Global Brain Drain: How Can the Maslow Theory of Motivation Improve Our Understanding of Physician Migration?


Abstract
:1. Introduction
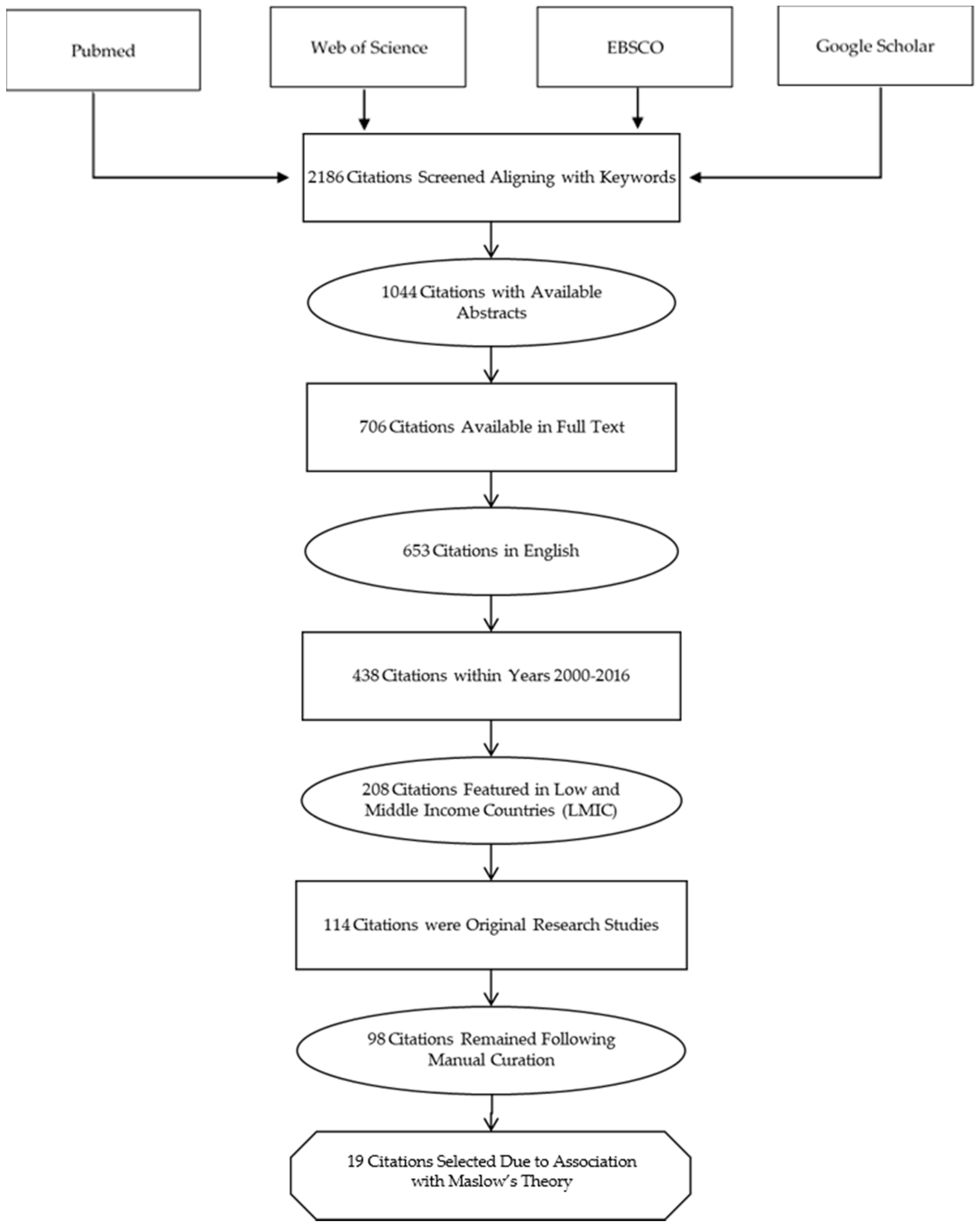
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Maslow, A.H. A theory of human motivation. Psychol. Rev. 1943, 50, 370–396. [Google Scholar] [CrossRef]
- Maslow, A.H. Toward a Psychology of Being, 3rd ed.; Wiley: New York, NY, USA, 1998; ISBN 978-0-471-29309-5. [Google Scholar]
- Crisp, N.; Chen, L. Global supply of health professionals. N. Engl. J. Med. 2014, 370, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Global Health Workforce Alliance and World Health Organization. A Universal Truth: No Health without a Workforce. Available online: https://www.who.int/workforcealliance/knowledge/resources/hrhreport2013/en/ (accessed on 17 February 2019).
