This section first introduces the current situation of the long-term aging health-care system in Taiwan, and then determines the problems through a survey regarding satisfaction degree. Finally, it proposes a systematic improvement method to improve the case. Therefore, this section is divided into three parts: a background description of Taiwan’s long-term care system; data collection, analysis, and results display; and suggestions and improvement strategies.
3.1. Background Description of Taiwan’s Long-Term Ageing-Care System
In 1993, Taiwan’s population structure began to enter an ageing state. More than 14% of the population was older than 65 in 2018, and the birth rate moved to a negative number [
54]. In this population structure change, such as the increase in demand for elderly care services, falling supplies, and other related issues have emerged consecutively. Taiwan’s government also began to study this problem, and in 2000, it formed a long-term care team. After eight years of research, this team proposed a long-term care (LTC) program (known as Long-term Care 1.0 in Taiwan), which covers disabled people, elderly people over 65 years old, mountain natives aged 55 to 64, individuals aged 50 to 64 years old who practice IADLs (instrumental activities of daily living), and individuals who are disabled and live alone [
55].
Among them, the service items include care service, wheezing service, home care, rehabilitation service, auxiliary aid, shuttle service, food delivery service, and long-term institution check-in service. Ten years after the implementation of the plan, Taiwan enacted the Long-Term Care Service Act in 2017 (known as Long-term Care 2.0 in Taiwan), which expanded the scope of services to include preventive care and created backward connections to daily care and peace of mind for the end of life in the home. The purpose of Long-term Care Service 2.0 is to reduce the burden on caregivers and improve the quality of life and dignity of the elderly. In addition, it provides service bases with different levels, scales, and functions, as well as related services, such as small-scale multi-functional care units, dementia care, caregiver service bases, community preventive care, integration of indigenous communities, prevention of disabilities, delay in disabilities, preparation at discharge, referral care after discharge, home care, etc. To put it simply, Long-term Care Service 2.0 is based on the “prevention-medical-care” system [
56].
Long-term care services are extensive and complex, thus, Taiwan’s care system is divided into three levels (A, B, C), each with a different role. Class C, known as the Hutong Long-Term Care Station, is the lowest level unit, which mainly provides a variety of care functions, such as short-term daily care in the village office or service center or meals for care recipients. Class B is known as the Multi-Function Long-Term Health Centre. Its main role is to achieve preventive health care through the integration of various functional departments; for example, after the patient is discharged from the hospital, the hospital sends the patient information data to a Class B care center for subsequent home care. The B-level care center conducts follow-up care needs assessment and sends the relevant information to the C-level care center. The Class C care centers provide services. Level A refers to the community integrated long-term medical service center. The main goal is to plan, develop, and promote the effective implementation of policies through resource allocation [
