Occupational Risk Evaluation through Infrared Thermography: Development and Proposal of a Rapid Screening Tool for Risk Assessment Arising from Repetitive Actions of the Upper Limbs


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants
2.3. Workstation
2.4. Equipment
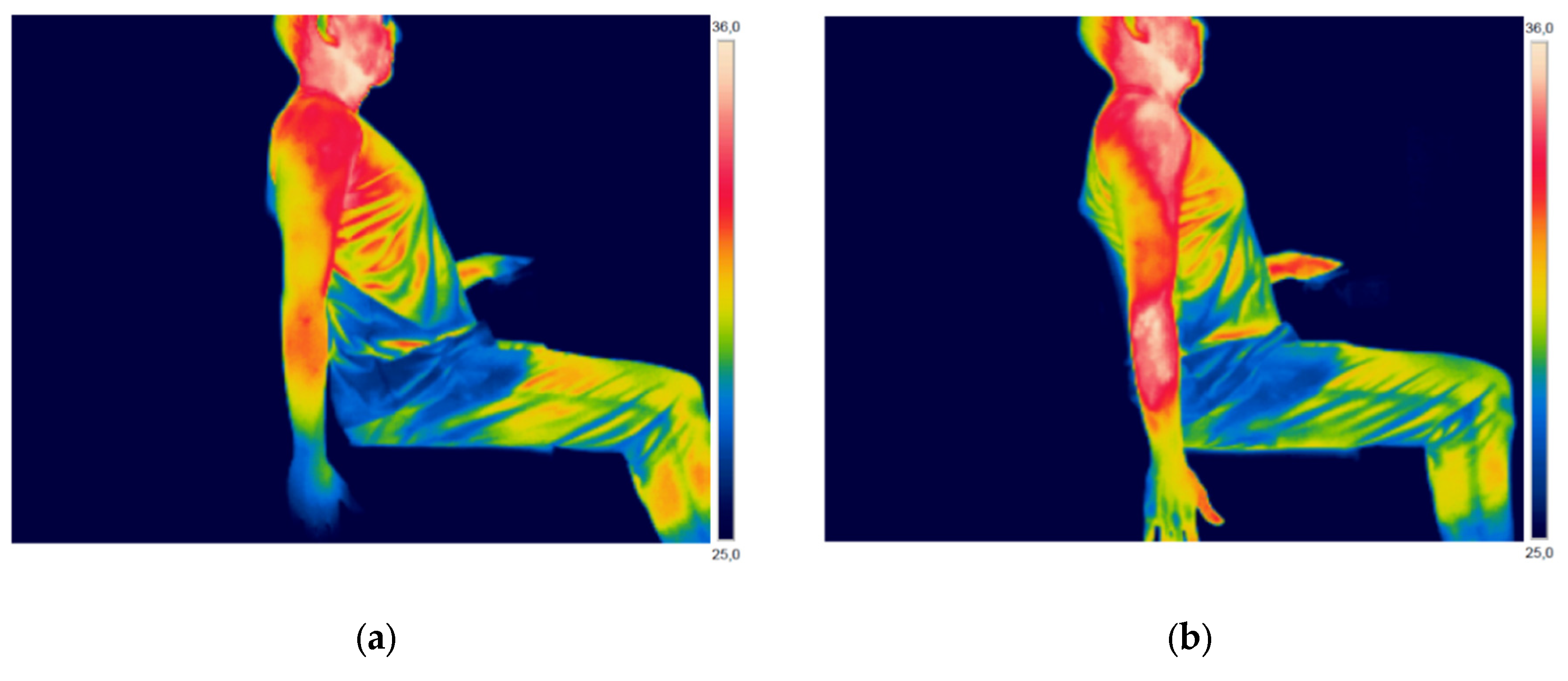
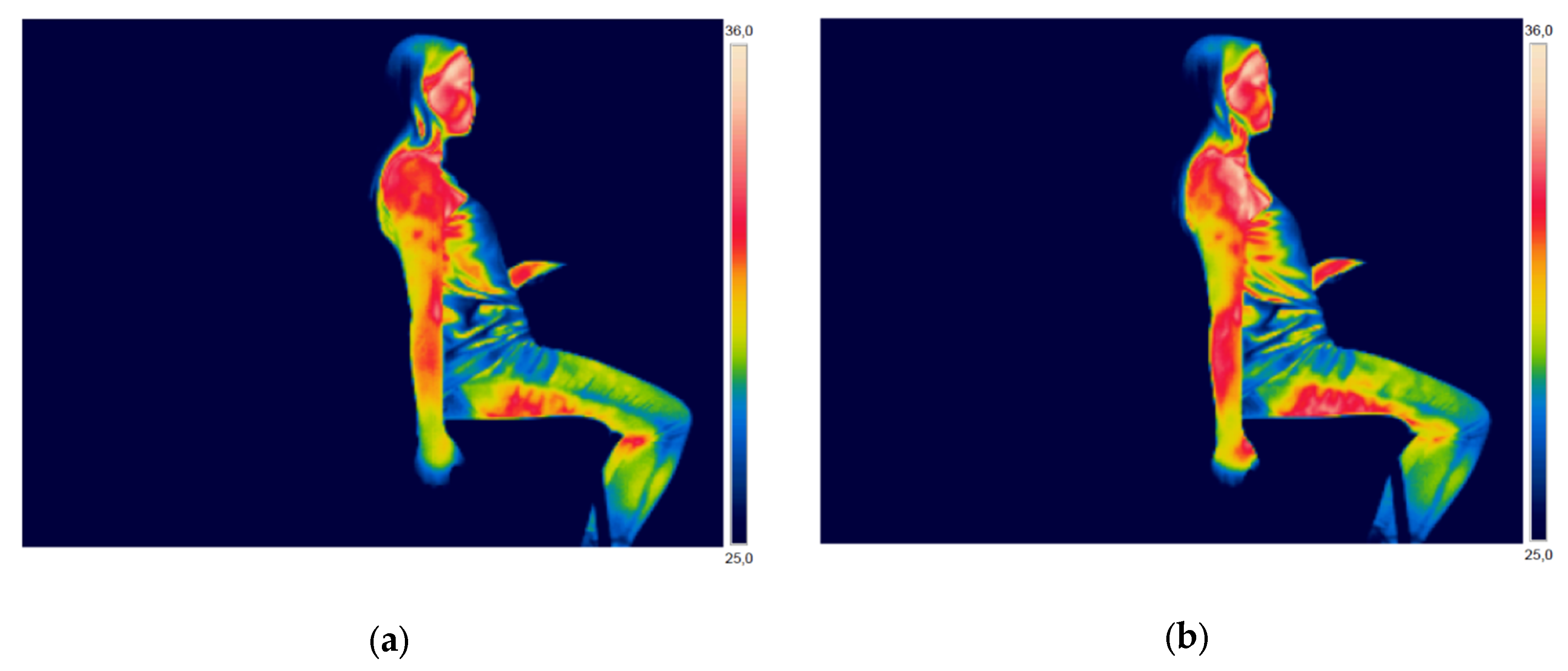
2.5. Infrared Thermography (IT): Experimental Procedures
2.6. Statistical Analysis
- paired t-test: to find out whether significant temperature variation occurred after the performance of the task in each OCRA level (per ROI); to compare the actual OCRA Index values and the predicted values calculated using linear regression;
- correlation test: correlation analysis was performed between the results obtained per ROI and the OCRA level performed by each participant; and,
- regression analysis: to determine equations that allow for calculating the OCRA level of each repetitive task, using the temperature variation of each ROI as input information.
