Theory Content, Question-Behavior Effects, or Form of Delivery Effects for Intention to Become an Organ Donor? Two Randomized Trials

 ,
,  ,
, 
Abstract
:1. Introduction
- -
- To replicate the findings of Doherty et al. [1], by determining whether intention to donate was different among groups exposed to differential levels of affective attitudes, when using a similar number of questionnaire items in each exposure
- -
- Determine whether findings were similar in different countries and cultures
- -
- Ascertain whether results are similar with face-to-face or web-based methodologies
2. Materials and Methods
2.1. Context
2.2. Trial Design
2.3. Participants
2.4. Interventions and Procedures
- -
- Group 1: No-intervention replication group, who completed the entire questionnaire (similar to the anticipated regret group from INORDAR), replicating methods of O’Carroll et al. [3].
- -
- Group 2: Omitted affective attitudes group. All 16 questions on affective attitudes were deleted, with dummy questions (e.g., about politics) substituted for these deleted questions (as in the INORDAR trial).
- -
- Group 3: Omitted 12 negatively-worded affective attitudes only, which were substituted with the same questions as Group 2.
2.5. Materials/Measures
- -
- UK: “I will definitely register for organ donation in the next few months”
- -
- Non-UK: “I will definitely sign up for organ donation and discuss this with my family in the next few months”
2.6. Procedures
2.7. Outcomes
2.8. Sample Size
2.9. Randomization
2.10. Statistical Methods
3. Results
3.1. Participant Profile
3.2. Outcomes
3.3. Ancillary Analyses
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
 | CONSORT 2010 checklist of information to include when reporting a randomised trial *. |

{kind=link}
| Section/Topic | Item No | Checklist Item | Reported on Page No |
|---|---|---|---|
| Title and abstract | |||
| 1a | Identification as a randomised trial in the title | 1 | |
| 1b | Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) | 1 (non-structured as per journal requirements) | |
| Introduction | |||
| Background and objectives | 2a | Scientific background and explanation of rationale | 1–3 |
| 2b | Specific objectives or hypotheses | 3 | |
| Methods | |||
| Trial design | 3a | Description of trial design (such as parallel, factorial) including allocation ratio | 3 |
| 3b | Important changes to methods after trial commencement (such as eligibility criteria), with reasons | 3 | |
| Participants | 4a | Eligibility criteria for participants | 3–4 |
| 4b | Settings and locations where the data were collected | 3,5 | |
| Interventions | 5 | The interventions for each group with sufficient details to allow replication, including how and when they were actually administered | 4–5, TIDIeR checklist |
| Outcomes | 6a | Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed | 5 |
| 6b | Any changes to trial outcomes after the trial commenced, with reasons | No changes | |
| Sample size | 7a | How sample size was determined | 5 |