57].
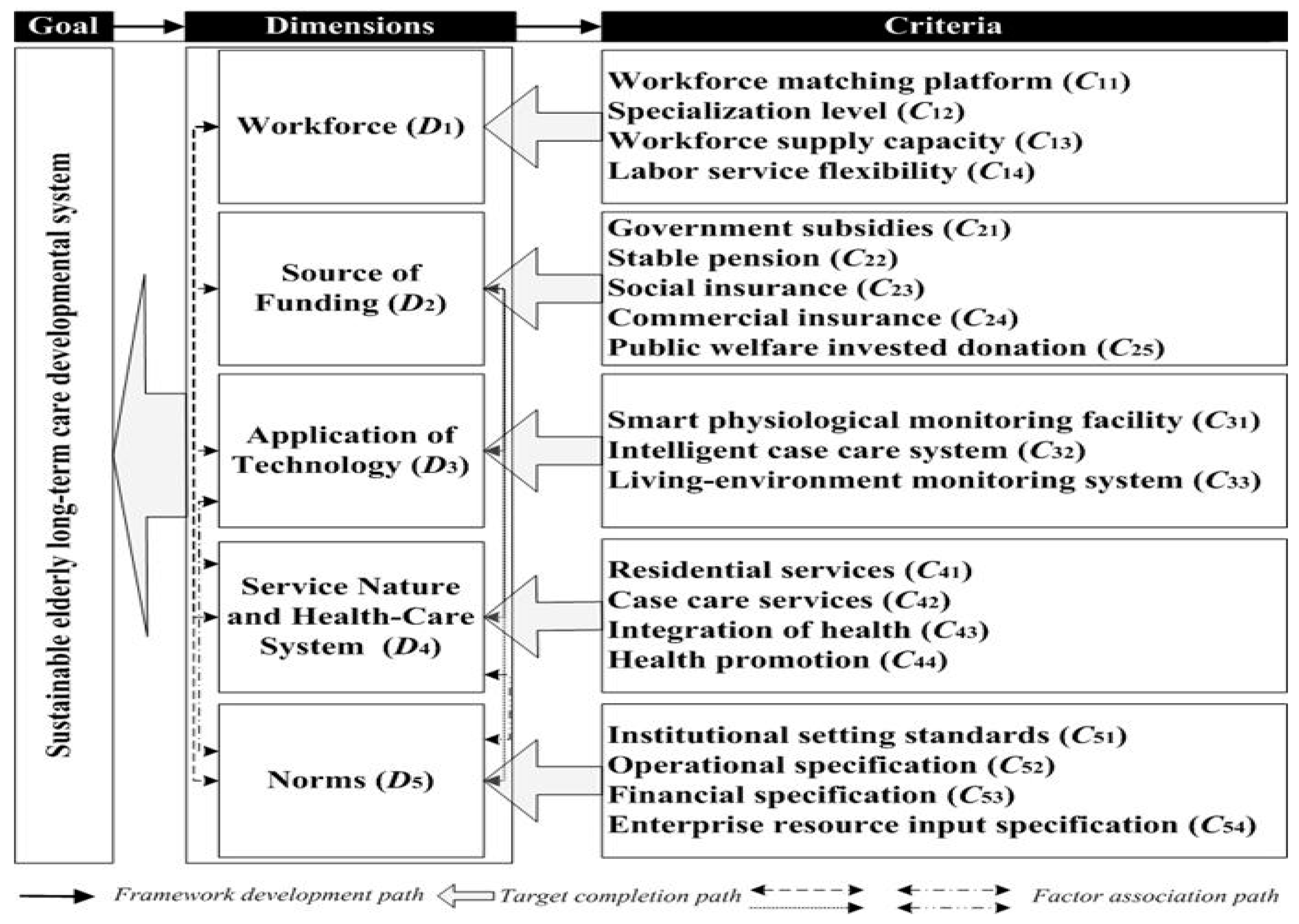
This care system further expands the coverage for dementia patients, as each county and city add a new care platform for dementia into the original disabled care center. The following explains the actual situation in more detail according to this index system.
● Workforce matching platform (C11)
The workforce matching platform can help the elderly by providing considerable assistance, sustain the supply of a long-term care labor force, and facilitate Taiwan’s employment channel platform matchmaking. Different levels of service centers for the elderly need different kinds of help, and the functions of each are not identical. The service centers for different types of professionals also provide related jobs [
58].
● Specialization level (C12)
At a professional level, Taiwan demonstrates the need for care services to be assessed first by government professionals who can develop care plans and link long-term care resources. For those in need of medical care, if they cannot seek medical treatment due to disability, they would receive medical care from home nurses after being visited by medical evaluators. For those in need of rehabilitation, a physical or functional therapist would be sent to the patients’ home for rehabilitation services after diagnosis by specialists [
59].
● Workforce supply capacity (C13)
At present, 45 colleges and universities in Taiwan have established long-term care-related departments, which can train about 5000 nursing professionals every year. Currently, there are about 140,000 licensed caretakers in Taiwan; however, only about 30,000 people are engaged in this industry. When the 2017 long-term care service 2.0 was launched, the shortage of care laborers was about 13,000 people [
50]. In order to make up for this gap, the government recruited the required labor force from fresh nursing graduates, and encouraged middle-aged people and graduates of other majors to enter the long-term care industry.
● Labor service flexibility (C14)
The average monthly salary of the working population in Taiwan is about USD
$1436, while the average monthly salary of long-term care personnel is only about USD
$734 to USD
$834. It can be found that salaries in the long-term care industry are lower than those of other industries [
57]. In the past, most long-term care service providers paid workers’ compensation and used the “uniform package”, which was calculated in time segments. In order to utilize labor more effectively, the “item-by-item pricing” approach is currently used. The purpose of support is to provide more flexible work time compensation, enabling employees to perform their duties more effectively.
