4.1. Measurement of Efficiency and Change
The data envelopment analysis method is used to calculate the provincial health care service efficiency of Chinese township hospitals in 29 provinces of China from 2003 to 2016. The results are shown in
Table 2. Due to space limitation, only the efficiency calculation results of 2003, 2005, 2007, 2009, 2011, 2013, 2015, 2016 and average by year are listed. As can be seen in the table, there exist apparent differences in the average efficiencies of township hospitals in the provinces of China. The township hospitals in most provinces were operating in an inefficient state. The top five provinces that have the highest average efficiencies are Tianjin and Ningxia. Furthermore, Inner-Mongolia, Shanxi and Jilin are the bottom three provinces that have the lowest average efficiencies.
In order to analyze the changing trend of provincial efficiency of Chinese township hospitals, the calculation method of Malmquist index is adopted. Using the method, this paper further measures the changes of efficiency of township hospitals in each province 2004 to 2016. The results are shown in
Table 3.
As can be seen from the table, the average provincial efficiency of Chinese township hospitals for most provinces increased from 2004 to 2016. The average efficiencies of only two provinces, Fujian and Guangdong, decreased during the time period. Besides that, the average efficiencies of township hospitals in Tianjin and Ningxia remained unchanged because the township hospitals in these two provinces were in the efficient state all the time during the time period.
Overall, from 2004 to 2016, the township hospitals in most provinces achieved gains in efficiency, which was conducive to the promotion of provincial total factor productivity for township hospitals in China. Meanwhile, it is also clear that there still exist apparent efficiency differences in township hospitals among provinces, which is a problem that has adverse effects for the improvement of overall efficiency of Chinese township hospitals.
4.2. Decomposition of Efficiency Difference
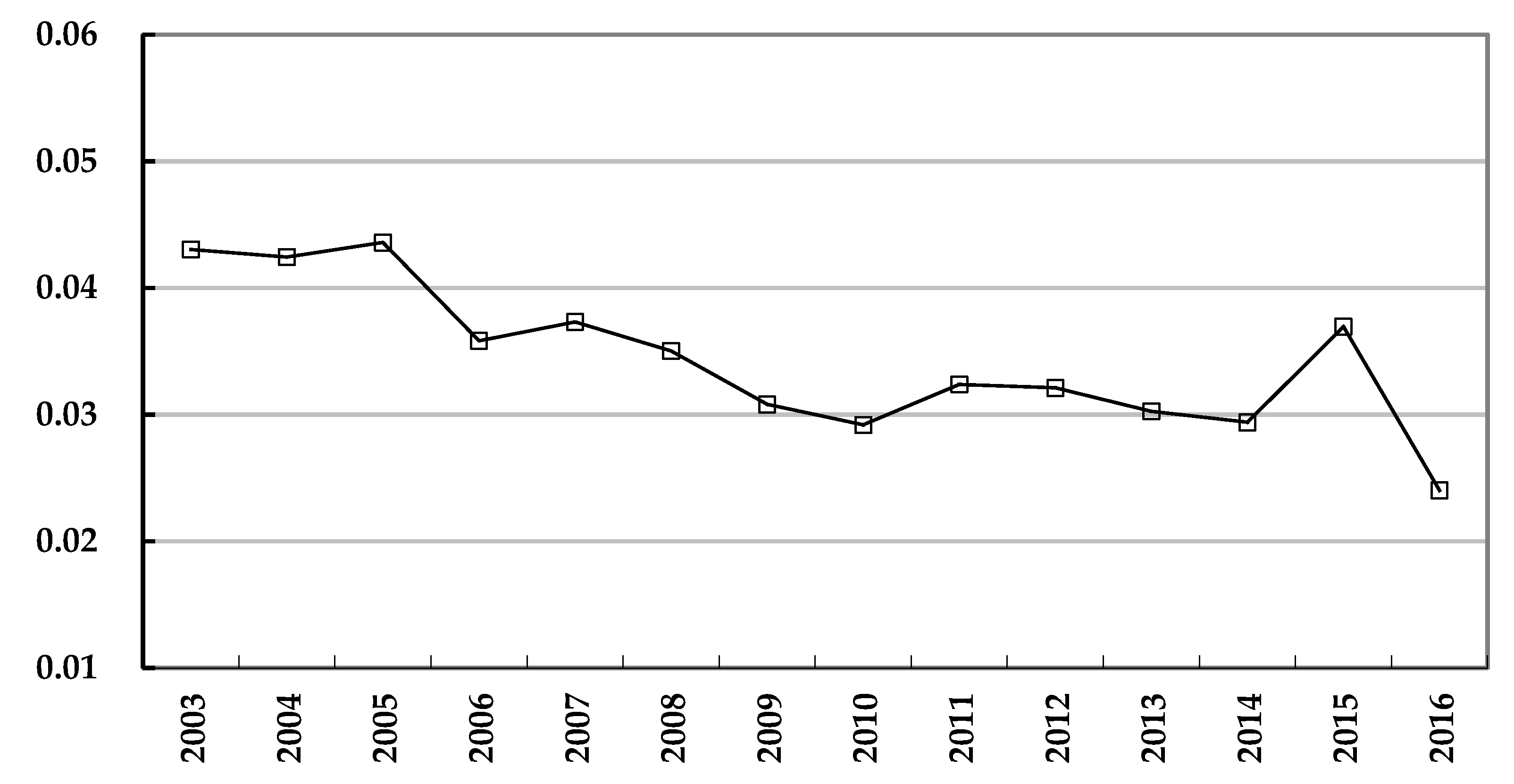
Through the results of provincial township hospital efficiency and efficiency change, it is clear that there exist apparent differences among provinces and regions. Therefore, this paper uses the Theil index to quantifiably measure the differences from 2003 to 2016, as shown in
Figure 1.
As shown in the figure, the changing trend of the Theil index of provincial township hospital efficiency reflects the variation and tendency of efficiency difference change. It can be found that the Theil index was 0.04304 in 2003, and it showed a downward trend decreasing to 0.02402 in 2016, with fluctuations during the time period. Therefore, it is clear that from 2003 to 2016, the decline is only about 44.2% than the difference in 2003, which is a relatively slow shrinkage of the difference in provincial efficiency of township hospitals.