| 7b | When applicable, explanation of any interim analyses and stopping guidelines | Not applicable | |
| Randomisation: | |||
| Sequence generation | 8a | Method used to generate the random allocation sequence | 5–6 |
| 8b | Type of randomisation; details of any restriction (such as blocking and block size) | 5–6 | |
| Allocation concealment mechanism | 9 | Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned | 5–6 |
| Implementation | 10 | Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions | 5–6 |
| Blinding | 11a | If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how | 5–6 |
| 11b | If relevant, description of the similarity of interventions | 4 | |
| Statistical methods | 12a | Statistical methods used to compare groups for primary and secondary outcomes | 6 |
| 12b | Methods for additional analyses, such as subgroup analyses and adjusted analyses | 6 | |
| Results | |||
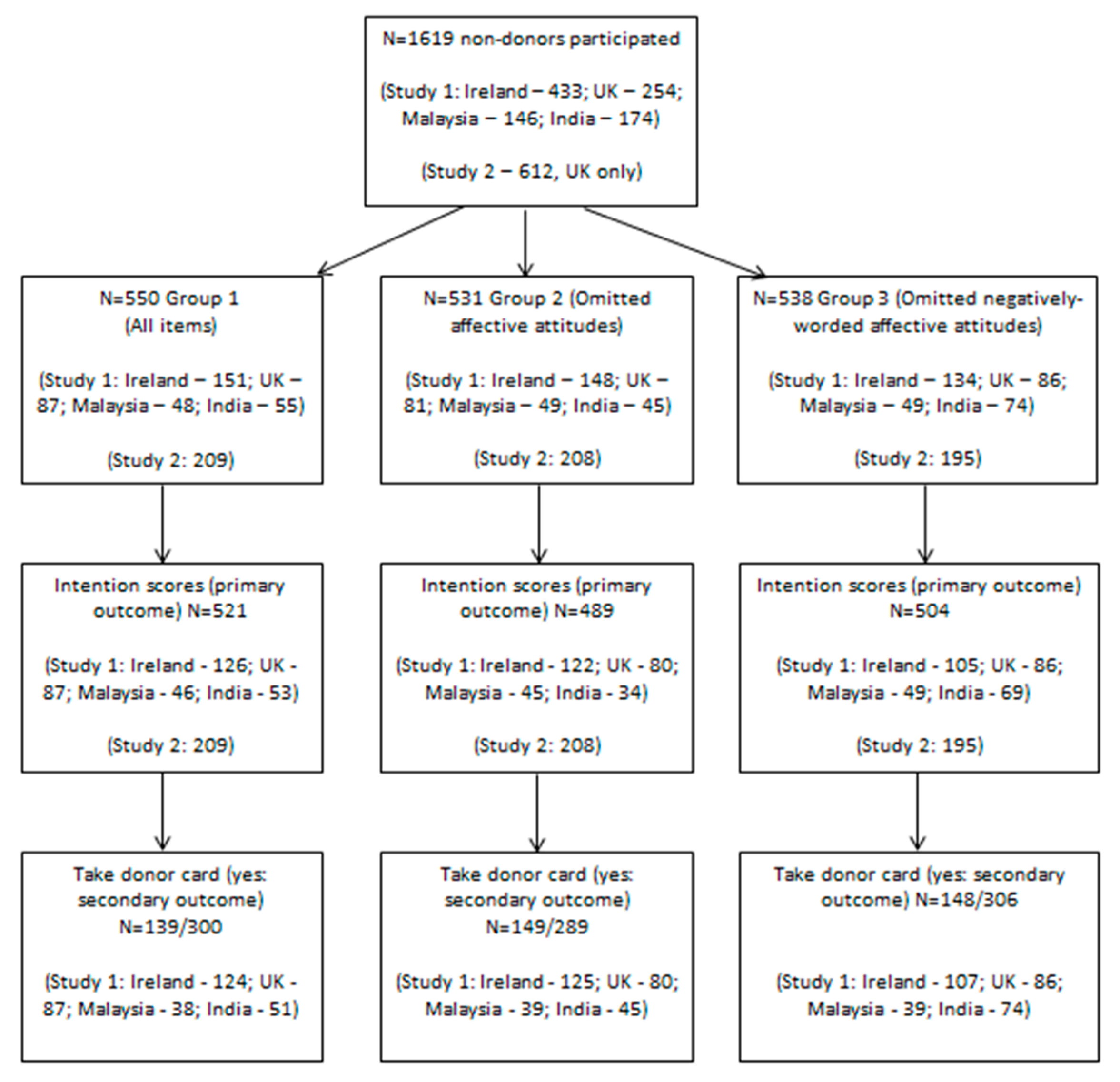
| Participant flow (a diagram is strongly recommended) | 13a | For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analysed for the primary outcome | 7—Figure 1 |
| 13b | For each group, losses and exclusions after randomisation, together with reasons | 7—Figure 1 | |
| Recruitment | 14a | Dates defining the periods of recruitment and follow-up | 5 |
| 14b | Why the trial ended or was stopped | Not applicable | |
| Baseline data | 15 | A table showing baseline demographic and clinical characteristics for each group | 8—Table 1, 21—Appendix |
| Numbers analysed | 16 | For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups | 6,7—Figure 1 |
| Outcomes and estimation | 17a | For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval) | 11 10—Table 2 12—Table 3 |
| 17b | For binary outcomes, presentation of both absolute and relative effect sizes is recommended | 10 10—Table 2 12—Table 3 | |
| Ancillary analyses | 18 | Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre-specified from exploratory | 11 12—Table 3 |
| Harms | 19 | All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) | Not applicable |
| Discussion | |||
| Limitations | 20 | Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses | 14 |
| Generalisability | 21 | Generalisability (external validity, applicability) of the trial findings | 13 |
| Interpretation | 22 | Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence | 13–14 |
| Other information | |||
| Registration | 23 | Registration number and name of trial registry | 3 |
| Protocol | 24 | Where the full trial protocol can be accessed, if available | Not applicable |
| Funding | 25 | Sources of funding and other support (such as supply of drugs), role of funders | 14 |
Appendix B
 | The TIDieR (Template for Intervention Description and Replication) Checklist *: |
| Item Number | Item | Where Located ** | |
|---|---|---|---|
| Primary Paper (Page or Appendix Number) | Other † (Details) | ||
| BRIEF NAME | |||
| 1. | Provide the name or a phrase that describes the intervention. | n/a | _____________ |