● Government subsidies (C21)
At present, the financial resources of the long-term care system in Taiwan are mainly obtained through increasing taxes, and subsidies are based on the two criteria of losing self-care ability and economic status. The financial subsidy in 2017 was set at 100% for individuals earning USD
$343 to USD
$515 per person per month, 90% for individuals earning USD
$515 to USD
$740 per person per month, and 70% for general subsidized care. For remote areas, due to the need for medical care or long-term care services, transportation assistance and caregivers are needed; hence, it is necessary to subsidize transportation and other expenses for severely disabled people in disadvantaged groups, or to rent medical equipment for family health care, such as the home medical equipment needed for rehabilitation and subsidies to improve barrier-free spaces inside and outside the home, as well as elderly care allowances that qualify for long-term care needs [
54]. In the past, the financial resources during long-term care plan 1.0 were based on commercial insurance, and such stable financial resources had significant impact on the sustainability of the long-term care system. Therefore, there is still much discussion in Taiwan regarding the transfer of long-term care services from commercial insurance to taxation.
● Stable pension (C22)
Retirement pensions are the important basis of giving the elderly an independent life. After the Second World War, the global economy shifted from a recession to a period of high growth [
58], thus, Taiwan’s aged population experienced a period of rapid growth, and in this context, the older generation gained a better concept of savings. The the issue of the elderly population is of increasing concern for young people; however, elderly pension is stable, which has a certain stabilizing effect on society and families [
60]. In Taiwan, a pension is a labor protection mechanism, as the government requires employers to pay a certain pension insurance tax every month, as based on the wages of the workers. (Employees can also increase the amount of insurance according to their own wishes.) When workers retire, they can receive a pension from the government and their own employee insurance, as stored in the manner prescribed by law.
● Social insurance (C23)
The national health insurance system is a social medical insurance system [
61], which all Taiwanese can enjoy together; however, this system only solves the medical part of the long-term care system. The subsequent long-term ageing health care is currently dependent on other systems for connection [
62].
● Commercial insurance (C24)
Commercial insurance is used to make up for the deficiency of the public insurance system [
63]. Therefore, different purchasing behaviors are generated according to individual needs, incomes, and characteristics [
64]. This is also true in different areas of Taiwan, such as northern Taiwan, where there are more and higher purchases of commercial insurance, as it is the political and economic core of Taiwan.
● Public welfare invested donation (C25)
Encourage relevant corporate philanthropy, promote corporate social responsibility practices, and achieve the integration of corporate and public welfare undertakings in corporate donations [
31].
● Smart physiological monitoring devices (C31)
Smart physiological monitoring devices can measure the physiological state of the elderly at any time, and then transmit the data to a remote database for interpretation [
35]. At present, the main smart devices in Taiwan can be divided into two categories; one is specialized devices, such as smart mattresses, while other is consumptive devices, such as smart bracelets, crutches, and shoes. Specialized devices are mostly used in large medical and long-term care institutions as they are more expensive [
65].
● Intelligent case care systems (C32)
At present, some large medical care companies in Taiwan are using cloud ERP systems as a management platform in medical care to manage individual cases. This management platform records the past treatment process, rehabilitation, and related follow-up services, in order to enable the medical long-term care agency to make more efficient use of resources and maximize the benefits [
66].
● Living-environment monitoring systems (C33)
Living-environment monitoring systems mainly focus on the long-term care system modularization of merchandise. With living-environment monitoring, the emergency medical system can move quickly during a medical rescue [
67]. Taiwan’s electronic communications technology industry is an interdisciplinary medical and long-term care services industry, and many companies have developed relevant integrated products.
● Residential services (C41)
At present, residential services mainly provide relevant services on the basis of the care management center; they provide timely housework and daily care, help with the provision of meals for caregivers, and body care services [
68]. Care Management Central also provides a meal delivery service for elderly people living alone. Upon assessment, the center provides this service to elderly people who are unable to prepare their own meals [
69].
● Case care services (C42)
Taiwan is promoting a community-based ageing mechanism to provide diversified and differentiated services through the long-term ageing health care service system of caring communities [
55].
● Integration of health (C43)
Since the ultimate goal of a health care system is to provide an integrated preventative care service to those in need, effective integration of the personal home environment, medical system, long-term ageing health care system, and government-related units must be carried out [
6,
37]. Currently, under the Long-Term Care Service 2.0 policy in Taiwan, different functional units have been integrated, and the health care system has been divided into three levels (ABC), which have different responsibilities.