- Liu, J.X.; Goryakin, Y.; Maeda, A.; Bruckner, T.; Scheffler, R. Global Health Workforce Labor Market Projections for 2030. Hum. Resour. Health 2017, 15, 11. [Google Scholar] [CrossRef]
- Moszynski, P. One billion people are affected by global shortage of healthcare workers. BMJ 2011, 342, d696. [Google Scholar] [CrossRef]
- Aluttis, C.; Bishaw, T.; Frank, M.W. The workforce for health in a globalized context—Global shortages and international migration. Glob. Health Action 2014, 7, 23611. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Report 2006—Working together for health. Available online: https://www.who.int/whr/2006/en/ (accessed on 17 February 2019).
- Clemens, M.A.; Pettersson, G. New data on African health professionals abroad. Hum. Resour. Health 2008, 6, 1. [Google Scholar] [CrossRef]
- Duvivier, R.J.; Burch, V.C.; Boulet, J.R. A comparison of physician emigration from Africa to the United States of America between 2005 and 2015. Hum. Resour. Health 2017, 15, 41. [Google Scholar] [CrossRef] [PubMed]
- Asongu, S. The Impact of Health Worker Migration on Development Dynamics: Evidence of Wealth—Effects from Africa; Social Science Research Network: Rochester, NY, USA, 2012. [Google Scholar]
- Arah, O.A. The metrics and correlates of physician migration from Africa. BMC Public Health 2007, 7, 83. [Google Scholar] [CrossRef]
- Berhan, Y. Medical doctors profile in Ethiopia: Production, attrition and retention. In memory of 100-years Ethiopian modern medicine & the new Ethiopian millennium. Ethiop. Med. J. 2008, 46 (Suppl. 1), 1–77. [Google Scholar] [PubMed]
- Bhargava, A.; Docquier, F.; Moullan, Y. Modeling the effects of physician emigration on human development. Econ. Hum. Biol. 2011, 9, 172–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosselli, D.; Otero, A.; Maza, G. Colombian physician brain drain. Med. Educ. 2001, 35, 809–810. [Google Scholar] [CrossRef]
- Morley, C.P.; Wang, D.; Mader, E.M.; Plante, K.P.; Kingston, L.N.; Rabiei, A. Analysis of the association between millennium development goals 4 & 5 and the physician workforce across international economic strata. BMC Int. Health Hum. Rights 2017, 17, 18. [Google Scholar]
- Kirigia, J.M.; Gbary, A.R.; Muthuri, L.K.; Nyoni, J.; Seddoh, A. The cost of health professionals’ brain drain in Kenya. BMC Health Serv. Res. 2006, 6, 89. [Google Scholar] [CrossRef] [PubMed]
- Shet, A.S. Physician migration: trends and long term perspectives. Natl. Med. J. India 2008, 21, 246–247. [Google Scholar]
- Mills, E.J.; Kanters, S.; Hagopian, A.; Bansback, N.; Nachega, J.; Alberton, M.; Au-Yeung, C.G.; Mtambo, A.; Bourgeault, I.L.; Luboga, S.; et al. The financial cost of doctors emigrating from sub-Saharan Africa: Human capital analysis. BMJ 2011, 343, d7031. [Google Scholar] [CrossRef] [PubMed]
- Mullan, F. The Metrics of the Physician Brain Drain. New England Journal of Medicine 2005, 353, 1810–1818. [Google Scholar] [CrossRef] [PubMed]
- Salafsky, B.; Glasser, M.; Ha, J. Addressing issues of maldistribution of health care workers. Ann. Acad. Med. Singap. 2005, 34, 520–526. [Google Scholar] [PubMed]
- Halbeis, C.B.E.; Cvachovec, K.; Scherpereel, P.; Mellin-Olsen, J.; Drobnik, L.; Sondore, A. Anaesthesia workforce in Europe. Eur. J. Anaesthesiol. 2007, 24, 991–1007. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.J. The role and contributions of IMGs: A U.S. perspective. Acad. Med. 2006, 81, S17–S21. [Google Scholar] [CrossRef]
- Baerlocher, M.O. The importance of foreign-trained physicians to Canada. Clin. Invest. Med. 2006, 29, 151–153. [Google Scholar]