| WHY | |||
| 2. | Describe any rationale, theory, or goal of the elements essential to the intervention. | 2–5 | _____________ |
| WHAT | |||
| 3. | Materials: Describe any physical or informational materials used in the intervention, including those provided to participants or used in intervention delivery or in training of intervention providers. Provide information on where the materials can be accessed (e.g., online appendix, URL). | 4–5 | _____________ |
| 4. | Procedures: Describe each of the procedures, activities, and/or processes used in the intervention, including any enabling or support activities. | 5 | _____________ |
| WHO PROVIDED | |||
| 5. | For each category of intervention provider (e.g., psychologist, nursing assistant), describe their expertise, background and any specific training given. | 5–6 | _____________ |
| HOW | |||
| 6. | Describe the modes of delivery (e.g., face-to-face or by some other mechanism, such as internet or telephone) of the intervention and whether it was provided individually or in a group. | 5–6 | _____________ |
| WHERE | |||
| 7. | Describe the type(s) of location(s) where the intervention occurred, including any necessary infrastructure or relevant features. | 5–6 | _____________ |
| WHEN and HOW MUCH | |||
| 8. | Describe the number of times the intervention was delivered and over what period of time including the number of sessions, their schedule, and their duration, intensity or dose. | 5–6 | _____________ |
| TAILORING | |||
| 9. | If the intervention was planned to be personalised, titrated or adapted, then describe what, why, when, and how. | 4 | _____________ |
| MODIFICATIONS | |||
| 10. ǂ | If the intervention was modified during the course of the study, describe the changes (what, why, when, and how). | Not applicable | Recruitment location modified as per 2.2 |
| HOW WELL | |||
| 11. | Planned: If intervention adherence or fidelity was assessed, describe how and by whom, and if any strategies were used to maintain or improve fidelity, describe them. | 5—not assessed | _____________ |
| 12. ǂ | Actual: If intervention adherence or fidelity was assessed, describe the extent to which the intervention was delivered as planned. | Not assessed | _____________ |
Appendix C
| Ireland, All Groups | Group 1 | Group 2 | Group 3 | UK, All Groups | Group 1 | Group 2 | Group 3 | Malaysia, All Groups | Group 1 | Group 2 | Group 3 | India, All Groups | Group 1 | Group 2 | Group 3 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (mean, SD) | 37.1 (17.7) | 36.9 (17.4) | 36.7 (17.4) | 37.6 (18.5) | 46.1 (18.8) | 45.3 (19.0) | 46.8 (19.3) | 46.1 (18.3) | 19.7 (4.17) | 19.5 (4.19) | 20.0 (4.25) | 19.6 (4.14) | 22.6 (6.67) | 24.2 (8.72) | 22.8 (5.50) | 21.4 (5.18) |
| Women | 45.8% | 44.4% | 44.2% | 49.3% | 46.1% | 39.1% | 45.7% | 54.7% | 65.7% | 56.3% | 69.4% | 71.4% | 76.2% | 81.8% | 84.1% | 67.1% |
| Private health insurance † | 67.1% | 63.4% | 59.7% | 83% | † | † | † | † | 39.3% | 38.3% | 42.6% | 37.0% | 24.1% | 30.9% | 13.3% | 25.7% |
