Handgrip Strength is Associated with Psychological Functioning, Mood and Sleep in Women over 65 Years

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
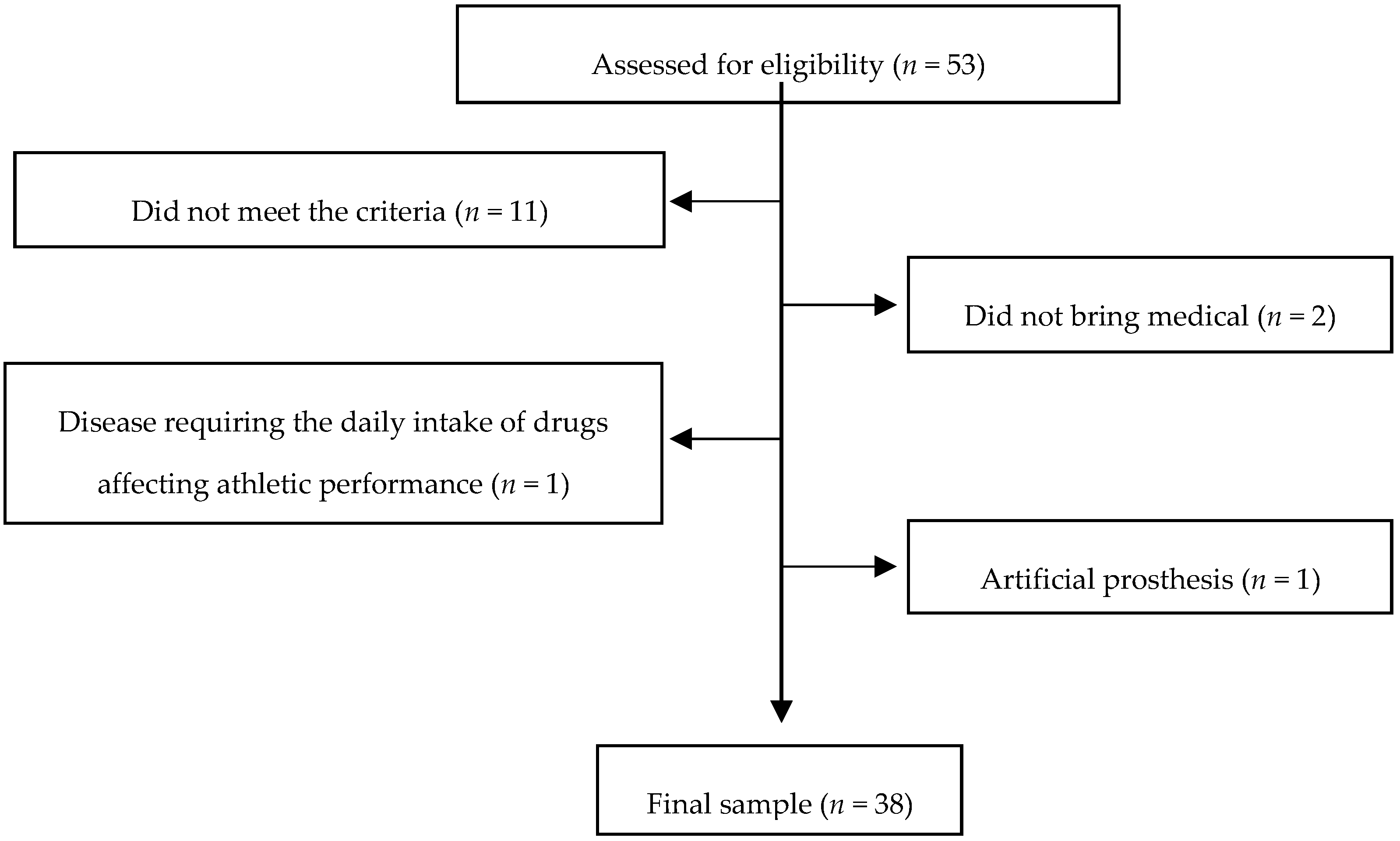
2.1. Participants
2.2. Materials and Instruments
2.3. Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- INE. Esperanza de Vida. Available online: http://www.ine.es/ss/Satellite?L=es_ES&c=INESeccion_C&cid=1259926380048&p=1254735110672&pagename=ProductosYServicios/PYSLayout (accessed on 4 February 2017).
