A Study of Physical Activity Determinants among High-Risk Hypertensive Filipino and Korean Americans

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Participants
2.3. Measures
2.3.1. Physical Activity Levels
2.3.2. Sociodemographic
2.3.3. Health-Related Factors
2.3.4. Body Mass Index (BMI)
2.4. Statistical Analysis
3. Results
3.1. Physical Activity Levels
3.2. Descriptive Characteristics among All Participants and by Physical Activity Level Group
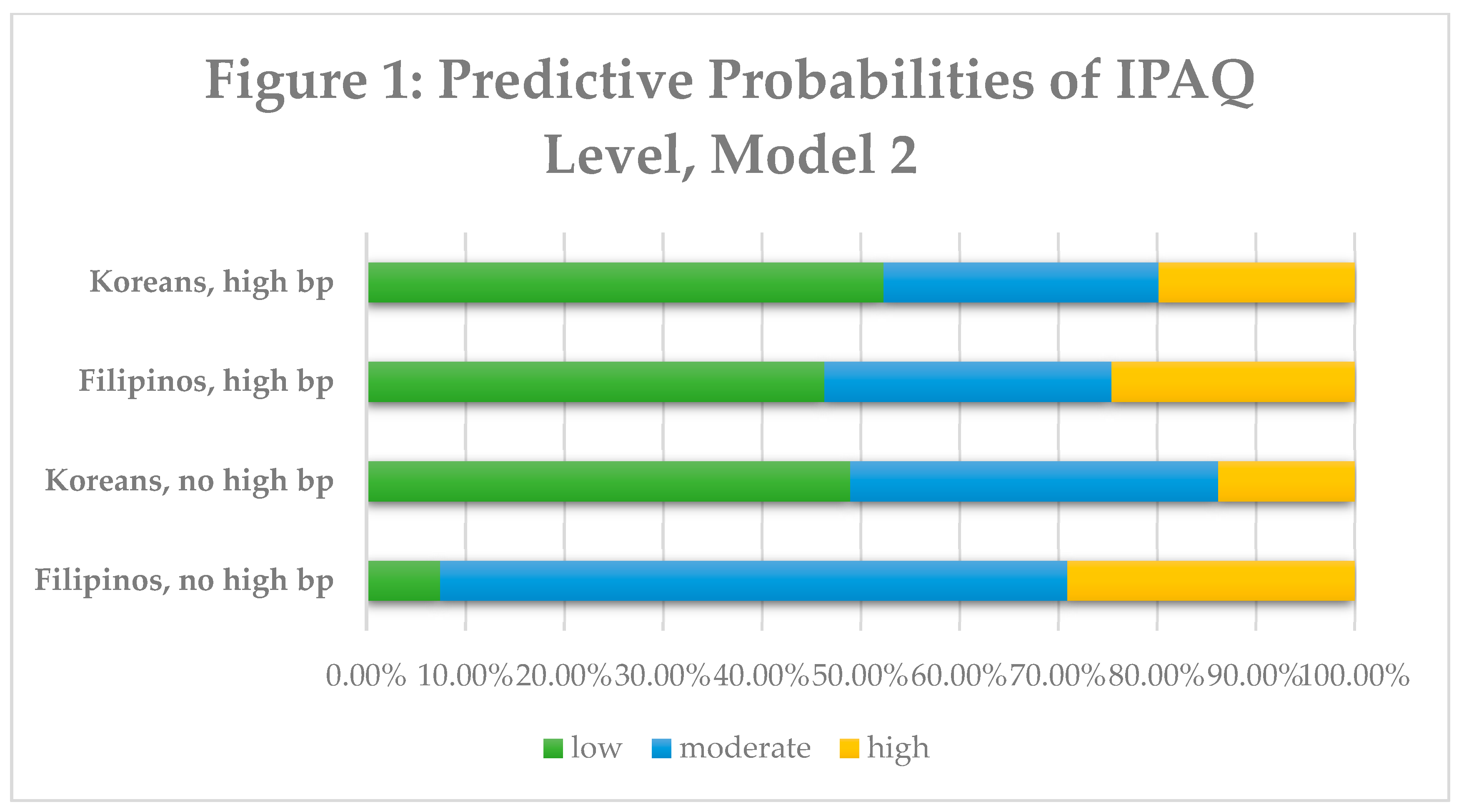
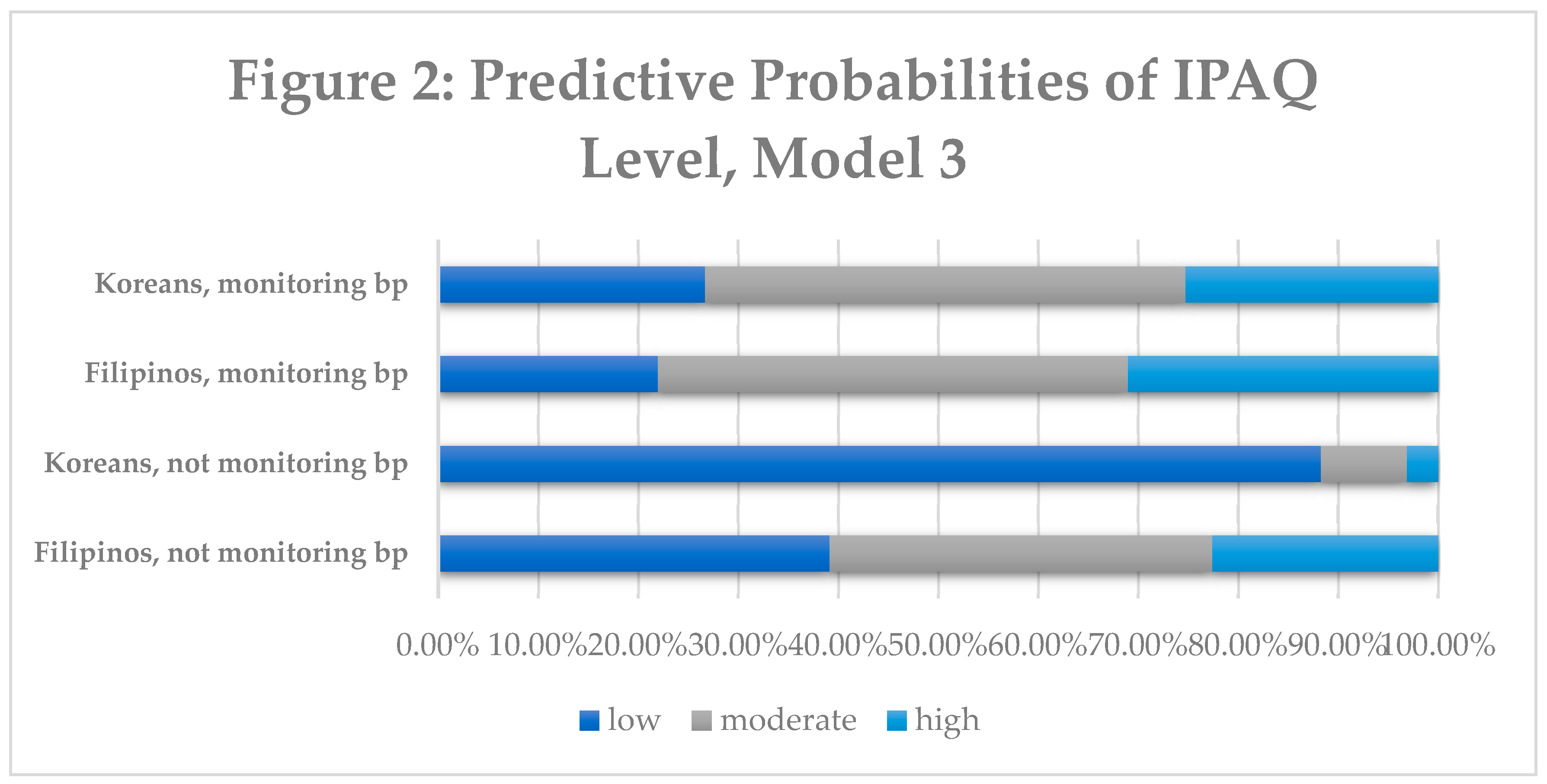
3.3. Multinomial Logistic Regression and Predictive Probability Analyses
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Palaniappan, L.P.; Araneta, M.R.G.; Assimes, T.L.; Barrett-Connor, E.L.; Carnethon, M.R.; Criqui, M.H.; Fung, G.L.; Venkat Narayan, K.M.; Patel, H.; Taylor-Piliae, R.E.; et al. Call to Action: Cardiovascular Disease in Asian Americans a Science Advisory from the American Heart Association. Circulation 2010, 122, 1242–1252. [Google Scholar] [CrossRef] [PubMed]
- Dela Cruz, F.A.; McBride, M.R.; Compas, L.B.; Calixto, P.-R.; Van Derveer, C.P. White paper on the health status of Filipino Americans and recommendations for research. Nurs. Outlook 2002, 50, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Abesamis, C.J.; Fruh, S.; Hall, H.; Lemley, T.; Zlomke, K.R. Cardiovascular Health of Filipinos in the United States: A Review of the Literature. J. Transcult. Nurs. 2016, 27, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Bayog, M.L.; Waters, C.M. Cardiometabolic risks, lifestyle health behaviors and heart disease in Filipino Americans. Eur. J. Cardiovasc. Nurs. 2017, 16, 522–529. [Google Scholar] [CrossRef]
- Palaniappan, L.P.; Wong, E.C.; Shin, J.J.; Fortmann, S.P.; Lauderdale, D.S. Asian Americans Have Greater Prevalence of Metabolic Syndrome Despite Lower Body Mass Index. Int. J. Obes. (Lond.) 2011, 35, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Klatsky, A.L.; Armstrong, M.A. Cardiovascular risk factors among Asian Americans living in northern California. Am. J. Public Health 1991, 81, 1423–1428. [Google Scholar] [CrossRef] [PubMed]