- Hussey, P.S. International migration patterns of physicians to the United States: A cross-national panel analysis. Health Policy 2007, 84, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Goodman, D.C.; Fisher, E.S. Physician workforce crisis? Wrong diagnosis, wrong prescription. N. Engl. J. Med. 2008, 358, 1658–1661. [Google Scholar] [CrossRef]
- Mbemba, G.I.C.; Gagnon, M.-P.; Hamelin-Brabant, L. Factors Influencing Recruitment and Retention of Healthcare Workers in Rural and Remote Areas in Developed and Developing Countries: An Overview. J. Public Health Africa 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Klein, D.; Hofmeister, M.; Lockyear, J.; Crutcher, R.; Fidler, H. Push, pull, and plant: the personal side of physician immigration to alberta, Canada. Fam. Med. 2009, 41, 197–201. [Google Scholar] [PubMed]
- Goodell, A.J.; Kahn, J.G.; Ndeki, S.S.; Kaale, E.; Kaaya, E.E.; Macfarlane, S.B.J. Modeling solutions to Tanzania’s physician workforce challenge. Glob. Health Action 2016, 9, 31597. [Google Scholar] [CrossRef]
- Aluwihare, A.P.R. Physician migration: Donor country impact. J. Contin. Educ. Health Prof. 2005, 25, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Word Health Organization. Managing health workforce migration—The Global Code of Practice. Available online: http://www.who.int/hrh/migration/code/practice/en/ (accessed on 17 February 2019).
- Holmes, G.M.; Fraher, E.P. Developing Physician Migration Estimates for Workforce Models. Health Serv. Res. 2017, 52 (Suppl. 1), 529–545. [Google Scholar] [CrossRef] [Green Version]
- Suciu, Ş.M.; Popescu, C.A.; Ciumageanu, M.D.; Buzoianu, A.D. Physician migration at its roots: A study on the emigration preferences and plans among medical students in Romania. Hum. Resour. Health 2017, 15, 6. [Google Scholar] [CrossRef]
- Tankwanchi, A.B.S.; Vermund, S.H.; Perkins, D.D. Monitoring Sub-Saharan African physician migration and recruitment post-adoption of the WHO code of practice: Temporal and geographic patterns in the United States. PLoS ONE 2015, 10, e0124734. [Google Scholar] [CrossRef]
- Tankwanchi, A.B.S.; Özden, Ç.; Vermund, S.H. Physician Emigration from Sub-Saharan Africa to the United States: Analysis of the 2011 AMA Physician Masterfile. PLoS Med. 2013, 10, e1001513. [Google Scholar] [CrossRef]
- Akl, E.A.; Maroun, N.; Major, S.; Afif, C.; Abdo, A.; Choucair, J.; Sakr, M.; Li, C.K.; Grant, B.J.; Schünemann, H.J. Post-graduation migration intentions of students of Lebanese medical schools: A survey study. BMC Public Health 2008, 8, 191. [Google Scholar] [CrossRef] [PubMed]
- Akl, E.A.; Maroun, N.; Major, S.; Afif, C.; Chahoud, B.; Choucair, J.; Sakr, M.; Schünemann, H.J. Why are you draining your brain? Factors underlying decisions of graduating Lebanese medical students to migrate. Soc. Sci. Med. 2007, 64, 1278–1284. [Google Scholar] [CrossRef]
- Okeke, E.N. Do higher salaries lower physician migration? Health Policy Plan 2014, 29, 603–614. [Google Scholar] [CrossRef]
- Okeke, E.N. Brain drain: Do economic conditions “push” doctors out of developing countries? Soc. Sci. Med. 2013, 98, 169–178. [Google Scholar] [CrossRef]
- Sheikh, A.; Naqvi, S.H.A.; Sheikh, K.; Naqvi, S.H.S.; Bandukda, M.Y. Physician migration at its roots: A study on the factors contributing towards a career choice abroad among students at a medical school in Pakistan. Glob. Health 2012, 8, 43. [Google Scholar] [CrossRef]
- de Silva, N.L.; Samarasekara, K.; Rodrigo, C.; Samarakoon, L.; Fernando, S.D.; Rajapakse, S. Why do doctors emigrate from Sri Lanka? A survey of medical undergraduates and new graduates. BMC Res. Notes 2014, 7, 918. [Google Scholar] [CrossRef] [PubMed]
