Visualising Combined Time Use Patterns of Children’s Activities and Their Association with Weight Status and Neighbourhood Context

 ,
,  , ,
, ,  , , and
, , and
Abstract
:
1. Introduction
Aims and Rationale
2. Methods
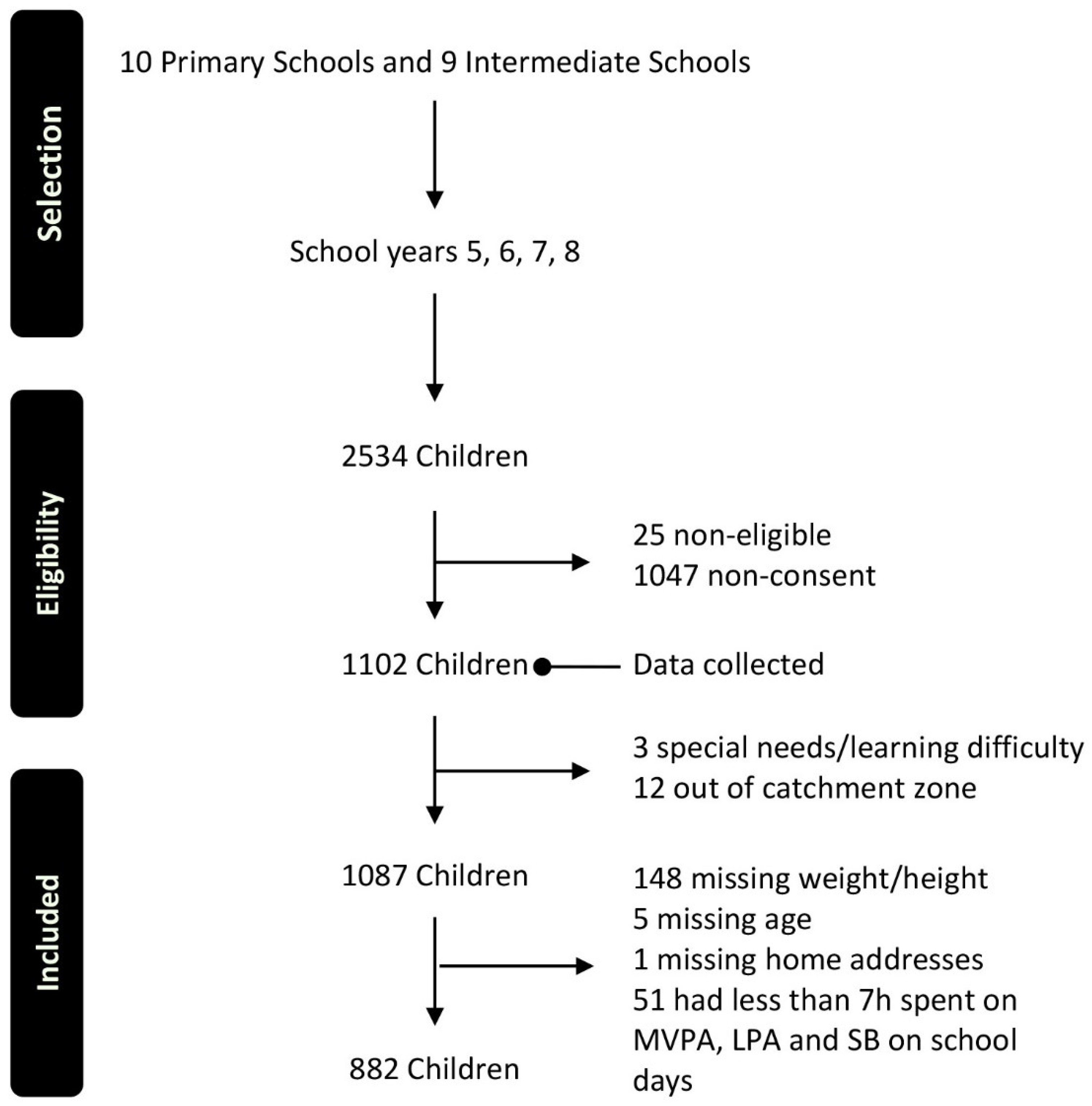
2.1. Participants and Data
2.1.1. Participants
2.1.2. Data
2.2. Visualisation Strategies
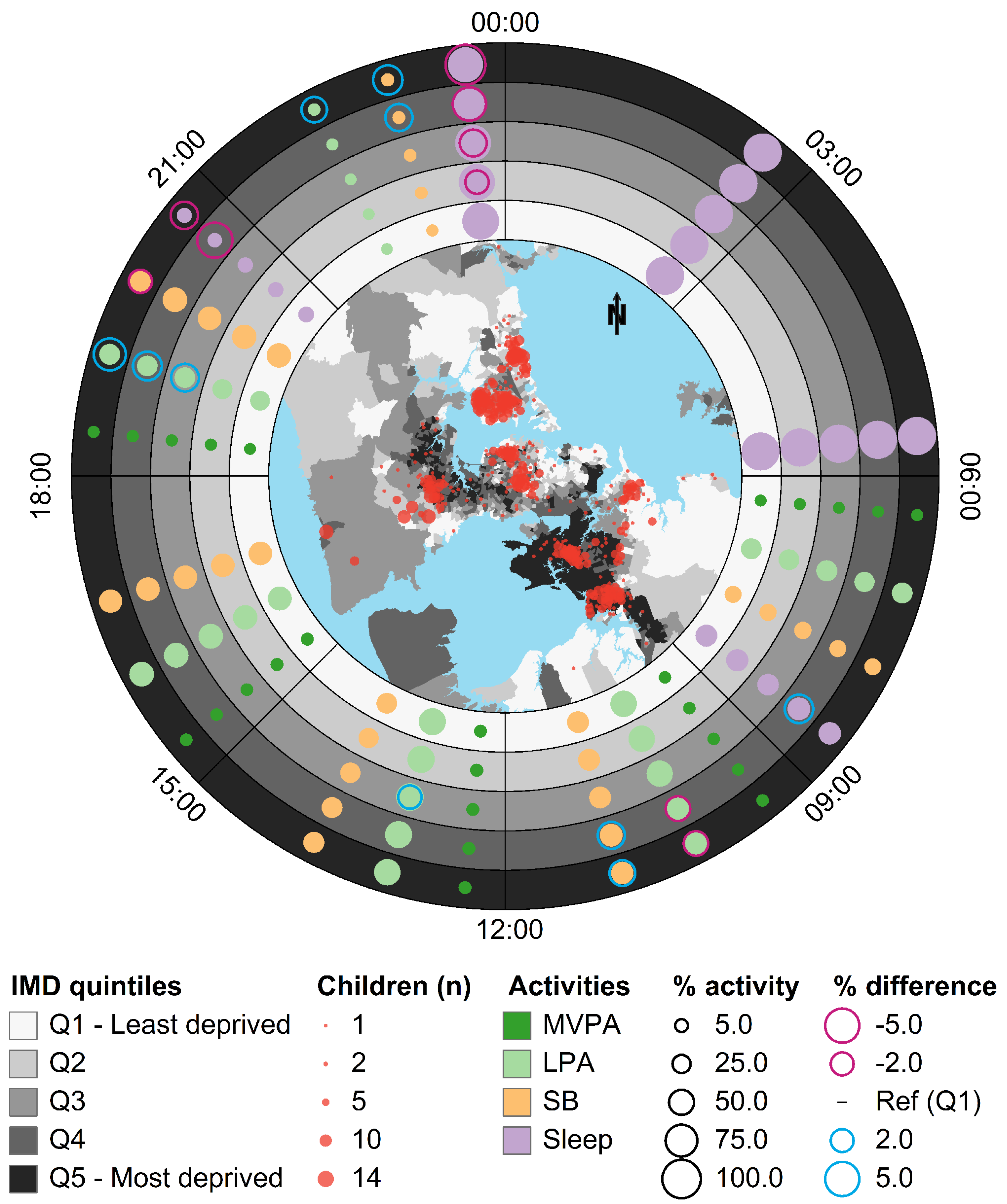
2.2.1. Using Ringmaps to Show an Overview of Patterns in the Data
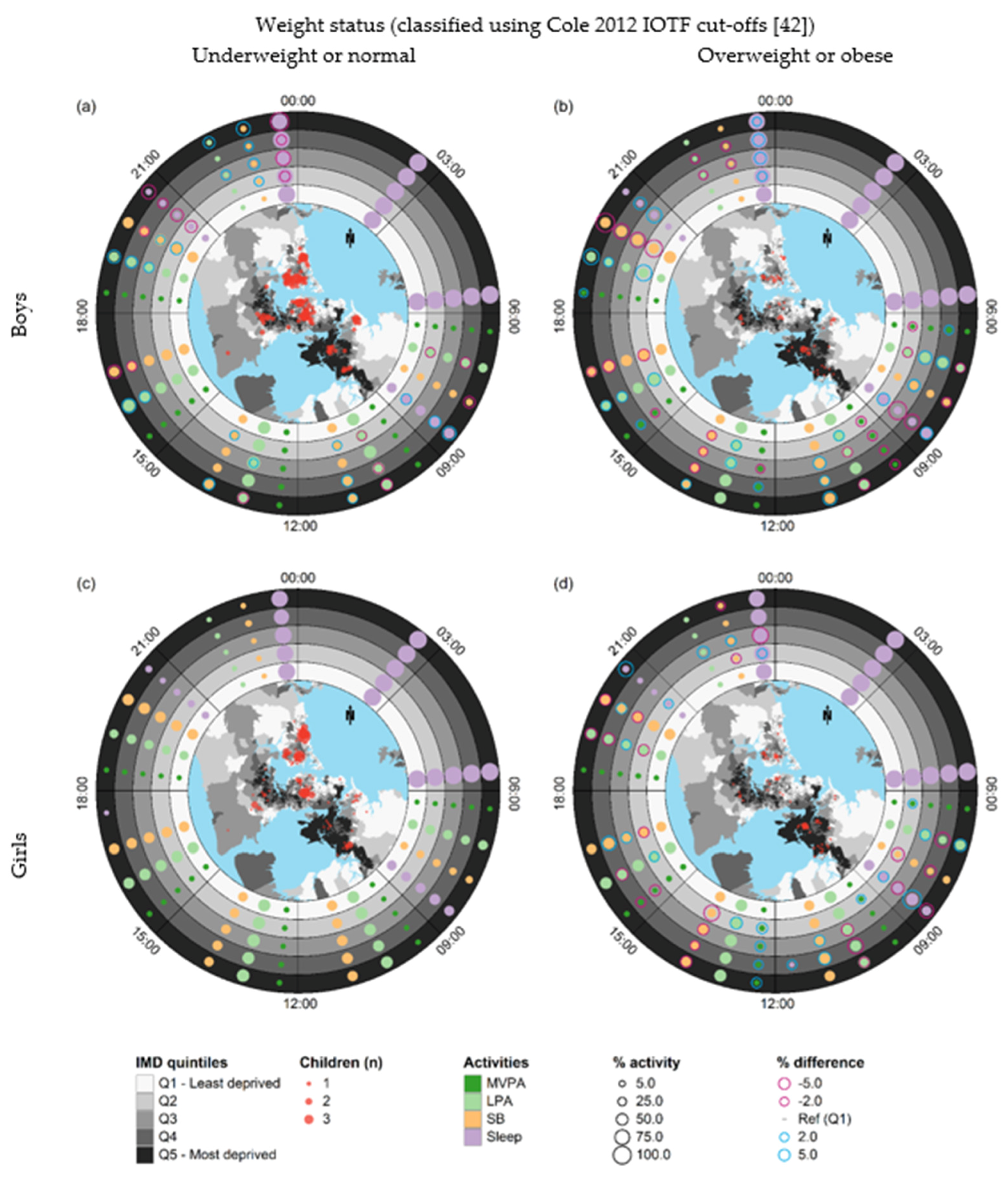
2.2.2. Using Small-Multiple Ringmaps to Compare Patterns in Sub-Sets of the Data
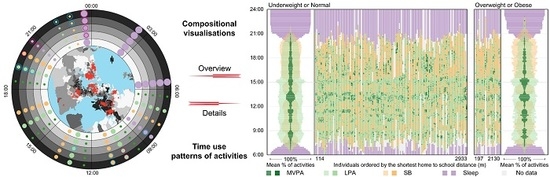
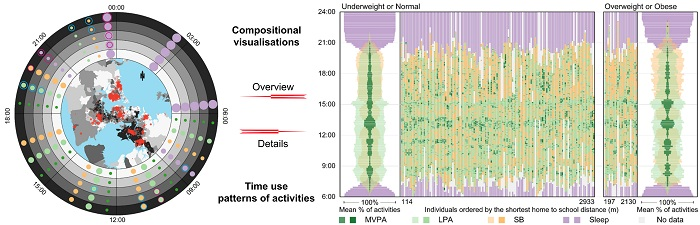
2.2.3. Developing Time–Activity Diagrams to Visualise Patterns at Both the Individual and Aggregated Levels
3. Results
3.1. Socio-Demographic and Weight Status Characteristics of Participants
3.2. Ringmap Overview
3.3. Small-Multiple Ringmaps
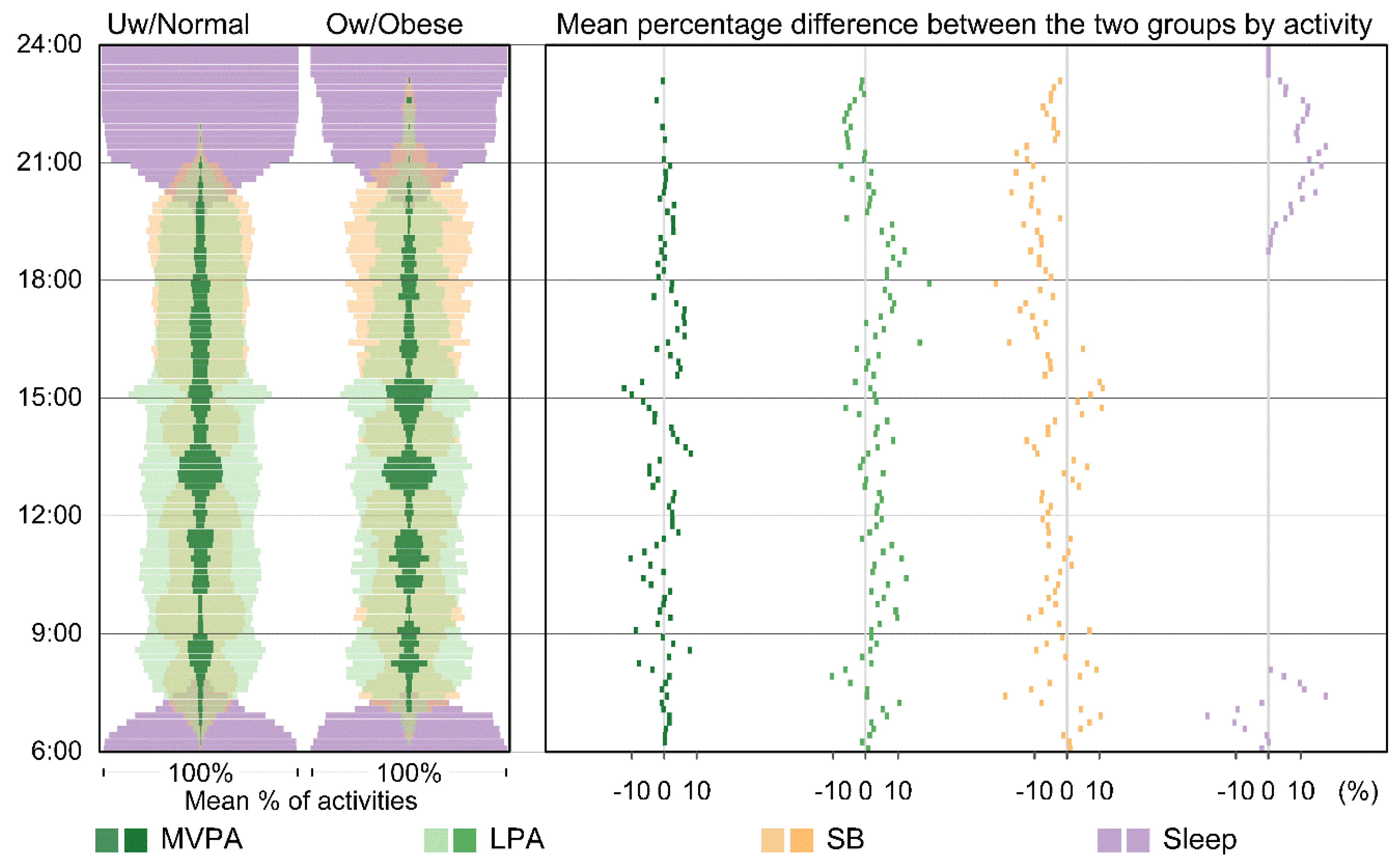