- Maryland Asian American Health Solution (MAAHS). University of Maryland College Park School of Public Health Korean Community Needs Assessment Summary Report; University of Maryland: College Park, MD, USA, 2007. [Google Scholar]
- Patterson, F.; Zhang, G.; Davey, A.; Tan, Y.; Ma, G.X. American Heart Association’s Ideal Cardiovascular Health Metrics in Under-Represented Asian Americans. J. Community Health 2016, 41, 1282–1289. [Google Scholar] [CrossRef] [Green Version]
- Ancheta, I.B.; Battie, C.A.; Tuason, M.T.; Borja-Hart, N.; Ancheta, C.V. The prevalence of cardiovascular risk factors and diabetes increases with a body mass index of > or = 23 kg/m2 in Filipino American women. Ethn. Dis. 2014, 24, 48–54. [Google Scholar] [PubMed]
- Jamerson, K.; Julius, S. Predictors of Blood Pressure and Hypertension General Principles. Am. J. Hypertens. 1991, 4, 598S–602S. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Lee, S.J.; Ahn, Y.-H.; Bowen, P.; Lee, H. Dietary acculturation and diet quality of hypertensive Korean Americans. J. Adv. Nurs. 2007, 58, 436–445. [Google Scholar] [CrossRef]
- Vargas, P.; Jurado, L.-F. Dietary Acculturation among Filipino Americans. Int. J. Environ. Res. Public Health 2015, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Brands, M.W.; Daniels, S.R.; Karanja, N.; Elmer, P.J.; Sacks, F.M.; American Heart Association. Dietary approaches to prevent and treat hypertension: A scientific statement from the American Heart Association. Hypertension 2006, 47, 296–308. [Google Scholar] [CrossRef] [PubMed]
- Jose, P.; Zhao, B.; Chung, S.; Fortmann, S.; Palaniappan, L. PS1-46: Variation in Hypertension Prevalence Among Asian American Subgroups: Results from PACS (Pan Asian Cohort Study). Clin. Med. Res. 2013, 11, 136. [Google Scholar] [CrossRef]