- Bojanic, A.; Bojanic, K.; Likic, R. Brain drain: Final year medical students’ intentions of training abroad. Postgrad. Med. J. 2015, 91, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Burnham, G.; Malik, S.; Al-Shibli, A.S.D.; Mahjoub, A.R.; Baqer, A.Q.; Baqer, Z.Q.; Al Qaraghuli, F.; Doocy, S. Understanding the impact of conflict on health services in Iraq: Information from 401 Iraqi refugee doctors in Jordan. Int. J. Health Plan. Manag. 2012, 27, e51–e64. [Google Scholar] [CrossRef]
- Deressa, W.; Azazh, A. Attitudes of undergraduate medical students of Addis Ababa University towards medical practice and migration, Ethiopia. BMC Med. Educ. 2012, 12, 68. [Google Scholar] [CrossRef] [PubMed]
- Hossain, N.; Shah, N.; Shah, T.; Lateef, S.B. Physicians’ Migration: Perceptions of Pakistani Medical Students. J. Coll. Physicians Surg. Pak. 2016, 26, 696–701. [Google Scholar]
- Rao, N.R.; Rao, U.K.; Cooper, R.A. Indian medical students’ views on immigration for training and practice. Acad. Med. 2006, 81, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Fouad, Y.A.; Fahmy, Y.M.; Abdel Hady, S.M.; Elsabagh, A.E. Egyptian future physicians are packing to leave but may be willing to return. Int. Health 2015, 7, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Kizito, S.; Mukunya, D.; Nakitende, J.; Nambasa, S.; Nampogo, A.; Kalyesubula, R.; Katamba, A.; Sewankambo, N. Career intentions of final year medical students in Uganda after graduating: The burden of brain drain. BMC Med. Educ. 2015, 15, 122. [Google Scholar] [CrossRef]
- Bailey, N.; Mandeville, K.L.; Rhodes, T.; Mipando, M.; Muula, A.S. Postgraduate career intentions of medical students and recent graduates in Malawi: A qualitative interview study. BMC Med. Educ. 2012, 12, 87. [Google Scholar] [CrossRef]
- Eliason, S.; Tuoyire, D.A.; Awusi-Nti, C.; Bockarie, A.S. Migration intentions of Ghanaian medical students: The influence of existing funding mechanisms of medical education (“the fee factor”). Ghana Med. J. 2014, 48, 78–84. [Google Scholar] [CrossRef]
- Gouda, P.; Kitt, K.; Evans, D.S.; Goggin, D.; McGrath, D.; Last, J.; Hennessy, M.; Arnett, R.; O’Flynn, S.; Dunne, F.; et al. Ireland’s medical brain drain: Migration intentions of Irish medical students. Hum. Resour. Health 2015, 13, 11. [Google Scholar] [CrossRef]
- Silvestri, D.M.; Blevins, M.; Afzal, A.R.; Andrews, B.; Derbew, M.; Kaur, S.; Mipando, M.; Mkony, C.A.; Mwachaka, P.M.; Ranjit, N.; et al. Medical and nursing students’ intentions to work abroad or in rural areas: A cross-sectional survey in Asia and Africa. Bull. World Health Organ. 2014, 92, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Imran, N.; Azeem, Z.; Haider, I.I.; Amjad, N.; Bhatti, M.R. Brain Drain: Post Graduation Migration Intentions and the influencing factors among Medical Graduates from Lahore, Pakistan. BMC Res. Notes 2011, 4, 417. [Google Scholar] [CrossRef] [PubMed]
- Lakhey, M.; Lakhey, S.; Niraula, S.R.; Jha, D.; Pant, R. Comparative attitude and plans of the medical students and young Nepalese doctors. Kathmandu Univ. Med. J. 2009, 7, 177–182. [Google Scholar] [CrossRef]
- Kotha, S.R.; Johnson, J.C.; Galea, S.; Agyei-Baffour, P.; Nakua, E.; Asabir, K.; Kwansah, J.; Gyakobo, M.; Dzodzomenyo, M.; Kruk, M.E. Lifecourse factors and likelihood of rural practice and emigration: A survey of Ghanaian medical students. Rural Remote Health 2012, 12, 1898. [Google Scholar]
- Burch, V.C.; McKinley, D.; van Wyk, J.; Kiguli-Walube, S.; Cameron, D.; Cilliers, F.J.; Longombe, A.O.; Mkony, C.; Okoromah, C.; Otieno-Nyunya, B.; et al. Career intentions of medical students trained in six sub-Saharan African countries. Educ. Health (Abingdon) 2011, 24, 614. [Google Scholar]