- Pérez, M.; Eduardo, J.; Martínez, S.; Ignacio, F.; Perpiñán, A.; María, J. Esperanza de vida ajustada por la calidad en españa: Una aproximación quality-adjusted life expectancy in Spain: An estimate. J. Public. Progr. Policy Eval. 2016, 6, 28–48. [Google Scholar]
- Casas Herrero, A.; Izquierdo Redín, M. Ejercicio fisico como intervencion eficaz en el anciano fragil. An. Sist. Sanit. Navar. 2012, 35, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Chong Daniel, A. Aspectos biopsicosociales que inciden en la salud del adulto mayor. Rev. Cuba. Med. Gen. Integr. 2012, 28, 79–86. [Google Scholar]
- Lolbé, M.; Guzmán, B.; Flores Galaz, M.M. Construcción de Una Escala de Salud Mental Positiva para Adultos en Poblacion Mexicana Positive Mental Health, Construction of a Measurement Scale for Adults in Mexican Population, Rev Iberoam Diagnóstico y Evaluación—E Avaliação Psicológica; RIDEP: Lisbon, Portugal, 2015; Volume 1, pp. 22–23. [Google Scholar]
- Bonardi, J.M.T.; Lima, L.G.; Campos, G.O.; Bertani, R.F.; Moriguti, J.C.; Ferriolli, E.; Lima, N.K.C. Effect of different types of exercise on sleep quality of elderly subjects. Sleep Med. 2016, 25, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Eumann Mesas, A.; López-García, E.; Rodríguez-Artalejo, F. Sleep duration and functional limitations in older adult. Med. Clin. 2017, 136, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Kline, C.E.; Irish, L.A.; Krafty, R.T.; Sternfeld, B.; Kravitz, H.M.; Buysse, D.J.; Bromberger, J.T.; Dugan, S.A.; Hall, M.H. Consistently high sports/exercise activity is associated with better sleep quality, continuity and depth in midlife women: The SWAN Sleep Study. Sleep 2013, 36, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Annunziata, G.; Di Somma, C.; Laudisio, D.; Colao, A.; Savastano, S. Obesity and sleep disturbance: The chicken or the egg. Crit. Rev. Food Sci. Nutr. 