3.4. Time–Activity Diagrams for Aggregated Patterns
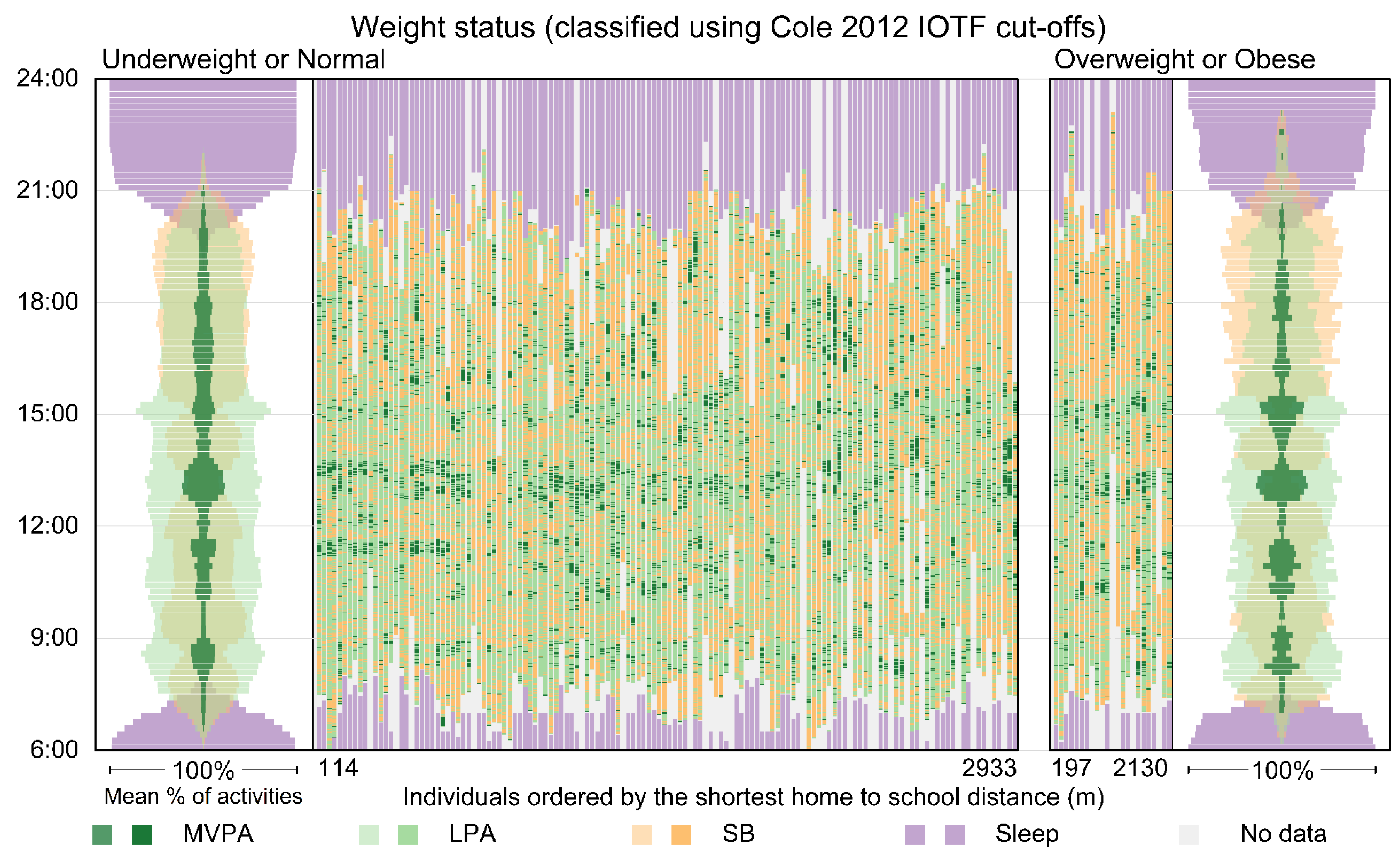
3.5. Time–Activity Diagrams for Individual and Aggregated Patterns
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Olds, T.; Ferrar, K.E.; Gomersall, S.R.; Maher, C.; Walters, J.L. The Elasticity of Time:Associations Between Physical Activity and Use of Time in Adolescents. Health Educ. Behav. 2012, 39, 732–736. [Google Scholar] [CrossRef]
- Harvey, A.S. Time-use studies: A tool for macro and micro economic and social analysis. Soc. Indic. Res. 1993, 30. [Google Scholar] [CrossRef]
- WHO. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans; Department of Health and Human Services: Washington, DC, USA, 2018.
- Bull, F.; the Expert Working Groups. Physical Activity Guidelines in the U.K.: Review and Recommendations. School of Sport, Exercise and Health Sciences; Loughborough University: Loughborough, UK, May 2010. [Google Scholar]
