/format (guided imagery) | 240 | Mixed | Antidepressants | Depression severity (BDI) | Yes | No | No |
| Fissler et al. (2016) [49] | DSM-IV (a psychiatrist), 100% of MDD, Germany | 74 (8.1%), 56% female, 100% Caucasians | 42 (12.5) | Q: 7 × 50 min/week, 2 weeks (Static Qigong); C: 7 × 50 min/week (rest and music) | 700 | Grp | Antidepressants | Depression severity (BDI) | Yes | No | No |
| Categorical Moderator | Outcome | Level | No. of Studies/ Comparisons | Hedges’ g | 95% CI | I2 % | Test for Between-Group Homogeneity | ||
|---|---|---|---|---|---|---|---|---|---|
| Q-Value | df (Q) | p-Value | |||||||
| Control Type | Depression | Active | 4 | −0.47 | −0.81 to −0.12 | 22.75% | 1.41 | 1 | 0.23 |
| Passive | 5 | −0.80 | −1.23 to −0.37 | 48.07% | |||||
| Qigong Type | Depression | Movement | 7 | −0.62 | −0.96 to −0.28 | 41.62% | 0.02 | 1 | 0.9 |
| Static | 2 | −0.67 | −1.38 to 0.04 | 67.84% | |||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, L.; Kong, Z.; Zhang, Y. Qigong-Based Therapy for Treating Adults with Major Depressive Disorder: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 826. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050826
Guo L, Kong Z, Zhang Y. Qigong-Based Therapy for Treating Adults with Major Depressive Disorder: A Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2019; 16(5):826. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050826
Chicago/Turabian StyleGuo, Lijuan, Zhaowei Kong, and Yanjie Zhang. 2019. "Qigong-Based Therapy for Treating Adults with Major Depressive Disorder: A Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 16, no. 5: 826. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050826