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.P.R.; McNaughton, L.R.; Polman, R.C.J. Effects of sleep deprivation and exercise on cognitive, motor performance and mood. Physiol. Behav. 2006, 87, 396–408. [Google Scholar] [CrossRef] [PubMed]
- Bridle, C.; Spanjers, K.; Patel, S.; Atherton, N.M.; Lamb, S.E. Effect of exercise on depression severity in older people: Systematic review and meta-analysis of randomised controlled trials. Br. J. Psychiatry. 2012, 201, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, R. Neurobiology of Major Depressive Disorder. Neural Plast. 2013, 2013, e-873278, Hindawi Publishing Corporation. [Google Scholar] [CrossRef] [PubMed]
- Sher, L.; Oquendo, M.A.; Burke, A.K.; Cooper, T.B.; John Mann, J. Combined dexamethasone suppression–corticotrophin-releasing hormone stimulation test in medication-free major depression and healthy volunteers. J. Affect. Disord. 2013, 151, 1108–1112. [Google Scholar] [CrossRef] [PubMed]
- Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; García-Pinillos, F.; Latorre-Román, P.Á. Effects of a 10-week functional training programme on pain, mood state, depression, and sleep in healthy older adults. Psychogeriatrics 2018, 18, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Man, Q.; Li, L.; Song, P.; Jia, S.; Song, S.; Meng, L.; Zhang, J. Vitamin D receptor gene polymorphisms modify the association of serum 25-hydroxyvitamin D levels with handgrip strength in the elderly in Northern China. Nutrition 2019, 57, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Muscogiuri, G.; Di Somma, C.; Tramontano, G.; De Luca, V.; Illario, M.; Colao, A.; Savastano, S. Association between Mediterranean diet and hand grip strength in older adult women. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-Y.; Chen, L.-Y. Grip strength in older adults: Test-retest reliability and cutoff for subjective weakness of using the hands in heavy tasks. Arch. Phys. Med Rehabil. 2010, 91, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Kuh, D.; Cooper, C.; Gale, C.R.; Lawlor, D.A.; Matthews, F.; Hardy, R.; FALCon, HALCyon Study Teams. Objective measures of physical capability and subsequent health: A systematic review. Age Ageing 2011, 40, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Franke, W.D.; Margrett, J.A.; Heinz, M.; Martin, P. Handgrip strength, positive affect, and perceived health are prospectively associated with fewer functional limitations among centenarians. Aging Hum. Dev. 2012, 75, 351–363. [Google Scholar] [CrossRef] [PubMed]
- Taekema, D.G.; Gussekloo, J.; Maier, A.B.; Westendorp, R.G.J.; de Craen, A.J.M. Handgrip strength as a predictor of functional, psychological and social health. A prospective population-based study among the oldest old. Age Ageing 2010, 39, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukumori, N.; Yamamoto, Y.; Takegami, M.; Yamazaki, S.; Onishi, Y.; Sekiguchi, M.; Otani, K.; Konno, S.; Kikuchi, S.; Fukuhara, S. Association between hand-grip strength and depressive symptoms: Locomotive Syndrome and Health Outcomes in Aizu Cohort Study (LOHAS). Age Ageing 2015, 44, 592–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancilla Solorza, E.; Ramos, S.; Morales, P. Fuerza de prensión manual según edad, género y condición funcional en adultos mayores Chilenos entre 60 y 91 años. Rev. Med. Chil. 2016, 144, 598–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabañero-Martínez, M.J.; Cabrero-García, J.; Richart-Martínez, M.; Muñoz-Mendoza, C.L. The Spanish versions of the Barthel index (BI) and the Katz index (KI) of activities of daily living (ADL): A structured review. Arch. Gerontol. Geriatr. 