● Health promotion (C44)
Health promotion is currently developing in Taiwan in the two main directions of prevention and the delay of disability. The government also encourages related medical consortiums or school units to propose relevant courses, such as using physical fitness training to prevent the degeneration of functions or delaying the speed of dementia through the stimulation of sound waves [
40].
● Institutional setting standards (C51)
At present, Taiwan’s long-term Care Services Act regulates the management of legally registered long-term care institutions. Under this law, relevant regulations have been established [
56].
● Operational specifications (C52)
The Long-Term Care Services Act applies to legitimate long-term care organizations, including institutional layout, business categories, external advertising, service content and cost criteria, staffing, referral services, and links between healthcare and long-term ageing health care systems. The organization’s safety management, service quality standards, supervision by competent government departments, and illegal penalties are clearly stipulated [
70].
● Financial specifications (C53)
The financial regulations for long-term ageing health care organizations mainly reveal the process of operating performance management with the principle of financial transparency [
71], and there are relevant explicit regulations in the Long-Term Care Services Act.
● Enterprise resource input specifications (C54)
In order to promote the development and subsidies of long-term care system-related resources, the sources of relevant funds have been specified in the Long-Term Care Services Act, among which donation income is one source of funding [
56,
71]. However, monetary donations must comply with the provisions of income tax law regarding donations to charities. In Taiwan, charitable organizations have different norms, as based on individual and for-profit institutions. Individuals can donate to legally-registered charities, with the total donation not exceeding 20% of an individual’s personal income in the current year. The donations made by profit-making institutions shall not exceed 10% of the revenue in the current year. However, there is no restriction if the donation is approved by the Ministry of Finance.
3.3. Results and Discussion
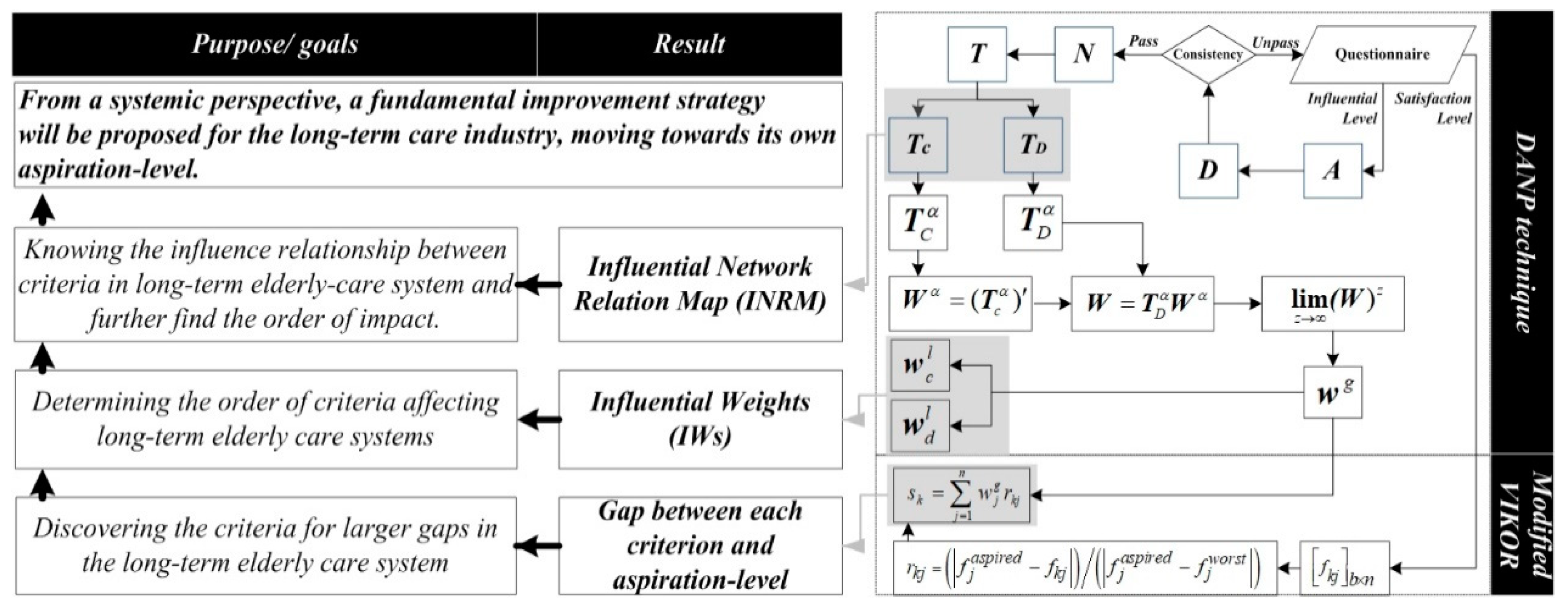
This study constructed an index system for long-term ageing health care, which contains five dimensions and 20 criteria. The interactions of the various factors among the systems were investigated and identified according to the INRM of the DANP technique, as shown in
Figure 3 (For detailed calculation results, please refer to
Appendix B,
Table A1,
Table A2,
Table A3,
Table A4,
Table A5,
Table A6 and
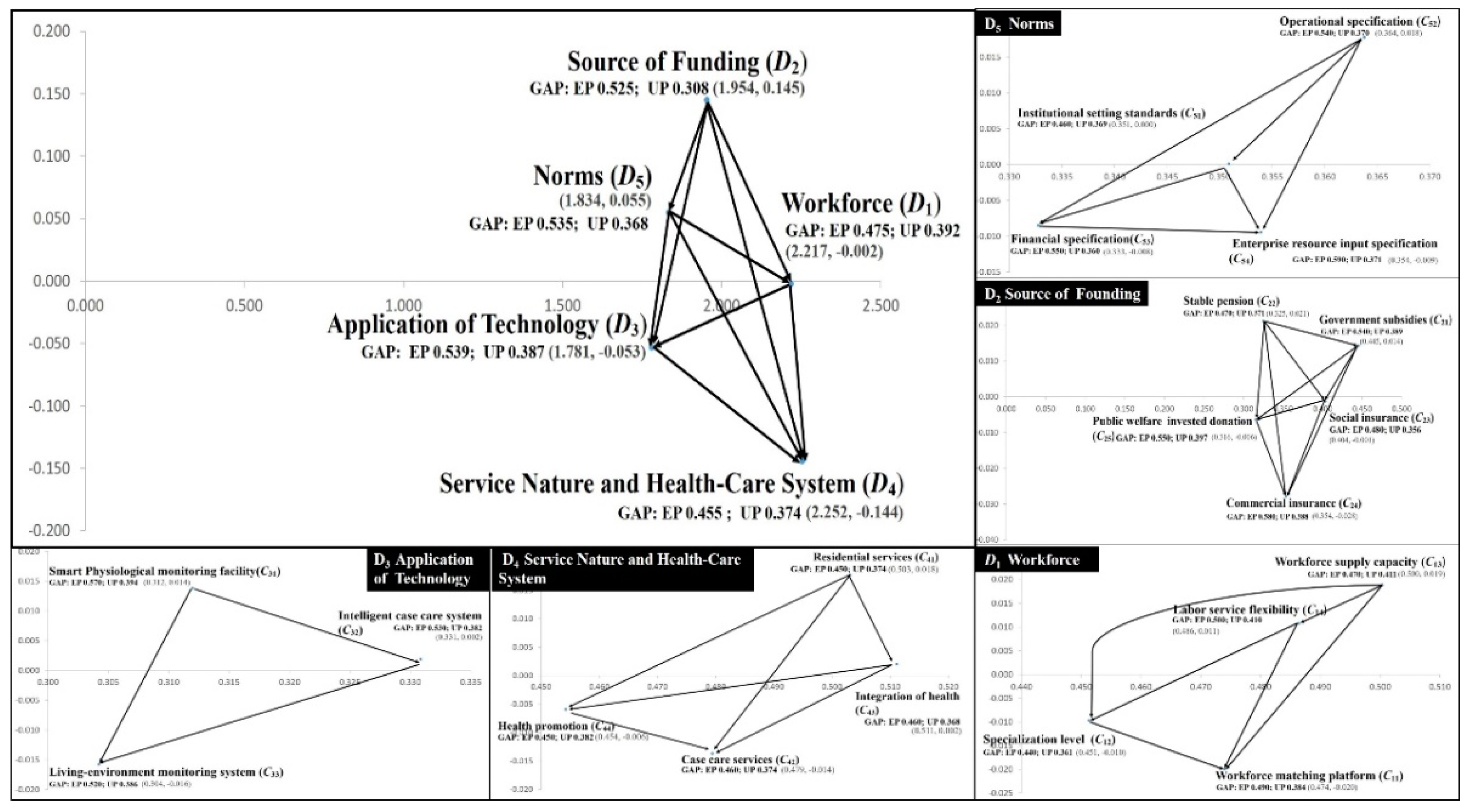
Table A7). The vertical axis of INRM represents the level of influence, where a higher level of influence indicates the factor’s greater impact within the overall system; that is, if this factor changes, other factors would be affected. Therefore, when policy makers need to formulate improvement strategies, there are more effective ways to conceive factors based on the source of influence, especially in the case of limited resources. According to
Figure 3, the order of influence is: source of funding (
D2), norms (
D5), workforce (
D1), application of technology (
D3), and service nature and health-care system (
D4).