- Ghimire, S.; Cheong, P.; Sagadraca, L.; Chien, L.-C.; Sy, F.S. A Health Needs Assessment of the Filipino American Community in the Greater Las Vegas Area. Health Equity 2018, 2, 334–348. [Google Scholar] [CrossRef] [PubMed]
- Bhimla, A.; Yap, L.; Lee, M.; Seals, B.; Aczon, H.; Ma, G.X. Addressing the Health Needs of High-Risk Filipino Americans in the Greater Philadelphia Region. J. Community Health 2017, 42, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Ursua, R.A.; Islam, N.S.; Aguilar, D.E.; Wyatt, L.C.; Tandon, S.D.; Abesamis-Mendoza, N.; Nur, P.R.M.Q.; Rago-Adia, J.; Ileto, B.; Rey, M.J.; et al. Predictors of hypertension among Filipino immigrants in the Northeast US. J. Community Health 2013, 38, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.-N.; Keller, C.; An, K.; Sim, J. Cardiovascular Disease in Korean Americans: A Systematic Review. J Cardiovasc. Nurs. 2018, 33, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical Activity and Public Health. Updated Recommendation for Adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 38, 1423–1434. [Google Scholar]
- Becerra, M.B.; Herring, P.; Marshak, H.H.; Banta, J.E. Social Determinants of Physical Activity Among Adult Asian-Americans: Results from a Population-Based Survey in California. J. Immigr. Minority Health 2015, 17, 1061–1069. [Google Scholar] [CrossRef]
- Kao, D.; Carvalho Gulati, A.; Lee, R.E. Physical Activity Among Asian American Adults in Houston, Texas: Data from the Health of Houston Survey 2010. J. Immigr Minor Health 2016, 18, 1470–1481. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.S.; Roberts, C.; Lightstone, A.S.; Shih, M.; Trinh-Shevrin, C. Disparities in meeting physical activity guidelines for Asian Americans in two metropolitan areas in the United States. Ann. Epidemiol. 2015, 25, 656–660.