2009, 49, e77–84. [Google Scholar] [CrossRef] [PubMed]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Profile of Mood State Manual; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Fuentes, I.; Balaguer, I.; Meliá, J.L.; García-Merita, M.L. Forma Abreviada del Perfil de los Estados de Ánimo (POMS). In Actas del V Congreso Nacional de Psicología de la Actividad Física y el Deporte; Universitat de València: Valencia, Spain, 1995; pp. 29–39. [Google Scholar]
- Sheikh, J.I.; Hill, R.D.; Yesavage, J.A. Long-term efficacy of cognitive training for age-associated memory impairment: A six-month follow-up study. Dev. Neuropsychol. 1986, 2, 413–421. [Google Scholar] [CrossRef]
- Martínez de La Iglesia, J.; Onís Vilches, M.; Dueñas Herrero, R.; Albert Colomer, C.; Aguado Taberné, C.; Luque Luque, R. Versión española del cuestionario de Yesavage abreviado (GDS) para el despistaje de depresión en mayores de 65 años: Adaptación y validación. Medifam 2002, 12, 26–40. [Google Scholar] [CrossRef]
- García, J.B.; G-Portilla, M.P.G.; Martínez, P.A.S.; Fernández, M.T.B.; Alvarez, C.I.; Domínguez, J.M.F. Propiedades psicométricas del cuestionario Oviedo de sueño. Psicothema 2000, 12, 107–112. [Google Scholar]
- Ruiz, J.R.; España-Romero, V.; Ortega, F.B.; Sjöström, M.; Castillo, M.J.; Gutierrez, A. Hand Span Influences Optimal Grip Span in Male and Female Teenagers. J. Hand. Surg. Am. 2006, 31, 1367–1372. [Google Scholar] [CrossRef] [PubMed]