- Wells, K.M.; Shalabi, H.; Sergelen, O.; Wiessner, P.; Zhang, C.; deVries, C.; Price, R. Patient and Physician Perceptions of Changes in Surgical Care in Mongolia 9 Years After Roll-out of a National Training Program for Laparoscopy. World J. Surg. 2016, 40, 1859–1864. [Google Scholar] [CrossRef] [PubMed]
- Talati, J.J.; Pappas, G. Migration, medical education, and health care: A view from Pakistan. Acad. Med. 2006, 81, S55–S62. [Google Scholar] [CrossRef]
- Burnham, G.M.; Lafta, R.; Doocy, S. Doctors leaving 12 tertiary hospitals in Iraq, 2004–2007. Soc. Sci. Med. 2009, 69, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Al-Kindi, S. Violence against doctors in Iraq. Lancet 2014, 384, 954–955. [Google Scholar] [CrossRef]
- Bidwell, P.; Laxmikanth, P.; Blacklock, C.; Hayward, G.; Willcox, M.; Peersman, W.; Moosa, S.; Mant, D. Security and skills: The two key issues in health worker migration. Glob. Health Action 2014, 7, 24194. [Google Scholar] [CrossRef]
- Bhargava, A.D. Frédéric HIV Pandemic, Medical Brain Drain, and Economic Development in Sub-Saharan Africa. World Bank Econ. Rev. 2008, 22, 345–366. [Google Scholar] [CrossRef]
- Wu, L.X.; Qi, L.; Li, Y. Challenges faced by young Chinese doctors. Lancet 2016, 387, 1617. [Google Scholar] [CrossRef]
- Assefa, T.; Haile Mariam, D.; Mekonnen, W.; Derbew, M.; Enbiale, W. Physician distribution and attrition in the public health sector of Ethiopia. Risk Manag. Healthc. Policy 2016, 9, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Hagopian, A.; Thompson, M.J.; Fordyce, M.; Johnson, K.E.; Hart, L.G. The migration of physicians from sub-Saharan Africa to the United States of America: Measures of the African brain drain. Hum. Resour. Health 2004, 2, 17. [Google Scholar] [CrossRef]
- Astor, A.; Akhtar, T.; Matallana, M.A.; Muthuswamy, V.; Olowu, F.A.; Tallo, V.; Lie, R.K. Physician migration: Views from professionals in Colombia, Nigeria, India, Pakistan and the Philippines. Soc. Sci. Med. 2005, 61, 2492–2500. [Google Scholar] [CrossRef]
- Starkiene, L.; Smigelskas, K.; Padaiga, Z.; Reamy, J. The future prospects of Lithuanian family physicians: A 10-year forecasting study. BMC Fam. Pract. 2005, 6, 41. [Google Scholar] [CrossRef]
- Stilwell, B.; Diallo, K.; Zurn, P.; Vujicic, M.; Adams, O.; Dal Poz, M. Migration of health-care workers from developing countries: Strategic approaches to its management. Bull. World Health Organ. 2004, 82, 595–600. [Google Scholar] [PubMed]
- Sherr, K.; Mussa, A.; Chilundo, B.; Gimbel, S.; Pfeiffer, J.; Hagopian, A.; Gloyd, S. Brain drain and health workforce distortions in Mozambique. PLoS ONE 2012, 7, e35840. [Google Scholar] [CrossRef] [PubMed]
- Opoku, S.T.; Apenteng, B.A. Seeking greener pastures? The relationship between career satisfaction and the intention to emigrate: A survey of Ghanaian physicians. Int. Health 2014, 6, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Raghuram, P. Situating women in the brain drain discourse: Discursive challenges and opportunities. In Gender and Migration in 21st Century Europe; Stalford, H., Currie, S., Velluti, S., Eds.; Ashgate: Aldershot, UK, 2009; pp. 85–106. ISBN 978-0-7546-7450-4. [Google Scholar]
- Dodani, S.; LaPorte, R.E. Ways to strengthen research capacity in developing countries: Effectiveness of a research training workshop in Pakistan. Public Health 2008, 122, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Kingsnorth, A.; Gyoh, S. Is it possible to train surgeons for rural Africa? A report of a successful international program. World J. Surg. 2012, 36, 1439–1440. [Google Scholar] [CrossRef]
- Chuang, L.; Moore, K.N.; Creasman, W.T.; Goodman, A.; Henriquez Cooper, H.; Price, F.V.; Conner, M.G.; Gupta, V.; Gallion, H.H.; Husseinzadeh, N.; et al. Teaching gynecologic oncology in Low resource settings: A collaboration of health volunteers overseas and the society of gynecologic oncology. Gynecol. Oncol. 2014, 135, 580–582. [Google Scholar] [CrossRef]