These results indicate that source of funding (D2) is the foundation of the long-term ageing health care system, and policymakers should base their plans according to funding, and then, observe the structure to address the other four aspects. The impact of this strategic development, which is referred to as the Coping Measures and Root Cause Improvement Strategy in this study, is a more effective and efficient approach. The use of this improved strategy can promote the sustainability of the long-term health care system.
After understanding the source and impact order of each dimension, the parts of the criteria in each dimension were observed. First, the factor with the most impact on the source of funding (D2) dimension is stable pension (C22). The order of influence is stable pension (C22), government subsidies (C21), social insurance (C23), public welfare investment donation (C25), and commercial insurance (C24). The factor for influencing the source in norms (D5) is operational specifications (C52), and the order of influence is operational specifications (C52), institutional setting standards (C51), financial specifications (C53), and enterprise resource input specifications (C54). The third dimension is workforce (D1), and the factor for influencing the source in this dimension is workforce supply capacity (C13). The order of influence is: workforce supply capacity (C13), labour service flexibility (C14), specialization level (C12), and workforce matching platform (C11). However, the smart physiological monitoring device (C31) is the source of influence of the application of technology (D3), and the order of influence is: smart physiological monitoring devices (C31), intelligent case care system (C32), and living-environment monitoring system (C33). Finally, residential services (C41) is the source of influence for service nature and the health-care system (D4), and the order of influence is: residential services (C41), integration of health (C43), health promotion (C44), and case care services (C42).
After understanding how to develop a complementary and rooted improvement strategy, the next step was to determine the biggest difference from the ideal state, which this study calls the biggest gap. The biggest gap can be found using the modified VIKOR technique, and the results of the operation are shown in
Table 2. Since the long-term health care system has been implemented in Taiwan for some time, this study explored long-term health care from the user perspective (user performance; UP), as well as from the perspectives of the Policy makers and implementers (expert performance; EP). Two different perspectives were used to explore the problem criteria for long-term ageing health care systems.
First, according to the total gap value in
Table 2, the value of UP is 0.380, which is better than the EP value of 0.502. These results represent different degrees of perception between the users (people), policy makers, and implementers (experts). However, both sides believed that there was room for improvement in the system, and that it required improvement. This study then observed the gap value of each dimension. The experts believed that the dimension of the largest gap is Application of Technology (
D3). The order of the gap from large to small is
D3 (0.539),
D5 (0.535),
D2 (0.525),
D1 (0.475), and
D4 (0.455). The public believed that the dimension with the largest gap is Workforce (
D1). The order of gap from large to small is
D1 (0.392),
D3 (0.387),
D2 (0.380),
D4 (0.374), and
D5 (0.368).
The results indicate that the level of experience of the experts and the public only presents a partial consensus, such as the ordering of D3, D2, D4, D3, and D5. The process of filling out the questionnaire found that such cognitive gaps mainly came from differences in opinions. Experts are usually policy designers or industry executives; therefore, they adopt the perspective of design or performance. However, people have strong feelings about the implementation of policy, and this feeling is often affected by the relationships among the media, relatives, friends, and their own impressions. As some of the topics in this study, such as regulations or technology products, are related to professional thinking, and because the respondents were mainly seniors over the age of 65, there might be some degree of error in the perception of this topic. In order to avoid such biases, although the public’s point of view was valued, this study used expert satisfaction in the formulation of support and root improvement strategies.