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Church, T. Exercise in obesity, metabolic syndrome, and diabetes. Prog. Cardiovasc. Dis. 2011, 53, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, P. The role of physical activity and exercise in obesity and weight management: Time for critical appraisal. J. Sport Health Sci. 2016, 5, 151–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.; Juon, H.-S. Assessing Overweight and Obesity Risk Among Korean Americans in California Using World Health Organization Body Mass Index Criteria for Asians. Prev. Chronic Dis. 2006, 3, A79. [Google Scholar] [PubMed]
- Staimez, L.R.; Weber, M.B.; Narayan, K.M.V.; Oza-Frank, R. A systematic review of overweight, obesity, and type 2 diabetes among Asian American subgroups. Curr. Diabetes Rev. 2013, 9, 312–331. [Google Scholar] [CrossRef]
- WHO Expert Consultation Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [CrossRef]
- Jih, J.; Mukherjea, A.; Vittinghoff, E.; Nguyen, T.T.; Tsoh, J.Y.; Fukuoka, Y.; Bender, M.S.; Tseng, W.; Kanaya, A.M. Using appropriate body mass index cut points for overweight and obesity among Asian Americans. Prev. Med. 2014, 65, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Serafica, R.; Angosta, A.D. Acculturation and changes in body mass index, waist circumference, and waist–hip ratio among Filipino Americans with hypertension. J. Am. Soc. Hypertens. 2016, 10, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.B.; Macfarlane, D.J.; Thomas, G.N.; Lao, X.Q.; Jiang, C.Q.; Cheng, K.K.; Lam, T.H. Reliability and validity of the IPAQ-Chinese: The Guangzhou Biobank Cohort study. Med. Sci. Sports Exerc. 2008, 40, 303–307. [Google Scholar] [CrossRef]
- Dinger, M.K.; Behrens, T.K.; Han, J.L. Validity and Reliability of the International Physical Activity Questionnaire in College Students. Am. J. Health Educ. 2006, 37, 337–343. [Google Scholar] [CrossRef]
- Sjostrom, M.; Ainsworth, B.; Bauman, A.; Bull, F.; Craig, C.; Sallis, J. Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ) short form. Available online: http://www.institutferran.org/documentos/scoring_short_ipaq_april04.pdf (accessed on 11 December 2018).