In order to find more effective ways of reducing provincial efficiency difference, it is necessary to find an appropriate way to quantifiably decompose the Theil index to study the structure of the difference, which would be helpful in finding the solution of the problem. Using the Theil index decomposition method, the results for 2003 to 2016 are shown in
Table 4.
(1) Intra-regional difference is the main cause of the overall provincial efficiency difference of Chinese township hospitals, while the inter-regional difference is the minor cause in the overall difference. On average, during the time period from 2003 to 2016, the proportion of the sum of intra-regional differences was 87.0%, while the proportion of inter-regional difference was 13.0%. From the perspective of the proportions year by year, the proportions changed steadily. In 2003, the sum of proportions of intra-regional differences was 74.1%, while the proportion of the inter-regional difference was 25.9%. Although there were minor fluctuations, from 2003 to 2016, the sum of proportions of intra -regional differences increased to 98.1% in 2016, while the proportion of the inter-regional difference decreased to 1.9%.
(2) From the perspective of intra-regional difference for each region, the trends of the differences within the eastern, central and western regions of China were different year by year. Among them, although there were fluctuations during the time period, the proportion of intra-regional difference in eastern China in the overall difference decreased from 17.8% in 2003 to 11.0% in 2016, while the intra-regional difference in central China increased from 28% in 2003 to 51.0% in 2016, and the intra-regional difference in western China increased from 28.3% in 2003 to 36.0% in 2016. Furthermore, the proportion of intra-regional difference in central and western regions took the first place alternatively, while, the proportion of intra-regional difference in eastern region was the lowest through the time period. Except for 2004, 2005, 2006, 2014, 2015 and 2016, the proportion of intra-regional difference in western China was higher than the proportions of other regions during the time period. The proportion of intra-regional difference in central China took the second place in most years, but took the first place in 2004, 2005, 2006, 2014, 2015 and 2016. The intra-regional difference in eastern China was lower than the other two regions from 2003 to 2016, therefore it is relatively unimportant to the overall provincial efficiency difference of Chinese township hospitals.