| Do you know someone who (% yes) | ||||||||||||||||
| has received an organ | 21.0% | 20% | 20% | 31% | 13.0% | 11.5% | 12.4% | 15.1% | 15.8% | 8.33% | 20.4% | 18.4% | 20.7% | 26% | 26.8% | 13.7% |
| needs an organ | 16.1% | 15.2% | 14.6% | 18.8% | 5.1% | 2.3% | 9.88% | 3.49% | 16.4% | 14.6% | 18.4% | 16.3% | 7.69% | 3.7% | 11.9% | 8.22% |
| has donated an organ | 12.8% | 12.6% | 15.2% | 10.5% | 8.27% | 4.6% | 9.88% | 10.5% | 11.0% | 8.33% | 14.3% | 10.2% | 23.0% | 26.0% | 26.2% | 19.2% |
| Ever donated blood | 37.2% | 34.4% | 38.2% | 39.1% | 46.9% | 46.0% | 48.2% | 46.5% | 24.7% | 27.1% | 34.7% | 12.2% | 18.2% | 14.6% | 16.7% | 21.9% |
References
- Doherty, S.; Dolan, E.; Flynn, J.; O’Carroll, R.E.; Doyle, F. Circumventing the ‘ick’ factor: A randomised trial of the effects of omitting affective attitudes questions to increase intention to become an organ donor. Front. Psychol. 2017, 8, 1443. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.E.; Stephenson, M.T.; Harrison, T.R.; Afifi, W.A.; Long, S.D. Facts versus ‘Feelings’: How rational is the decision to become an organ donor? J. Health Psychol. 2008, 13, 644–658. [Google Scholar] [CrossRef]
- O’Carroll, R.E.; Foster, C.; McGeechan, G.; Sandford, K.; Ferguson, E. The “ick” factor, anticipated regret, and willingness to become an organ donor. Health Psychol. 2011, 30, 236–245. [Google Scholar] [CrossRef]
- O’Carroll, R.E.; Ferguson, E.; Hayes, P.C.; Shepherd, L. Increasing organ donation via anticipated regret (INORDAR): Protocol for a randomised controlled trial. BMC Public Health 2012, 12, 169. [Google Scholar] [CrossRef] [PubMed]
- O’Carroll, R.E.; Shepherd, L.; Hayes, P.C.; Ferguson, E. Anticipated regret and organ donor registration: A randomized controlled trial. Health Psychol. 2016, 35, 1169–1177. [Google Scholar] [CrossRef] [PubMed]
- Kahneman, D. Thinking, Fast and Slow; Penguin: London, UK, 2011. [Google Scholar]
- Sprott, D.E.; Spangenberg, E.R.; Knuff, D.C.; Devezer, B. Self-prediction and patient health: Influencing health-related behaviors through self-prophecy. Med. Sci. Monit. 2006, 12, RA85–RA91. [Google Scholar] [PubMed]
- Wilding, S.; Conner, M.; Sandberg, T.; Prestwich, A.; Lawton, R.; Wood, C.; Miles, E.; Godin, G.; Sheeran, P. The question-behaviour effect: A theoretical and methodological review and meta-analysis. Eur. Rev. Soc. Psychol. 2016, 27, 196–230. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; O’Brien, N.; French, D.P.; Glidewell, L.; Sniehotta, F.F. The question-behavior effect: Genuine effect or spurious phenomenon? A systematic review of randomized controlled trials with meta-analyses. Health Psychol. 2015, 34, 61–78. [Google Scholar] [CrossRef]
- Nichols, A.L.; Maner, J.K. The good-subject effect: Investigating participant demand characteristics. J. Gen. Psychol. 2008, 135, 151–165. [Google Scholar] [CrossRef]
- Perinelli, E.; Gremigni, P. Use of Social Desirability Scales in Clinical Psychology: A Systematic Review. J. Clin. Psychol. 2016, 72, 534–551. [Google Scholar] [CrossRef]