- Guede Rojas, F.; Chirosa Ríos, L.J.; Vergara Ríos, C.; Fuentes Contreras, J.; Delgado Paredes, F.; Valderrama Campos, M.J. Fuerza prensil de mano y su asociación con la edad, género y dominancia de extremidad superior en adultos mayores autovalentes insertos en la comunidad: Un estudio exploratorio. Rev. Med. Chil. 2015, 143, 995–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buigues, C.; Padilla-Sánchez, C.; Garrido, J.F.; Navarro-Martínez, R.; Ruiz-Ros, V.; Cauli, O. The relationship between depression and frailty syndrome: A systematic review. Aging Ment. Health 2015, 19, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Latorre Román, P.A.; García-Pinillos, F.; Huertas Herrador, J.A.; Cózar Barba, M.; Muñoz Jiménez, M. Relacion entre sexo, Composicion corporal, Velocidad de la marcha y satisfaccion corporal en ancianos. Nutr. Hosp. 2014, 30, 851–857. [Google Scholar] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Ford, D.E.; Cooper-Patrick, L. Sleep disturbances and mood disorders: An epidemiologic perspective. Depress Anxiety 2001, 14, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Lino, V.T.S.; Rodrigues, N.C.P.; O’Dwyer, G.; Andrade, M.K.; de Noronha Andrade, M.K.; Mattos, I.E.; Portela, M.C. Handgrip Strength and Factors Associated in Poor Elderly Assisted at a Primary Care Unit in Rio de Janeiro, Brazil. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Kasagi, F.; Yamada, M.; Fujita, S. Grip Strength Predicts Cause-Specific Mortality in Middle-Aged and Elderly Persons. Am. J. Med. 2007, 120, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Al Snih, S.; Markides, K.S.; Ray, L.; Ostir, G.V.; Goodwin, J.S. Handgrip Strength and Mortality in Older Mexican Americans. J. Am. Geriatr. Soc. 2002, 50, 1250–1256. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
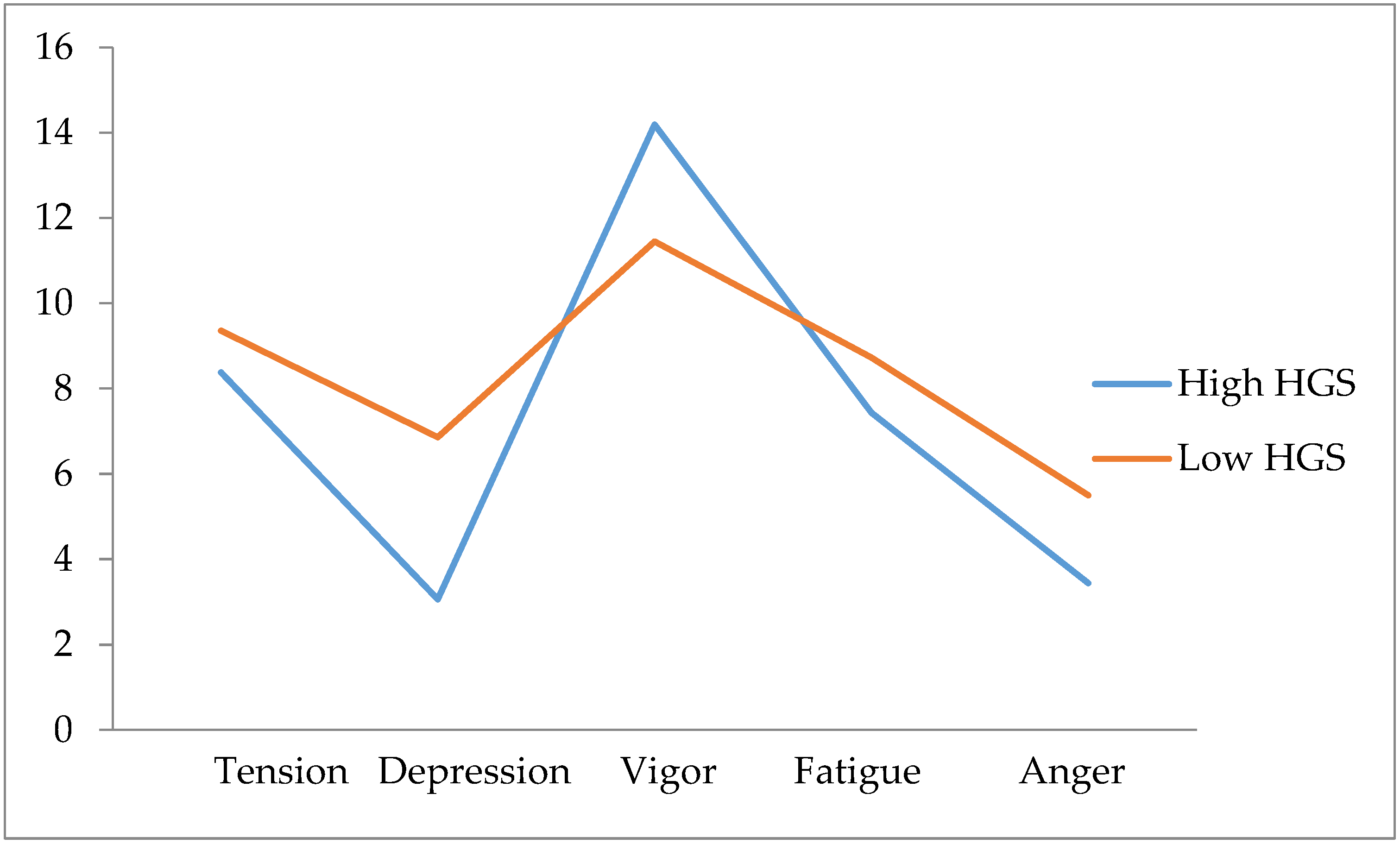
| High HGS Mean (SD) n = 16 | Low HGS Mean (SD) n = 22 | p-Valor | Partial Eta2 | |
|---|---|---|---|---|
| Age (years) | 71.00 (5.47) | 73.32 (4.89) | 0.157 | 0.055 |
| BMI (Kg/m2) | 30.98 (6.37) | 30.48 (5.28) | 0.791 | 0.002 |