- CDC Physical Activity Basics. Available online: https://www.cdc.gov/physicalactivity/basics/index.htm (accessed on 11 November 2016).
- Choi, J.; Wilbur, J.; Miller, A.; Szalacha, L.; McAuley, E. Correlates of leisure-time physical activity in Korean immigrant women. West. J. Nurs. Res. 2008, 30, 620–638. [Google Scholar] [CrossRef]
- Atienza, A.A.; King, A.C. Comparing Self-Reported Versus Objectively Measured Physical Activity Behavior: A Preliminary Investigation of Older Filipino American Women. Res. Q. Exerc. Sport 2005, 76, 358–362. [Google Scholar] [CrossRef]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, A.E.; Crespi, C.M.; Alano, R.E.; Sudan, M.; Bastani, R. Health Risk Behaviors among Five Asian American Subgroups in California: Identifying Intervention Priorities. J. Immigr. Minor Health 2012, 14, 890–894. [Google Scholar] [CrossRef] [PubMed]
- Berry, B.; Berry, J.W. Acculturation: Living successfully in two cultures. Int. J. Intercult. Relat. 2005, 29, 697–712. [Google Scholar] [CrossRef]
- Song, Y.J.; Hofstetter, C.R.; Hovell, M.F.; Paik, H.Y.; Park, H.R.; Lee, J.; Irvin, V. Acculturation and health risk behaviors among Californians of Korean descent. Prev. Med. 2004, 39, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Afable-Munsuz, A.; Ponce, N.A.; Rodriguez, M.; Perez-Stable, E.J. Immigrant generation and physical activity among Mexican, Chinese & Filipino adults in the U.S. Soc. Sci. Med. 2010, 70, 1997–2005. [Google Scholar] [PubMed]
- Shaw, B.A.; Spokane, L.S. Examining the Association between Education Level and Physical Activity Changes During Early Old Age. J. Aging Health 2008, 20, 767–787. [Google Scholar] [CrossRef]
- Lewis, J.; Ma, G.; Patterson, F.; Wang, M.Q. Correlates of blood pressure control behaviors among Korean Americans in the greater Philadelphia area. Psychol. Rep. 2013, 113, 908–920. [Google Scholar] [CrossRef]
- Han, H.-R.; Kim, K.B.; Kang, J.; Jeong, S.; Kim, E.-Y.; Kim, M.T. Knowledge, beliefs, and behaviors about hypertension control among middle-aged Korean Americans with hypertension. J. Community Health 2007, 32, 324–342. [Google Scholar] [CrossRef]
- Angosta, A.D.; Serafica, R. Assessing Physical Activity Levels in Filipino Americans With Hypertension Using the Rapid Assessment of Physical Activity Questionnaire. Home Health Care Manag. Pract. 2017, 29, 91–95. [Google Scholar] [CrossRef]
- Maneze, D.; DiGiacomo, M.; Salamonson, Y.; Descallar, J.; Davidson, P.M. Facilitators and Barriers to Health-Seeking Behaviours among Filipino Migrants: Inductive Analysis to Inform Health Promotion. Biomed. Res. Int. 2015, 2015, 506269. [Google Scholar] [CrossRef]