- Omaswa, F.G. The contribution of the Medical Education Partnership Initiative to Africa’s renewal. Acad. Med. 2014, 89, S16–S18. [Google Scholar] [CrossRef]
- Stuart-Shor, E.M.; Cunningham, E.; Foradori, L.; Hutchinson, E.; Makwero, M.; Smith, J.; Kasozi, J.; Johnston, E.M.; Khaki, A.; Vandervort, E.; et al. The Global Health Service Partnership: An Academic-Clinical Partnership to Build Nursing and Medical Capacity in Africa. Front. Public Health 2017, 5, 174. [Google Scholar] [CrossRef]
- Alem, A.; Pain, C.; Araya, M.; Hodges, B.D. Co-creating a psychiatric resident program with Ethiopians, for Ethiopians, in Ethiopia: The Toronto Addis Ababa Psychiatry Project (TAAPP). Acad. Psychiatry 2010, 34, 424–432. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Ref. | Study Population | Study Sample | Percentage with the Intention to Leave | Reasons to Emigrate | The Equivalent on Maslow Theory |
|---|---|---|---|---|---|
| [51] | Ireland | 1519 (medical trainees) | 88% | career opportunities (85%), working conditions (83%), lifestyle (80%). | Self-actualization Esteem |
| [47] | Egypt | 940 (students) | 85.7% (81.8% plan to return) | better research opportunities (mean 4.74) working conditions (mean 4.64) | Self-actualization |
| [48] | Uganda | 251 | 44.6% | “doctors are paid a high salary abroad, safe working environment, and the desire to continue academics.” | Safety needs Self-actualization Esteem |
| [52] | Bangladesh, Ethiopia, India, Kenya, Malawi, Nepal, Tanzania and Zambia | 3156 (medical and nursing students) | 28% | educational opportunities, monetary opportunities | Safety needs Self-actualization Esteem |
| [49] | Malawi | 12 (medical students) | All participants intended to work in Malawi in the long term, after a period outside the country. | “[T] his was in the pursuit of postgraduate study rather than higher salaries. In general, medical students and young doctors were enthusiastic about working at district level, although this is curtailed by their desire for specialist training and frustration with resource shortages.” | Self-actualization Esteem |
| [42] | Croatia | 232 | 53% for specialty (26%) or subspecialty (27%) training | excel professionally (38%), prosper financially (17%), and acquire new experiences and international exposure (26%). | Safety needs Self-actualization Esteem |
| [44] | Ethiopia | 600 (medical students) | 53% of the students | “improving the quality of education and career choice satisfaction, creating conducive training and working conditions.” | Safety needs Self-actualization Esteem |
| [53] | Pakistan | 275 (medical students) | 60.4%; 14.2% intended to return to Pakistan immediately after training; 10% never intended to go back to Pakistan or wished to stay abroad temporarily (37%). | the impact of training on future career (mean score 8.20 ± 2.3), financial conditions of doctors (mean score 7.97 ± 2.37), and job opportunities (mean score7.90 ± 2.34). | Safety needs Self-actualization Esteem |
| [36] | Lebanon | 425 (medical students) | 95.5%; 25.1% respondents intended to return to Lebanon directly after finishing training abroad; 63.8% intended to return to Lebanon after working abroad temporarily for a varying number or years; 10.6% intended to never return to Lebanon. | training perspective | Self-actualization |