| Handgrip strength (Kg) | 22.61 (2.89) | 13.21 (2.93) | <0.001 | 0.727 |
| Geriatric depression | 3.06 (2.72) | 4.23 (2.54) | 0.138 | 0.064 |
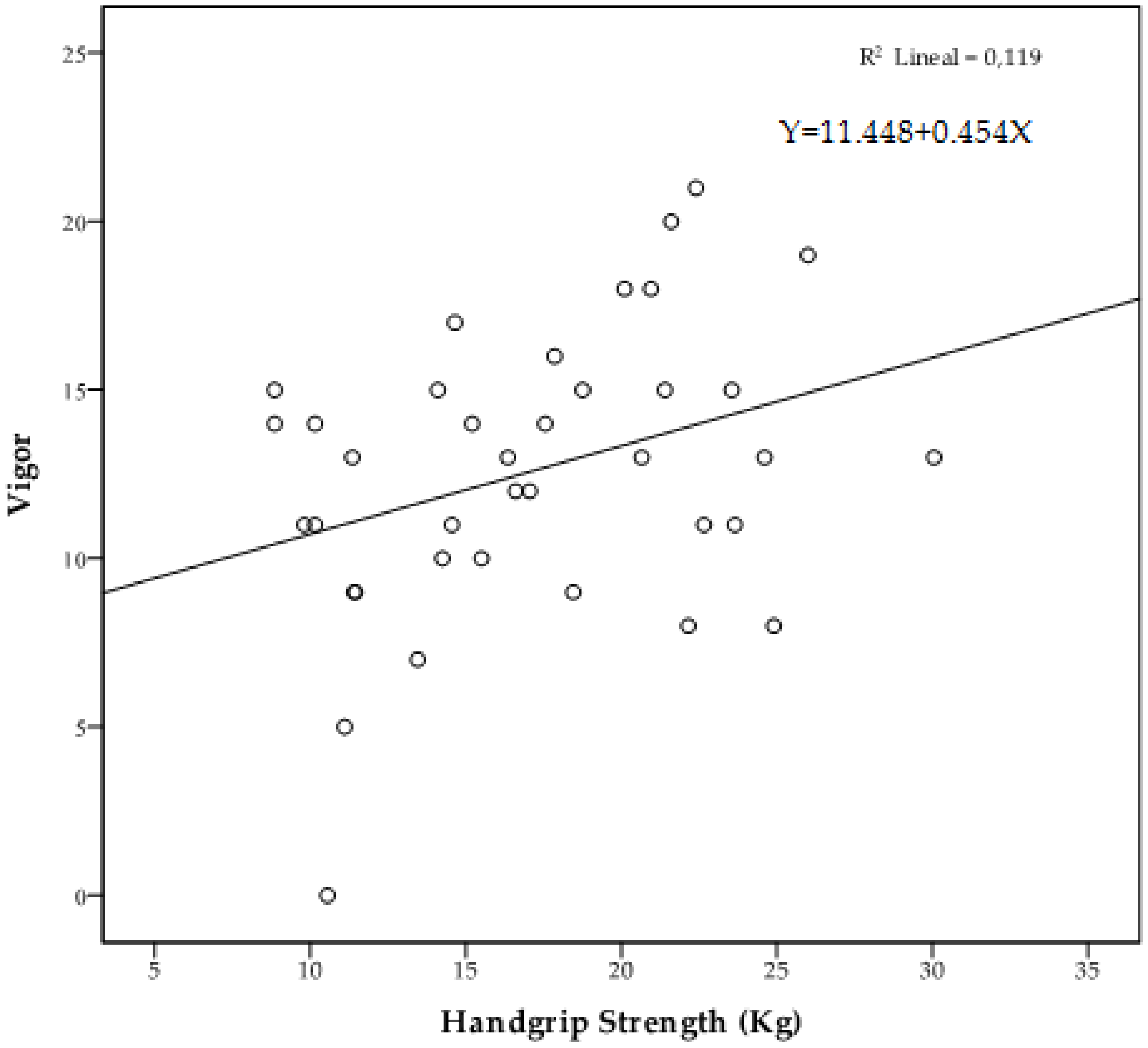
| Vigor | 14.19 (4.18) | 11.45 (3.88) | 0.050 | 0.105 |
| Anger | 3.44 (4.76) | 5.50 (4.72) | 0.202 | 0.048 |
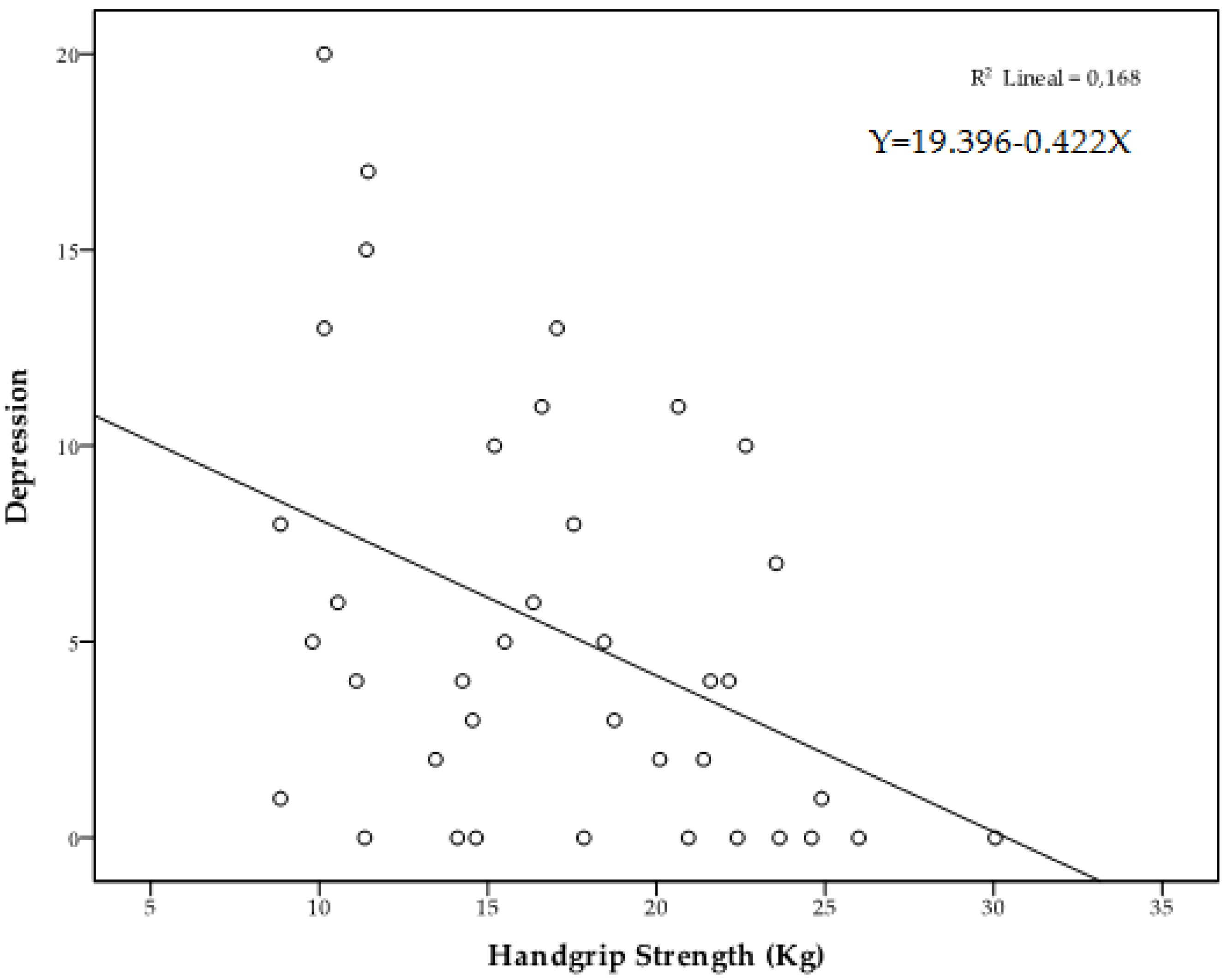
| Depression | 3.06 (3.60) | 6.86 (5.90) | 0.040 | 0.118 |
| Tension | 8.38 (3.68) | 9.36 (4.34) | 0.408 | 0.020 |
| Fatigue | 7.44 (5.39) | 8.73 (3.48) | 0.197 | 0.048 |
| Sleep satisfaction | 3.81 (1.37) | 3.82 (1.18) | 0.942 | <0.001 |
| Insomnia | 21.00 (4.89) | 26.18 (6.58) | 0.032 | 0.129 |
| Hypersomnia | 5.19 (1.94) | 5.27 (3.04) | 0.687 | 0.005 |
| Sleep total score | 30.00 (5.46) | 35.27 (7.70) | 0.045 | 0.113 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; García-Pinillos, F.; Latorre-Román, P.Á. Handgrip Strength is Associated with Psychological Functioning, Mood and Sleep in Women over 65 Years. Int. J. Environ. Res. Public Health 2019, 16, 873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050873
Laredo-Aguilera JA, Carmona-Torres JM, Cobo-Cuenca AI, García-Pinillos F, Latorre-Román PÁ. Handgrip Strength is Associated with Psychological Functioning, Mood and Sleep in Women over 65 Years. International Journal of Environmental Research and Public Health. 2019; 16(5):873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050873
Chicago/Turabian StyleLaredo-Aguilera, José Alberto, Juan Manuel Carmona-Torres, Ana Isabel Cobo-Cuenca, Felipe García-Pinillos, and Pedro Ángel Latorre-Román. 2019. "Handgrip Strength is Associated with Psychological Functioning, Mood and Sleep in Women over 65 Years" International Journal of Environmental Research and Public Health 16, no. 5: 873. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050873