- Han, B.; Sadarangani, T.; Wyatt, L.C.; Zanowiak, J.M.; Kwon, S.C.; Trinh-Shevrin, C.; Lee, L.; Islam, N.S. Correlates of Physical Activity Among Middle-Aged and Older Korean Americans at Risk for Diabetes. J. Nurs. Sch. 2016, 48, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Belza, B.; Walwick, J.; Shiu-Thornton, S.; Schwartz, S.; Taylor, M.; LoGerfo, J. Older adult perspectives on physical activity and exercise: Voices from multiple cultures. Prev. Chronic Dis. 2004, 1, A09. [Google Scholar] [PubMed]
- Pettee, K.K.; Brach, J.S.; Kriska, A.M.; Boudreau, R.; Richardson, C.R.; Colbert, L.H.; Satterfield, S.; Visser, M.; Harris, T.B.; Ayonayon, H.N.; et al. Influence of Marital Status on Physical Activity Levels among Older Adults. Med. Sci. Sports Exerc. 2006, 38, 541–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| PA Scoring |
| Vigorous PA = 8 × (vigorous activity per day) × (minutes of vigorous activity per day) |
| Moderate PA = 4 × (moderate activity per day) × (minutes of moderate activity per day) |
| Walking PA = 3.3 × (walking per day) × (minutes of walking per day) |
| Total PA score = Vigorous PA + Moderate PA + Walking PA |
| PA Classification Criteria |
| Category 1: Low active |
| No activity is reported or some activity is reported but not enough to meet the other two categories. |
| Category 2: Moderately active—any of the following criteria: |
| 3 or more days of vigorous activity of at least 20 minutes per day |
| 5 or more days of moderate intensity activity or walking of at least 30 minutes per day |
| 5 or more days of any combination of walking, moderate-intensity, and vigorous activities achieving a minimum of at least 600 MET−min/week. |
| Category 3: Highly active—any of the following: |
| Vigorous activity on at least 3 days and accumulating at least 1500 MET−minutes/week, 7 or more days of any combination of walking, moderate, or vigorous activity achieving a minimum of at least 3000 MET−minutes/week. |
| Physical Activity Levels (METs) | Low Category | Moderate Category | High Category | Total |
|---|---|---|---|---|
| Mean, standard deviation | 37.86 ± 162.51 | 703.43 ± 1060.41 | 6134.25 ± 2765.60 | 1654.61 ± 2804.59 |
| Variable | Low | Moderate | High | All |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Age (years) | ||||
| Under 40 | 3 (37.5) | 4 (50) | 1 (12.5) | 8 (5.84) |
| 40–64 | 26 (44.07) | 17 (28.81) | 16 (27.12) | 59 (43.07) |
| 65+ | 20 (28.57) | 37 (52.86) | 13 (18.57) | 70 (51.09) |
| p = 0.090 ‡ | ||||
| Ethnicity | ||||
| Filipino | 20 (28.17) | 33 (46.48) | 18 (25.35) | 71 (51.82) |
| Korean | 29 (43.94) | 25 (37.88) | 12 (18.18) | 66 (48.18) |
| p = 0.151 | ||||
| Gender | ||||
| Male | 12 (29.27) | 18 (43.90) | 11 (26.83) | 41 (29.93) |
| Female | 37 (38.54) | 40 (41.67) | 19 (19.79) | 96 (70.07) |
| p = 0.503 | ||||
| Marital status | ||||
| Married | 34 (36.56) | 36 (38.71) | 23 (24.73) | 93 (71.54) |
| Never married | 4 (50.00) | 3 (37.50) | 1 (12.50) | 8 (6.15) |
| Divorced/widowed/separated | 10 (34.48) | 15 (15.72) | 4 (13.79) | 29 (22.31) |
| p = 0.574 ‡ | ||||
| Education | ||||