| [56] | Democratic Republic of Congo, Kenya, Nigeria, Tanzania and Uganda | 990 (medical students) | Many students (40%) planned to train abroad. | Career-related factors favoring retention in Africa were career options and the quality and availability of training opportunities. The top personal factors for staying in Africa were a desire to improve medicine in Africa, personal safety, social conditions, and family issues. The top career-related factors favoring relocation outside Africa were remuneration, access to equipment and advanced technology, career and training opportunities, a regulated work environment, and the politics of health care in Africa. The top personal factors favoring relocation outside Africa were personal safety, the opportunity for experience in a different environment, social conditions, and greater personal freedom. | Self-transcendence Self-actualization Social belonging Safety needs Food shelter |
| [55] | Ghana | 282 | 64.9% had considered emigrating after graduation. | Consideration of emigration was predicted by having lived abroad but never in a rural area (OR: 3.39, 95%CI: 1.15–9.97). | Social belonging |
| [54] | Nepal | 265 (student, interns, and house officers) | 40% of students, 58% of interns, and 48% of house officers | Improving career opportunities or the working environment of the doctor could make the profession more attractive. | Self-actualization Esteem |
| [46] | India | 260 (medical students) | 59% intend to leave for training. | While more than 60% perceived greater professional opportunities in the United States than in India, approximately 75% were concerned that the United States had become less welcoming after the terrorist attacks of 9/11, and similar numbers were concerned about the examination administered by the Educational Commission on Foreign Medical Graduates. Conversely, the majority of respondents felt that opportunities for physicians in India were improving. | Self-actualization, Safety needs |
| [41] | Sri Lanka | 374 (students, pre-interns) | 23.8% | better quality of life, better earnings, and more training opportunities | Self-actualization Esteem Safety needs |
| [43] | Iraq | 1243 (physicians) | 61% left the country. | safety, security, poor financial conditions | Safety needs Food and shelter |
| [45] | Pakistan | 240 (students, interns) | 54% | 48%: postgraduate education, 35.2%: economic prospects, 92.5%: weak medical system, 78.5%: religious intolerance | Safety needs Self-actualization Esteem |
| [40] | Pakistan | 323 (students) | 60.4% | lucrative salary, quality of training, job satisfaction better way of life, relatives, and domestic terrorism | Self-actualization Esteem Social belonging Safety needs |
| [31] | Romania | 957 (students) | 84.7% | earning potential, better life | Safety needs Self-actualization Esteem |
| [57] | Mongolia | 39 (physicians) | 26% | insufficient equipment supply training funding | Self-actualization |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dohlman, L.; DiMeglio, M.; Hajj, J.; Laudanski, K. Global Brain Drain: How Can the Maslow Theory of Motivation Improve Our Understanding of Physician Migration? Int. J. Environ. Res. Public Health 2019, 16, 1182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071182
Dohlman L, DiMeglio M, Hajj J, Laudanski K. Global Brain Drain: How Can the Maslow Theory of Motivation Improve Our Understanding of Physician Migration? International Journal of Environmental Research and Public Health. 2019; 16(7):1182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071182
Chicago/Turabian StyleDohlman, Lena, Matthew DiMeglio, Jihane Hajj, and Krzysztof Laudanski. 2019. "Global Brain Drain: How Can the Maslow Theory of Motivation Improve Our Understanding of Physician Migration?" International Journal of Environmental Research and Public Health 16, no. 7: 1182. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071182