- Dumuid, D.; Stanford, T.E.; Martin-Fernandez, J.A.; Pedisic, Z.; Maher, C.A.; Lewis, L.K.; Hron, K.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; et al. Compositional data analysis for physical activity, sedentary time and sleep research. Stat. Methods Med. Res. 2017, 27, 3726–3738. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Carson, V.; Gray, C.E.; Tremblay, M.S. Importance of All Movement Behaviors in a 24 Hour Period for Overall Health. Int. J. Environ. Res. Public Health 2014, 11, 12575–12581. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Leduc, G.; Boyer, C.; Belanger, P.; LeBlanc, A.G.; Borghese, M.M.; Tremblay, M.S. Objectively measured physical activity, sedentary time and sleep duration: Independent and combined associations with adiposity in canadian children. Nutr. Diabetes 2014, 4, e117. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined Effects of Time Spent in Physical Activity, Sedentary Behaviors and Sleep on Obesity and Cardio-Metabolic Health Markers: A Novel Compositional Data Analysis Approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [PubMed]
- Dunton, G.F.; Berrigan, D.; Ballard-Barbash, R.; Graubard, B.; Atienza, A.A. Joint associations of physical activity and sedentary behaviors with body mass index: Results from a time use survey of US adults. Int. J. Obes. 2009, 33, 1427–1436. [Google Scholar] [CrossRef]
- Rosenberger, M.E.; Buman, M.P.; Haskell, W.L.; McConnell, M.V.; Carstensen, L.L. 24 Hours of Sleep, Sedentary Behavior, and Physical Activity with Nine Wearable Devices. Med. Sci. Sports Exerc. 2016, 48, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Pedišić, Ž. Measurement issues and poor adjustments for physical activity and sleep undermine sedentary behaviour research—The focus should shift to the balance between sleep, sedentary behaviour, standing and activity. Kinesiology 2014, 46, 135–146. [Google Scholar]
- Fairclough, S.J.; Dumuid, D.; Mackintosh, K.A.; Stone, G.; Dagger, R.; Stratton, G.; Davies, I.; Boddy, L.M. Adiposity, fitness, health-related quality of life and the reallocation of time between children's school day activity behaviours: A compositional data analysis. Prev. Med. Rep. 2018, 11, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Canadian Society for Exercise Physiology. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep; Canadian Society for Exercise Physiology: Ottawa, ON, Canada, 2017. [Google Scholar]
- Prentice-Dunn, H.; Prentice-Dunn, S. Physical activity, sedentary behavior, and childhood obesity: A review of cross-sectional studies. Psychol. Health Med. 2012, 17, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Annual Update of Key Results 2015/16: New Zealand Health Survey; Ministry of Health: Wellington, New Zealand, 2016. Available online: http://www.health.govt.nz (accessed on 6 May 2018).