| ≤High school | 12 (46.15) | 10 (38.46) | 4 (15.38) | 26 (19.26) |
| ≥College | 37 (33.94) | 46 (42.20) | 26 (23.85) | 109 (80.74) |
| p = 0.447 | ||||
| Asian BMI | ||||
| Underweight or normal weight | 22 (32.35) | 30 (44.12) | 16 (25.53) | 68 (51.13) |
| Overweight or obese | 25 (38.46) | 26 (40.00) | 14 (21.54) | 65 (48.87) |
| p = 0.762 | ||||
| Have health insurance | ||||
| Yes | 38 (32.30) | 51 (43.22) | 29 (24.58) | 118 (89.39) |
| No | 11 (78.57) | 2 (14.29) | 1 (7.14) | 14 (10.61) |
| p = 0.003 * ‡ | ||||
| Have high blood pressure | ||||
| Yes | 23 (35.94) | 26 (40.63) | 15 (23.44) | 65 (50.39) |
| No | 24 (39.92) | 26 (40.00) | 15 (23.08) | 64 (49.61) |
| p = 0.993 | ||||
| Monitor blood pressure | ||||
| Yes | 27 (27.84) | 45 (46.39) | 25 (25.77) | 97 (72.39) |
| No | 21 (56.76) | 11 (29.73) | 5 (13.51) | 37 (27.61) |
| p = 0.007 * |
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| Moderate Act. | High Act. | Moderate Act. | High Act. | Moderate Act. | High Act. | Moderate Act. | High Act. | |
| (vs. Low) | (vs. Low) | (vs. Low) | (vs. Low) | (vs. Low) | (vs. Low) | (vs. Low) | (vs. Low) | |
| Coefficient | Coefficient | Coefficient | Coefficient | Coefficient | Coefficient | Coefficient | Coefficient | |
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | |
| Age | ||||||||
| Under 40 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| 40–64 | −1.16 (−3.31–0.98) | −0.18 (−3.04–2.68) | −1.38 (−3.54–0.78) | −0.42 (−3.33–2.48) | −1.13 (−3.31–1.05) | −0.16 (−3.12–2.80) | −1.29 (−3.48–0.89) | −0.34 (3.30–2.63) |
| 65+ | −0.64 (−2.95–1.66) | −1.14 (−4.16–1.87) | −0.74 (−3.05–1.57) | −1.23 (−4.26–1.81) | −0.50 (−2.87–1.86) | −0.99 (−4.12–2.13) | −0.62 (−2.97–1.73) | −1.10 (−4.21–2.00) |
| Ethnic | ||||||||
| Filipino | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Korean | −0.43 (−1.71–0.85) | −1.17 (−2.63–0.28) | −1.55 (−3.28–0.19) | −2.32 (−4.30–−0.35) * | −1.66 (−3.66–0.33) | −2.62 (−5.26–0.01) | −1.95 (−4.01–0.12) | −2.89 (−5.57–−0.21) * |
| Gender | ||||||||
| Male | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Female | −0.46 (−1.69–0.76) | −0.88 (−2.24–0.47) | −0.34 (−1.58–0.91) | −0.78 (−2.16–0.59) | −0.15 (−1.43–1.12) | −0.58 (−1.97–0.80) | −0.20 (−1.48–1.09) | −0.63 (−2.04–0.77) |
| Marital status | ||||||||
| Married | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Never married | −0.96 (−3.12–1.19) | −2.09 (−4.85–0.68) | −1.21 (−3.47–1.05) | −2.25 (−5.12–0.62) | −0.92 (−3.12–1.27) | −1.98 (−4.81–0.85) | −1.10 (−3.37–1.16) | −2.13 (−5.02–0.76) |
| Divorced/Widowed/Separated | 0.75 (−0.62–3.13) | 0.15 (−1.50–1.80) | 0.87 (−0.54–2.28) | 0.29 (−1.40–1.97) | 0.51 (−0.90–1.93) | −0.08 (−1.77–1.62) | 0.69 (−0.77–2.15) | 0.10 (−1.63–1.84) |
| Education | ||||||||
| ≤High school | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| ≥College | 1.33 (−0.30–2.96) | 0.41 (−1.42–2.24) | 1.84 (0.08–3.60) * | 0.95 (−1.02–2.92) | 1.79 (−0.002–3.58) | 0.96 (−1.03–2.95) | 1.96 (0.15–3.78) * | 1.13 (−0.91–3.16) |