4.3. Determinants of Provincial Efficiency Difference of Chinese Township Hospitals
To find effective solutions to the shrinkage of the overall efficiency difference, it is necessary to further investigate the relative importance of the determinants for the difference. This paper uses the Grey correlation analysis model to study the correlation between overall provincial efficiency difference of Chinese township hospitals (x0) and the determinants of difference including: (1) difference of medical technical personnel proportion (x1); (2) difference of medical managerial personnel proportion (x2); (3) difference of licensed doctor and assistant doctor proportion (x3); (4) difference of provincial average years of schooling (x4); (5) difference of public medical and health expenditure proportion (x5); (6) difference of rural household health care and medical services expenditure proportion (x6); (7) difference of economic development level (x7).
Compared to the conventional statistical coefficients, Grey correlation analysis has much less strict requirements on the sample size. For each year, only one value of each Theil index could be obtained. Therefore, Grey correlation analysis is more appropriate for this paper than other conventional statistical methods.
According to the steps of the Grey relational analysis method, the Grey correlations between provincial efficiency difference of Chinese township hospitals and the determinants can be obtained. As shown in
Table 5, initial value treatment is conducted on raw data sequences.
Based on the results of initial value treatment, dimensionless differential sequences are calculated as shown in
Table 6.
According to the difference sequence in the table, the following values could be obtained:
Based on the results of difference sequence in the table 6, the grey correlation table are calculated as shown in
Table 7.
Furthermore, the Grey correlations between provincial efficiency differences of Chinese township hospitals (sequence x
0) and the determinants of efficiency difference (sequence x
1–x
7) could be solved. The results are shown in
Table 8.
According to the correlation results in
Table 8, among the determinants, the degree of correlation between x
0 and x
7 (difference of economic development level) is the highest among all the correlations. Then, x
1 (difference of medical technical personnel proportion), x
4 (difference of provincial average years of schooling), x
5 (difference of public medical and health expenditure proportion), x
6 (difference of rural household health care and medical services expenditure proportion), x
2 (difference of medical managerial personnel proportion), x
3 (difference of licensed doctor and assistant doctor proportion) take the second to seventh place in their degree of correlation with x
0 (overall provincial efficiency difference of Chinese township hospitals).
Furthermore, because the decomposition results of the Theil index reveal the structural causes of the provincial efficiency difference of Chinese township hospitals, i.e., the intra-regional difference is the major cause of the overall difference, this paper further examines the Grey correlations between intra-regional difference of provincial efficiency difference of Chinese township hospitals and determinants within each of the eastern, central and western regions of China. The results are shown in
Table 9.
According to the results in
Table 9, it is clear to see that the correlations between the intra-regional difference of provincial efficiency of Chinese township hospitals and determinants vary tremendously across different regions in China.
First of all, for the eastern region, x4 (difference of provincial average years of schooling) has the highest correlation with x0. The remaining determinants, including x7 (difference of economic development level), x5 (difference of public medical and health expenditure proportion), x3 (difference of licensed doctor and assistant doctor proportion), x1 (difference of medical technical personnel proportion), x2 (difference of medical managerial personnel proportion), x6 (difference of rural household health care and medical services expenditure proportion), rank from the second position to the seventh position with respect to their correlation with x0.
Secondly, for the central region, x7 (difference of economic development level) has the highest correlation with x0. The remaining determinants, including x3 (difference of licensed doctor and assistant doctor proportion), x1 (difference of medical technical personnel proportion), x6 (difference of rural household health care and medical services expenditure proportion), x5 (difference of public medical and health expenditure proportion), x4 (difference of provincial average years of schooling), x2 (difference of medical managerial personnel proportion), rank from the second position to the seventh position with respect to their correlation with x0.
Finally, for the western region, x6 (difference of rural household health care and medical services expenditure proportion) has the highest correlation with x0. The remaining determinants, including x2 (difference of medical managerial personnel proportion), x1 (difference of medical technical personnel proportion), x4 (difference of provincial average years of schooling), x5 (difference of public medical and health expenditure proportion), x7 (difference of economic development level), x3 (difference of licensed doctor and assistant doctor proportion), rank from the second position to the seventh position with respect to their correlation with x0.




{kind=link}