- Bou Malham, P.; Saucier, G. The conceptual link between social desirability and cultural normativity. Int. J. Psychol. 2016, 51, 474–480. [Google Scholar] [CrossRef]
- Dombrowski, S.U.; O’Carroll, R.E.; Williams, B. Form of delivery as a key ‘active ingredient’ in behaviour change interventions. Br. J. Health Psychol. 2016, 21, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Tate, D.F.; Gorin, A.A.; Raynor, H.A.; Fava, J.L. A self-regulation program for maintenance of weight loss. N. Engl. J. Med. 2006, 355, 1563–1571. [Google Scholar] [CrossRef]
- Murphy, R.; Hutton, P. Practitioner Review: Therapist variability, patient-reported therapeutic alliance, and clinical outcomes in adolescents undergoing mental health treatment—A systematic review and meta-analysis. J. Child Psychol. Psychiatry 2018, 59, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Del Re, A.C.; Fluckiger, C.; Horvath, A.O.; Symonds, D.; Wampold, B.E. Therapist effects in the therapeutic alliance-outcome relationship: A restricted-maximum likelihood meta-analysis. Clin. Psychol. Rev. 2012, 32, 642–649. [Google Scholar] [CrossRef]
- Kemmelmeier, M. Cultural differences in survey responding: Issues and insights in the study of response biases. Int. J. Psychol. 2016, 51, 439–444. [Google Scholar] [CrossRef]
- Smith, P.B.; Vignoles, V.L.; Becker, M.; Owe, E.; Easterbrook, M.J.; Brown, R.; Bourguignon, D.; Garðarsdóttir, R.B.; Kreuzbauer, R.; Ayala, B.C.; et al. Individual and culture-level components of survey response styles: A multi-level analysis using cultural models of selfhood. Int. J. Psychol. 2016, 51, 453–463. [Google Scholar] [CrossRef]
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P.; Group, C. Methods and processes of the CONSORT Group: Example of an extension for trials assessing nonpharmacologic treatments. Ann. Intern. Med. 2008, 148, W60–W66. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- O’Carroll, R.E.; Haddow, L.; Foley, L.; Quigley, J. If you needed an organ transplant would you have one? The effect of reciprocity priming and mode of delivery on organ donor registration intentions and behaviour. Br. J. Health Psychol. 2017, 22, 577–588. [Google Scholar] [CrossRef]
- De Boer, M.R.; Waterlander, W.E.; Kuijper, L.D.; Steenhuis, I.H.; Twisk, J.W. Testing for baseline differences in randomized controlled trials: An unhealthy research behavior that is hard to eradicate. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 4. [Google Scholar] [CrossRef]
- Landry, C.E.; Lange, A.; List, J.A.; Price, M.K.; Rupp, N.G. Toward an understanding of the economics of charity: Evidence from a field experiment. Q. J. Econ. 2006, 121, 747–782. [Google Scholar] [CrossRef]
- Brose, L.S.; McEwen, A.; West, R. Does it matter who you see to help you stop smoking? Short-term quit rates across specialist stop smoking practitioners in England. Addiction 2012, 107, 2029–2036. [Google Scholar] [CrossRef]