| Health insurance | ||||||||
| No | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Yes | 2.00 (0.08–3.92 )* | 2.43 (0.05–4.81) * | 1.67 (−0.35–3.70) | 2.09 (−0.45–4.63) | 1.98 (−0.07–4.04) | 2.44 (−0.03–4.92) | 1.73 (−0.34–3.79) | 2.17 (−0.39–4.72) |
| Asian BMI | ||||||||
| Underweight/normal | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Overweight/obese | −0.66 (−1.71–0.40) | −0.41 (−1.58–0.75) | −0.77 (−1.86–0.32) | −0.55 (−1.76–0.65) | −0.70 (−1.78–0.39) | −0.48 (−1.67–0.72) | −0.75 (−1.85–0.34) | −0.54 (−1.75–0.67) |
| High blood pressure (BP) | ||||||||
| No | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Yes | −1.40 (−2.69–−0.11) * | −0.78 (−2.18–0.62) | −2.61 (−4.42–−0.79) * | −2.00 (−3.94–−0.05) * | −1.40 (−2.72– −0.09) * | −0.80 (−2.21–0.61) | −2.21 (−4.10– −0.32) * | −1.58 (−3.58–0.41) |
| Monitor blood pressure (BP) | ||||||||
| No | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Yes | 1.73 (0.41–3.05) * | 1.85 (0.31–3.38) * | 1.98 (0.04–4.46) * | 2.12 (0.47–3.76) * | 0.78 (−0.89–2.46) | 0.89 (−0.96–2.74) | 1.29 (−0.65–3.23) | 1.39 (−1.18–4.39) |
| Ethnic*HighBP (Kor, yes) | 2.25 (0.57–3.40) * | 2.29 (−0.18–4.76) | 1.62 (−0.88–4.13) | 1.61 (−0.73–3.51) | ||||
| Ethnic*MonitorBP (Kor, yes) | 2.14 (−0.25–4.52) | 2.39 (−0.67–5.46) | 1.25 (−1.48–3.99) | 1.49 (−1.94–4.93) | ||||
| Constant | −1.66 (−5.32–2.00) | −1.70 (−6.24–2.84) | −1.15 (−4.97–2.68) | −1.19 (−5.94–3.56) | −1.71 (−5.65–2.23) | −1.84 (−6.59–2.92) | −1.30 (−5.26–2.66) | −1.39 (−6.23–3.46) |
| Log likelihood | −105.99225 | −103.4861 | −103.89338 | −102.95915 | ||||
| Pseudo r-square | 0.1589 | 0.1788 | 0.1756 | 0.183 | ||||
| LR Chi−square (df) | 40.06 (22), p = −0.0106 | 45.07 (24), p = 0.0057 | 44.26 (24), p = 0.0071 | 46.13 (26), p = 0.0088 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhimla, A.; Gadegbeku, C.A.; Tan, Y.; Zhu, L.; Aczon, F.; Ma, G.X. A Study of Physical Activity Determinants among High-Risk Hypertensive Filipino and Korean Americans. Int. J. Environ. Res. Public Health 2019, 16, 1156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071156
Bhimla A, Gadegbeku CA, Tan Y, Zhu L, Aczon F, Ma GX. A Study of Physical Activity Determinants among High-Risk Hypertensive Filipino and Korean Americans. International Journal of Environmental Research and Public Health. 2019; 16(7):1156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071156
Chicago/Turabian StyleBhimla, Aisha, Crystal A. Gadegbeku, Yin Tan, Lin Zhu, Ferdinand Aczon, and Grace X. Ma. 2019. "A Study of Physical Activity Determinants among High-Risk Hypertensive Filipino and Korean Americans" International Journal of Environmental Research and Public Health 16, no. 7: 1156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071156