According to the sorting of the dimension gap, the first description is the application of technology (
D3). In this dimension, the criterion of the maximum gap (Biggest gap) is smart physiological monitoring devices (
C31), which is 0.570. The order is
C31,
C32, and
C33, followed by norms (
D5) in this dimension, and the criterion for the maximum gap is enterprise resource input specifications (
C54), which is 0.590, followed by
C53, C52, and
C51. This is also the biggest gap of all criteria. The following dimension is the source of funding (
D2). In this dimension, the largest gap criterion is commercial insurance (
C24) with a value of 0.580, followed by
C25,
C21,
C23, and
C22. The next dimension is workforce (
D1). In this dimension, the maximum gap criterion is Labour service flexibility (
C14), which is 0.500, followed by
C11,
C13, and
C12. The last dimension is service nature and health-care system (
D4). In this dimension, the maximum gap criteria are case care services (
C42) and integration of health (
C43), both of which are 0.460, while secondary influences are
C41 and
C44 (
Table 2).
The principle of smart physiological monitoring devices (C31), which was the biggest gap in the application of technology (D3), is that large home monitoring systems or professional medical care monitoring systems cannot be extended to every consumer; therefore, current intelligent monitoring systems mainly consist of consumer electronic products, as launched by manufacturers. However, this can lead to incompatible monitoring systems and create gaps in care services. As a result, the intelligent monitoring systems criterion was the source of the application of a technology dimension. Therefore, to improve the application of technology dimension, this study suggested improving the precision of consumer electronics using the data of medical units, integrating the information of consumer electronics with the medical monitoring of large hospital systems, and allowing data to flow instantly in two directions.
Regarding Norms (D5), the factor of gap’s biggest problem is Enterprise resource input specifications (C54), which is due to Taiwan’s current regulations restricting the direct investment of profit-making institutions in long-term ageing health care systems. During the interviews, many experts emphasized that the participation and resource investment of profit-making institutions are important bases for the stable development of long-term health care systems for the elderly. However, the government remains concerned that if laws and regulations are loosened, the profit-making characteristics of profit-making institutions might lead to essential changes for non-profit institutions. In this dimension, the source of impact is Operational Specifications (C52). Currently, the government’s operating regulations are designed to prevent misconduct in operations, rather than sustainable development. Therefore, the idea of adding a transparent navigation drainage mechanism to replace restrictions in the operational specifications could allow for-profit companies to effectively and efficiently channel resources into this career.
In the Source of Funding (D2) dimension, the biggest gap problem criterion was Commercial insurance (C24). The current low purchase rate of commercial health insurance in Taiwan is due to the limitations of salary levels and a lack of sufficient public awareness. While there is a robust health care system in Taiwan, the elderly tend to ignore care and maintenance after receiving medical care, which is a large future expense in their retired life. In addition, young people generally face the problem of insufficient wages, which leads to a lack of willingness to purchase commercial health insurance. Such issues would lead to an increase in social welfare insurance expenditures, thereby affecting the sustainable development of the long-term ageing health care system.
If only relying on individual purchases of commercial health insurance, the dilemma of the problem of insufficient salaries remains, and the funding source of the long-term ageing health care system is still limited. “Funding” should not be regarded as a negative cause. Although the amount of funding positively correlates with the long-term development of the system, “exploring more sources” is not the only point of attention, as “effective use of funding” can also ensure that funding is well allocated. Reducing the waste of expenses could allow assets to be effectively utilized and reach those who need help; for example, the purchase of some commercial insurance considers the price sensitivity of consumers [
72], and also allows doctors to play the role of a bridge between insurance clients and insurance practitioners. Those in need of insurance can communicate with insurance practitioners through professional advice, and then, find the type of insurance that suits them best. This will not only avoid consumer price cost sensitivity issues, it will also mean that consumers can buy business insurance that meets their needs, and thus, effectively reduce their risk of financial bankruptcy. Finally, the system’s sustainability can help more people in need.
For the long-term ageing health care system to achieve sustainability, the performance of funding sources must be improved. A pension is a very important influencing factor, because it is the only source of income for most elderly people. If seniors’ pensions are in a stable state, they would be able and willing to purchase appropriate commercial health insurance, which can serve as an additional source of funding for the long-term ageing health care system and effectively reduce the dependence on social welfare insurance. As a result, more sustainable development of the long-term health care system for the elderly can be provided. Commercial insurance providers can offer appropriate commercial insurance, thereby providing additional attention to the funding sources of the long-term ageing health care system, reducing dependence on social welfare insurance, and enabling the development of the elderly long-term health care system into a more sustainable state.