- Gainforth, H.L.; Aujla, S.Y.; Beard, E.; Croghan, E.; West, R. Associations between Practitioner Personality and Client Quit Rates in Smoking Cessation Behavioural Support Interventions. J. Smok. Cessat. 2017, 13, 103–109. [Google Scholar] [CrossRef]
- Falomir-Pichastor, J.M.; Berent, J.A.; Pereira, A. Social psychological factors of post-mortem organ donation: A theoretical review of determinants and promotion strategies. Health Psychol. Rev. 2013, 7, 202–247. [Google Scholar] [CrossRef]
- Shrout, P.E.; Stadler, G.; Lane, S.P.; McClure, M.J.; Jackson, G.L.; Clavél, F.D.; Iida, M.; Gleason, M.E.J.; Xu, J.H.; Bolger, N. Initial elevation bias in subjective reports. Proc. Natl. Acad. Sci. USA 2018, 115, E15–E23. [Google Scholar] [CrossRef]
- Ellis, E.M.; Elwyn, G.; Nelson, W.L.; Scalia, P.; Kobrin, S.C.; Ferrer, R.A. Interventions to Engage Affective Forecasting in Health-Related Decision Making: A Meta-Analysis. Ann. Behav. Med. 2018, 52, 157–174. [Google Scholar] [CrossRef]

| Study 1 | Study 2 | Combined Data | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study 1, N | Study 1, All Groups | Group 1 | Group 2 | Group 3 | Study 2 Overall (N = 612 for All) | Group 1 | Group 2 | Group 3 | Combined Samples | Group 1 | Group 2 | Group 3 | |
| Age (mean, SD) | 1005 | 34.4 (18.1) | 34.6 (17.9) | 34.8 (18.1) | 33.7 (18.2) | 50.4 (15.6) | 50.8 (15.3) | 49.5 (16.1) | 51.0 (15.4) | 40.4 (18.9) | 40.7 (18.7) | 40.6 (18.8) | 40.0 (19.1) |
| Women | 1004 | 54.0% | 50.7% | 56.1% | 55.3% | 50.3% | 51.2% | 52.4% | 47.2% | 52.6% | 50.9% | 54.6% | 52.3% |
| Private health insurance † | 691 | 50.7% | 51.2% | 47.2% | 53.7% | † | † | † | † | - | - | - | - |
| Interview location (anonymized, Ireland only) | 433 | n/a | n/a | n/a | n/a | - | - | - | - | ||||
| 1 | 26.3% | 30.5% | 22.3% | 26.1% | |||||||||
| 2 | 34.2% | 33.8% | 35.2% | 33.6% | |||||||||
| 3 | 27.5% | 23.2% | 32.4% | 26.9% | |||||||||
| 4 | 8.08% | 7.95% | 6.76% | 9.70% | |||||||||
| 5 | 3.93% | 4.64% | 3.38% | 3.73% | |||||||||
| Do you know someone who (% yes) | |||||||||||||
| has received an organ | 992 | 18.2% | 17.0% | 19.0% | 18.5% | 11.1% | 12.0% | 10.6% | 10.8% | 15.5% | 15.1% | 15.7% | 15.7% |
| needs an organ | 997 | 11.9% | 10.0% | 13.6% | 12.3% | 3.59% | 4.78% | 4.33% | 1.54% | 8.76% | 8.01% | 9.92% | 8.40% |
| has donated an organ | 994 | 13.1% | 11.9% | 15.1% | 12.3% | 6.86% | 8.61% | 5.29% | 6.67% | 10.7% | 10.6% | 11.2% | 10.3% |
| Ever donated blood | 998 | 34.6% | 33.1% | 37.3% | 33.4% | 31.2% | 37.3% | 28.9% | 27.2% | 33.3% | 34.7% | 34.0% | 31.2% |
| Study 1 | Study 2 | Combined Data | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study 1, N | Study 1, All Groups | Group 1 | Group 2 | Group 3 | Study 2 Overall (N = 612 for All) | Group 1 | Group 2 | Group 3 | Combined Samples | Group 1 | Group 2 | Group 3 | |
| Intention (mean, SD) | 902 | 4.41 (1.60) | 4.44 (1.66) | 4.30 (1.57) | 4.47 (1.56) | 3.25 (1.54) | 3.13 (1.49) | 3.19 (1.56) | 3.44 (1.56) | 3.94 (1.68) | 3.91 (1.72) | 3.83 (1.66) | 4.07 (1.64) |