- Barton, M. Childhood obesity: A life-long health risk. Acta Pharmacol. Sin. 2012, 33, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Ashton, T.; Gillespie, J.; Cox, B.; Menon, A.; Simmons, D.; Birkbeck, J. Health care costs of obesity in New Zealand. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Perkins, C.; DeSousa, E. Trends in childhood height and weight, and socioeconomic inequalities. Lancet Public Health 2018, 3, e160–e161. [Google Scholar] [CrossRef]
- Singh, G.K.; Siahpush, M.; Kogan, M.D. Rising Social Inequalities in US Childhood Obesity, 2003–2007. Ann. Epidemiol. 2010, 20, 40–52. [Google Scholar] [CrossRef]
- Frederick, C.B.; Snellman, K.; Putnam, R.D. Increasing socioeconomic disparities in adolescent obesity. Proc. Natl. Acad. Sci. USA 2014, 111, 1338–1342. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M.; Kogan, M.D. Neighborhood socioeconomic conditions, built environments, and childhood obesity. Health Aff. 2010, 29, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Cetateanu, A.; Jones, A. Understanding the relationship between food environments, deprivation and childhood overweight and obesity: Evidence from a cross sectional England-wide study. Health Place 2014, 27, 68–76. [Google Scholar] [CrossRef]
- Kinra, S.; Nelder, R.P.; Lewendon, G.J. Deprivation and childhood obesity: A cross sectional study of 20 973 children in Plymouth, United Kingdom. J. Epidemiol. Community Health 2000, 54, 456–460. [Google Scholar] [CrossRef]
- Patel, V.C.; Spaeth, A.M. Relationships Between Time Use and Obesity in a Representative Sample of Americans. Obesity 2016, 24, 2164–2175. [Google Scholar] [CrossRef]
- Oliver, M.; McPhee, J.; Carroll, P.; Ikeda, E.; Mavoa, S.; Mackay, L.; Kearns, R.A.; Kyttä, M.; Asiasiga, L.; Garrett, N.; et al. Neighbourhoods for Active Kids: Study protocol for a cross-sectional examination of neighbourhood features and children’s physical activity, active travel, independent mobility and body size. BMJ Open 2016, 6. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Dumuid, D.; Taylor, S.; Curry, W.; McGrane, B.; Stratton, G.; Maher, C.; Olds, T. Fitness, fatness and the reallocation of time between children’s daily movement behaviours: An analysis of compositional data. Int. J. Behav. Nutr. Phys. Activ. 2017, 14, 64. [Google Scholar] [CrossRef]
- Maddison, R.; Gemming, L.; Monedero, J.; Bolger, L.; Belton, S.; Issartel, J.; Marsh, S.; Direito, A.; Solenhill, M.; Zhao, J.; et al. Quantifying Human Movement Using the Movn Smartphone App: Validation and Field Study. JMIR Mhealth Uhealth 2017, 5, e122. [Google Scholar] [CrossRef]
- Few, S. Data visualization for human perception. In The Encyclopedia of Human-Computer Interaction, 2nd ed.; Soegaard, M., Dam, R., Eds.; The Interaction Design Foundation: Aarhus, Denmark, 2014. [Google Scholar]
- Goodchild, M.F. Stepping Over The Line: Technological Constraints And the New Cartography. Cartogr. Geogr. Inf. Sci. 1988, 15, 311–319. [Google Scholar] [CrossRef]
- Kim, C. Spatial Data Mining, Geovisualization. In International Encyclopedia of Human Geography; Rob, K., Nigel, T., Eds.; Elsevier: Oxford, UK, 2009; pp. 332–336. [Google Scholar]
- Dodge, M.; McDerby, M.; Turner, M. (Eds.) The Power of Geographical Visualizations. In Geographic Visualization; Wiley: Hoboken, NJ, USA, 2008; pp. 1–10. [Google Scholar]
- NCD Risk Factor Collaboration. Adult Body-Mass Index. Available online: http://www.ncdrisc.org/data-visualisations-adiposity.html (accessed on 19 December 2018).