Regarding the workforce (D1) dimension, the biggest gap problem is Labour service flexibility (C14). Taiwan’s remuneration for care services is a system of unified parcel time; that is, time is used as the pricing standard for long-term ageing health care services. Regardless of the number of care services that a caregiver is required to perform within a given time period, only a fixed salary is paid to the caregiver. In other words, the number of service items is not associated with the compensation. However, in practice, a caregiver often needs to increase or decrease the service time according to his/her abilities and performance. If the number of work items is different, but the same salary is received, it would result in shortage of labour. Therefore, considering the ability of the caregiver and providing reasonable compensation could enable the workforce in the long-term ageing health care system to be effectively promoted.
Regarding the Service nature and health-care system (D4) dimension, the biggest gap problem is case care services (C42) and integration of health (C43). The current long-term care case manager and home care worker system in Taiwan is the relevant system implemented by the government to implement case management services. The main services are based on hospital discharge preparation, home visits, and follow-up care services. The purpose of this system is to enable service users to receive proactive care. The reason for the largest gap is the immediacy of demand from the service demanders. Since service demanders have more urgent need characteristics, case managers must make considerable clarifications in accordance with certain regulations and procedures when handling follow-up care. Such a process is less likely to respond to the needs of service demanders in real time. Residential services are the root cause of all impacts in this dimension. Currently, the service items offered by home caregivers are mainly planned and assigned by the case manager after judging the needs of individual cases. However, the number of service applicants continues to increase year by year; therefore, case managers are taking longer to respond to the needs of real users. Home care workers are often front-line service personnel, and are most familiar with the needs of the patients. In the past, the home care workers only engaged in factional work, as based on the assessment results of case managers; therefore, it is suggested that the services provided by home care workers should be flexible enough to meet the needs of users in real situations.
With regard to the integration of Taiwan’s long-term care system, the preparatory office of the government authority was established in September 2018, which is responsible for the integration of the long-term health care system in Taiwan; however, in the past, its related units and organizations adopted different systems, and efforts have been made to integrate and test the new system. In the past, the integration of health care systems was mostly based on consideration of the part of the system, and was less concerned with case requirements; therefore, it is recommended that home managers provide immediate feedback, which can be integrated into the health care system and used to adjust relevant structures. In general, because home care workers are the front-line service unit, they are also the unit that can identify problems the easiest; therefore, it is recommended to keep home care workers’ job items flexible, and design a mechanism that integrates the views of the immediate response service provider with the needs of the demander, in order to provide a basis for the sustainable development of the elderly health care system.
One aspect of the largest gap in the four areas is application technology (D3). This problem is mainly due to the difference between the precision of physiological and home-monitoring data and medical equipment. The physiological monitoring system is a type of consumer electronic product. A home-monitoring system has two characteristics; the first is the expansion of the physiological monitoring system, which is also a consumer electronics product; the second is the monitoring of the home environment. Such products are usually communication products. While these two types of products offer the advantage of immediate and low-cost monitoring and development, they also have lower precision than medical devices. However, for medical behaviour, high complexity is a necessary choice. Therefore, a problem that must be considered is how to improve the sophistication of consumer electronics and telecom products to integrate real-time monitoring health data with medical systems. To overcome this problem, it is necessary to ensure that multiple sources obtain sufficient funds, formulate appropriate policies and regulations, and protect the privacy of the health data model to establish certain basic standards for integration. Finally, it is important to have a high-quality workforce that is familiar with high quality medical maintenance applications and the implementation of related technology.
In summary, this study found that the two criteria of stable pension (C22) and government subsidies (C21) are the key to the government’s sustainable development of long-term ageing health care systems. The government must effectively adjust and control these two items. If a senior’s pension is in a stable state and there is a certain degree of government subsidy, the government can maintain the transcendence of non-profit businesses without the need specifically to introduce resources from profit-making business units. However, when the personal pensions of the elderly are in an unstable state, and government subsidies are relatively scarce, it is necessary to appropriately introduce resources from profit-making business units. According to the government’s current budget on subsidies for the long-term aging health care system and the current self-sustaining savings rate of the elderly, it is necessary to further conceive relevant laws and regulations, in order to maximize the benefits of resources, provide long-term ageing health care for the elderly, and achieve sustainable development.







{kind=link}
{kind=link}
{kind=link}