| Taking donor card (yes, %) | 895 | 48.7% | 46.3% | 51.6% | 48.4% | - | - | - | - | - | - | - | - |
| Transferred to organ donor website | - | - | - | - | - | 7.03% | 6.22% | 6.25% | 8.72% | - | - | - | - |
| Combined behavioral outcome (Taking card or website transfer) | - | - | - | - | - | - | - | - | - | 31.8% | 29.9% | 32.6% | 32.9% |
| Primary Outcome (Intention) | Secondary Outcomes (Card/Website) | |||||||
|---|---|---|---|---|---|---|---|---|
| Intention | β | Std. Err. | 95% CI | p | OR | 95% CI | p | |
| Study 1 | Group 1 | Ref. | - | - | - | Ref. | - | - |
| Group 2 | −0.120 | 0.130 | −0.375 to 0.134 | 0.354 | 1.28 | 0.890 to 1.84 | 0.183 | |
| Group 3 | 0.025 | 0.127 | −0.224 to 0.274 | 0.850 | 1.34 | 0.932 to 1.93 | 0.113 | |
| Study 2 | Group 1 | Ref. | - | - | - | Ref. | - | - |
| Group 2 | 0.061 | 0.150 | −0.234 to 0.355 | 0.686 | 1.00 | 0.426 to 2.03 | 0.990 | |
| Group 3 | 0.307 | 0.153 | 0.007 to 0.606 | 0.044* | 1.44 | 0.680 to 3.05 | 0.341 | |
| Combined data | Group 1 | Ref. | - | - | - | - | - | |
| Group 2 | −0.047 | 0.098 | −0.239 to 0.146 | 0.637 | 1.22 | 0.882 to 1.70 | 0.227 | |
| Group 3 | 0.136 | 0.098 | −0.055 to 0.328 | 0.163 | 1.37 | 0.982 to 1.90 | 0.063 | |
| Exploratory analyses—Irish data only | Group 1 | Ref. | - | - | - | Ref. | - | - |
| Group 2 | −0.124 | 0.199 | −0.514 to 0.266 | 0.533 | 1.55 | 0.916 to 2.63 | 0.102 | |
| Group 3 | −0.184 | 0.207 | −0.590 to 0.221 | 0.373 | 1.52 | 0.877 to 2.63 | 0.136 | |
| Researcher 1 | Ref. | - | - | - | Ref. | - | - | |
| Researcher 2 | −0.809 | 0.250 | −1.30 to −0.319 | 0.001 ** | 0.42 | 0.210 to 0.851 | 0.016 * | |
| Researcher 3 | −0.395 | 0.227 | −0.840 to 0.049 | 0.081 | 0.34 | 0.184 to 0.647 | 0.001 ** | |
| Researcher 4 | 0.283 | 0.235 | −0.177 to 0.745 | 0.227 | 0.63 | 0.326 to 1.22 | 0.174 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doyle, F.; Morgan, K.; Mathew, M.; Palatty, P.; Kamat, P.; Doherty, S.; Quigley, J.; Henderson, J.; O’Carroll, R. Theory Content, Question-Behavior Effects, or Form of Delivery Effects for Intention to Become an Organ Donor? Two Randomized Trials. Int. J. Environ. Res. Public Health 2019, 16, 1304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071304
Doyle F, Morgan K, Mathew M, Palatty P, Kamat P, Doherty S, Quigley J, Henderson J, O’Carroll R. Theory Content, Question-Behavior Effects, or Form of Delivery Effects for Intention to Become an Organ Donor? Two Randomized Trials. International Journal of Environmental Research and Public Health. 2019; 16(7):1304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071304
Chicago/Turabian StyleDoyle, Frank, Karen Morgan, Mary Mathew, Princy Palatty, Prashanti Kamat, Sally Doherty, Jody Quigley, Josh Henderson, and Ronan O’Carroll. 2019. "Theory Content, Question-Behavior Effects, or Form of Delivery Effects for Intention to Become an Organ Donor? Two Randomized Trials" International Journal of Environmental Research and Public Health 16, no. 7: 1304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16071304