- Battersby, S.E.; Stewart, J.E.; Fede, A.L.-D.; Remington, K.C.; Mayfield-Smith, K. Ring maps for spatial visualization of multivariate epidemiological data. J. Maps 2011, 7, 564–572. [Google Scholar] [CrossRef]
- Zhao, J.; Exeter, D.J.; Hanham, G.; Lee, A.C.L.; Browne, M.; Grey, C.; Wells, S. Using integrated visualization techniques to investigate associations between cardiovascular health outcomes and residential migration in Auckland, New Zealand. Cartogr. Geogr. Inf. Sci. 2015, 42, 381–397. [Google Scholar] [CrossRef]
- Weimann, A.; Dai, D.; Oni, T. A cross-sectional and spatial analysis of the prevalence of multimorbidity and its association with socioeconomic disadvantage in South Africa: A comparison between 2008 and 2012. Soc. Sci. Med. 2016, 163, 144–156. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef]
- Casey, A.A.; Elliott, M.; Glanz, K.; Haire-Joshu, D.; Lovegreen, S.L.; Saelens, B.E.; Sallis, J.F.; Brownson, R.C. Impact of the food environment and physical activity environment on behaviors and weight status in rural U.S. communities. Prev. Med. 2008, 47, 600–604. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Zhao, J.; Forer, P.; Harvey, A.S. Activities, ringmaps and geovisualization of large human movement fields. Inf. Visual. 2008, 7, 198–209. [Google Scholar] [CrossRef]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, E.; Mavoa, S.; Hinckson, E.; Witten, K.; Donnellan, N.; Smith, M. Differences in child-drawn and GIS-modelled routes to school: Impact on space and exposure to the built environment in Auckland, New Zealand. J. Transp. Geogr. 2018, 71, 103–115. [Google Scholar] [CrossRef]
- Exeter, D.J.; Zhao, J.; Crengle, S.; Lee, A.; Browne, M. The New Zealand Indices of Multiple Deprivation (IMD): A new suite of indicators for social and health research in Aotearoa, New Zealand. PLoS ONE 2017, 12, e0181260. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Exeter, D.J. Developing intermediate zones for analysing the social geography of Auckland, New Zealand. N. Zeal. Geogr. 2016, 72, 14–27. [Google Scholar] [CrossRef]
- Mattocks, C.; Leary, S.; Ness, A.; Deere, K.; Saunders, J.; Kirkby, J.; Blair, S.N.; Tilling, K.; Riddoch, C. Intraindividual Variation of Objectively Measured Physical Activity in Children. Med. Sci. Sports Exerc. 2007, 39, 622–629. [Google Scholar] [CrossRef] [PubMed]
- SAS Institute Inc. SAS Enterprise Guide 7.1; SAS Institute Inc.: Cary, NC, USA, 2014. [Google Scholar]
- Zhao, J.; Forer, P.; Sun, Q.; Simmons, D. Multiple-view strategies for enhanced understanding of dynamic tourist activity through geovisualization at regional and national scales. Cartogr. Geogr. Inf. Sci. 2013, 40, 349–360. [Google Scholar] [CrossRef]
- Tufte, E.R. The Visual Display of Quantitative Information; Graphics Press: Cheshire, CT, USA, 1983; p. 197. [Google Scholar]
- Slocum, T.A.; Sluter, R.S., Jr.; Kessler, F.C.; Yoder, S.C. A qualitative evaluation of maptime, a program for exploring spatiotemporal point data. Cartographica 2004, 39, 43–68. [Google Scholar] [CrossRef]
- MacEachren, A.; Dai, X.; Hardisty, F.; Guo, D.; Lengerich, G. Exploring High-D Spaces with Multiform Matricies and Small Multiples. In Proceedings of the International Symposium on Information Visualization, Seattle, WA, USA, 19–21 October 2003. [Google Scholar]
- Fabrikant, S.I.; Rebich-Hespanha, S.; Andrienko, N.; Andrienko, G.; Montello, D.R. Novel Method to Measure Inference Affordance in Static Small-Multiple Map Displays Representing Dynamic Processes. Cartogr. J. 2008, 45, 201–215. [Google Scholar] [CrossRef]
- Dumuid, D.; Stanford, T.E.; Pedišić, Ž.; Maher, C.; Lewis, L.K.; Martín-Fernández, J.-A.; Katzmarzyk, P.T.; Chaput, J.-P.; Fogelholm, M.; Standage, M.; et al. Adiposity and the isotemporal substitution of physical activity, sedentary time and sleep among school-aged children: A compositional data analysis approach. BMC Public Health 2018, 18, 311. [Google Scholar] [CrossRef]
- Olds, T.; Burton, N.W.; Sprod, J.; Maher, C.; Ferrar, K.; Brown, W.J.; van Uffelen, J.; Dumuid, D. One day you’ll wake up and won’t have to go to work: The impact of changes in time use on mental health following retirement. PLoS ONE 2018, 13, e0199605. [Google Scholar] [CrossRef]
- Vrotsou, K.; Ellegård, K.; Cooper, M. Everyday life discoveries: Mining and visualizing activity patterns in social science diary data. In Proceedings of the 11th International Conference Information Visualization, Zurich, Switzerland, 4–6 July 2007. [Google Scholar]
- Pearson, H. The time lab: Why does modern life seem so busy? Nature 2015, 526, 492–496. [Google Scholar] [CrossRef]
- Jago, R.; Salway, R.; Lawlor, D.A.; Emm-Collison, L.; Heron, J.; Thompson, J.L.; Sebire, S.J. Profiles of children’s physical activity and sedentary behaviour between age 6 and 9: A latent profile and transition analysis. Int. J. Behav. Nutr. Phys. Activ. 2018, 15, 103. [Google Scholar] [CrossRef]
- Zhao, J.; Forer, P.; Walker, M.; Dennis, T. The Space–Time Aquarium is Full of Albatrosses: Time Geography, Lifestyle and Trans-species Geovisual Analytics. In Geospatial Visualisation; Moore, A., Drecki, I., Eds.; Springer: Heidelberg/Berlin, Germany, 2013; pp. 235–260. [Google Scholar]
- Zhao, J.; Chang, K.; Smith-nee Oliver, M. Creating Time-Activity Diagrams to Visualise Compositional Time Use Patterns of Daily Activities Using R. Figshare. Code. 2019. Available online: https://figshare.com/ (accessed on 23 February 2019). [CrossRef]
- Olds, T.; Maher, C.A.; Ridley, K. The Place of Physical Activity in the Time Budgets of 10- to 13-Year-Old Australian Children. J. Phys. Activ. Health 2011, 8, 548–557. [Google Scholar] [CrossRef]
- Stanley, R.M.; Boshoff, K.; Dollman, J. A Qualitative Exploration of the “Critical Window”: Factors Affecting Australian Children’s After-School Physical Activity. J. Phys. Activ. Health 2013, 10, 33–41. [Google Scholar] [CrossRef]
- Zhao, J.; Exeter, D.; Moss, L.; Hanham, G.; Riddell, T.; Wells, S. Incorporating Ringmaps into Interactive Web Mapping for Enhanced Understanding of Cardiovascular Disease. In Proceedings of the 21st International Conference on Geoinformatics, Kaifeng, China, 20–22 June 2013; Institute of Electrical and Electronics Engineers (IEEE); pp. 595–600. [Google Scholar] [CrossRef]
- Cooper, A.R.; Jago, R.; Southward, E.F.; Page, A.S. Active travel and physical activity across the school transition: The PEACH project. Med. Sci. Sports Exerc. 2012, 44, 1890–1897. [Google Scholar] [CrossRef]
- Lubans, D.R.; Boreham, C.A.; Kelly, P.; Foster, C.E. The relationship between active travel to school and health-related fitness in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Activ. 2011, 8, 5. [Google Scholar] [CrossRef]
- Stewart, T.; Duncan, S.; Schipperijn, J. Adolescents who engage in active school transport are also more active in other contexts: A space-time investigation. Health Place 2017, 43, 25–32. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Boys | Girls | |||
|---|---|---|---|---|---|
| n | n | % | n | % | |
| Total | 882 | 437 | 49.5 | 445 | 50.5 |
| Age group | (mean = 10.66, SD = 1.18) | (mean = 10.53, SD = 1.20) | |||
| ≤9 | 187 | 83 | 44.4 | 104 | 55.6 |
| 10 | 234 | 115 | 49.1 | 119 | 50.9 |
| 11 | 234 | 119 | 50.9 | 115 | 49.1 |
| ≥12 | 190 | 101 | 53.2 | 89 | 46.8 |
| Weight | (mean = 43.24, SD = 12.17) | (mean = 43.70, SD = 14.31) | |||
| Height | (mean = 1.49, SD = 0.09) | (mean = 1.48, SD = 0.10) | |||
| Weight status (classified using Cole 2012 IOTF cut-offs [42]) | |||||
| Underweight or Normal | 640 | 325 | 50.8 | 315 | 49.2 |
| Overweight or Obese | 242 | 112 | 46.3 | 130 | 53.7 |
| IMD Quintiles | (mean = 2.89, SD = 1.48) | (mean = 3.0, SD = 1.5) | |||
| Q1—Least deprived | 194 | 101 | 52.1 | 93 | 47.9 |
| Q2 | 204 | 101 | 49.5 | 103 | 50.5 |
| Q3 | 157 | 79 | 50.3 | 78 | 49.7 |
| Q4 | 112 | 57 | 50.9 | 55 | 49.1 |
| Q5—Most deprived | 215 | 99 | 46 | 116 | 54 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, J.; Mackay, L.; Chang, K.; Mavoa, S.; Stewart, T.; Ikeda, E.; Donnellan, N.; Smith, M. Visualising Combined Time Use Patterns of Children’s Activities and Their Association with Weight Status and Neighbourhood Context. Int. J. Environ. Res. Public Health 2019, 16, 897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050897
Zhao J, Mackay L, Chang K, Mavoa S, Stewart T, Ikeda E, Donnellan N, Smith M. Visualising Combined Time Use Patterns of Children’s Activities and Their Association with Weight Status and Neighbourhood Context. International Journal of Environmental Research and Public Health. 2019; 16(5):897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050897
Chicago/Turabian StyleZhao, Jinfeng, Lisa Mackay, Kevin Chang, Suzanne Mavoa, Tom Stewart, Erika Ikeda, Niamh Donnellan, and Melody Smith. 2019. "Visualising Combined Time Use Patterns of Children’s Activities and Their Association with Weight Status and Neighbourhood Context" International Journal of Environmental Research and Public Health 16, no. 5: 897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050897