3. Results
3.1. OCRA Index
3.2. Variation of Skin Temperature
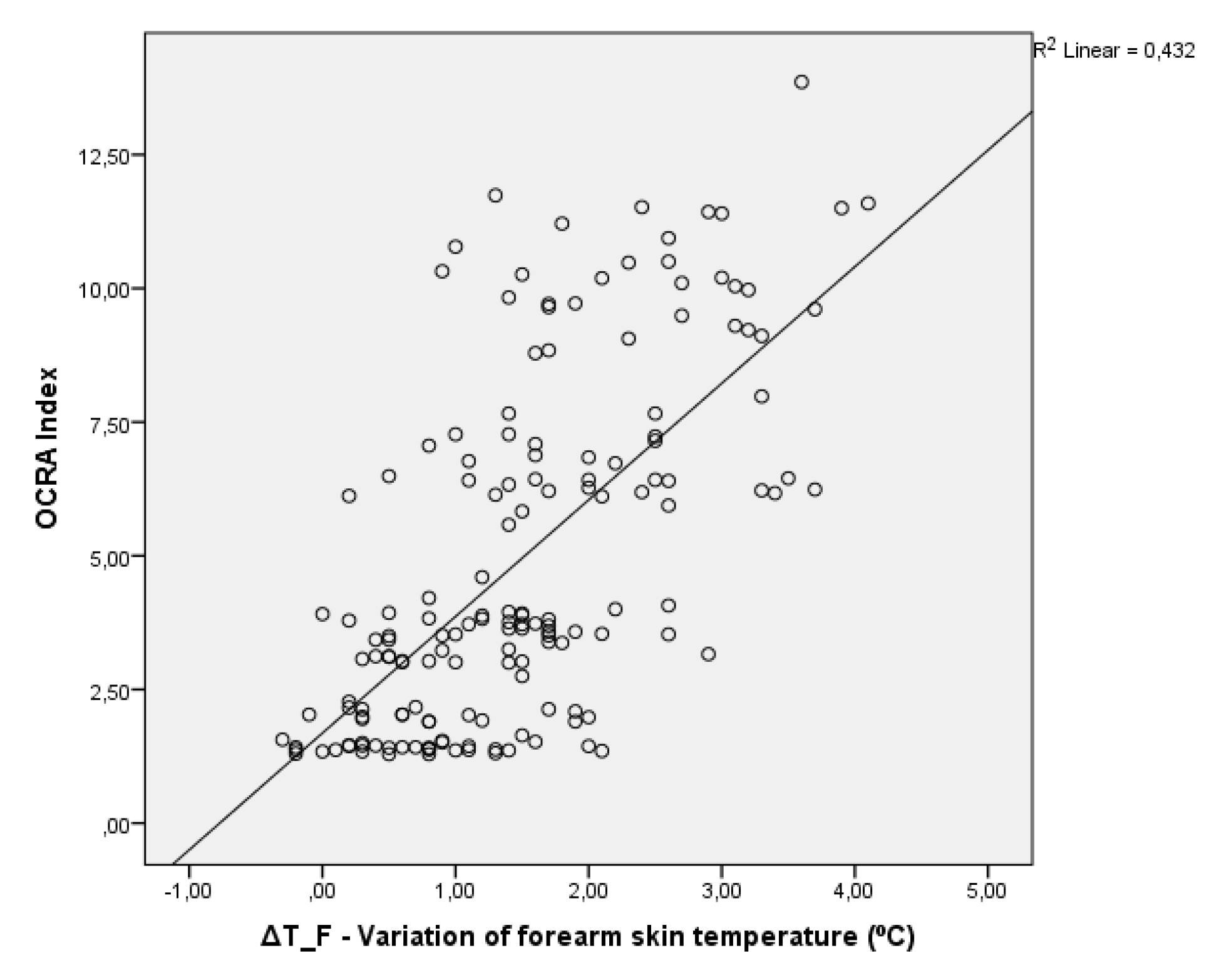
3.3. Correlation Analysis
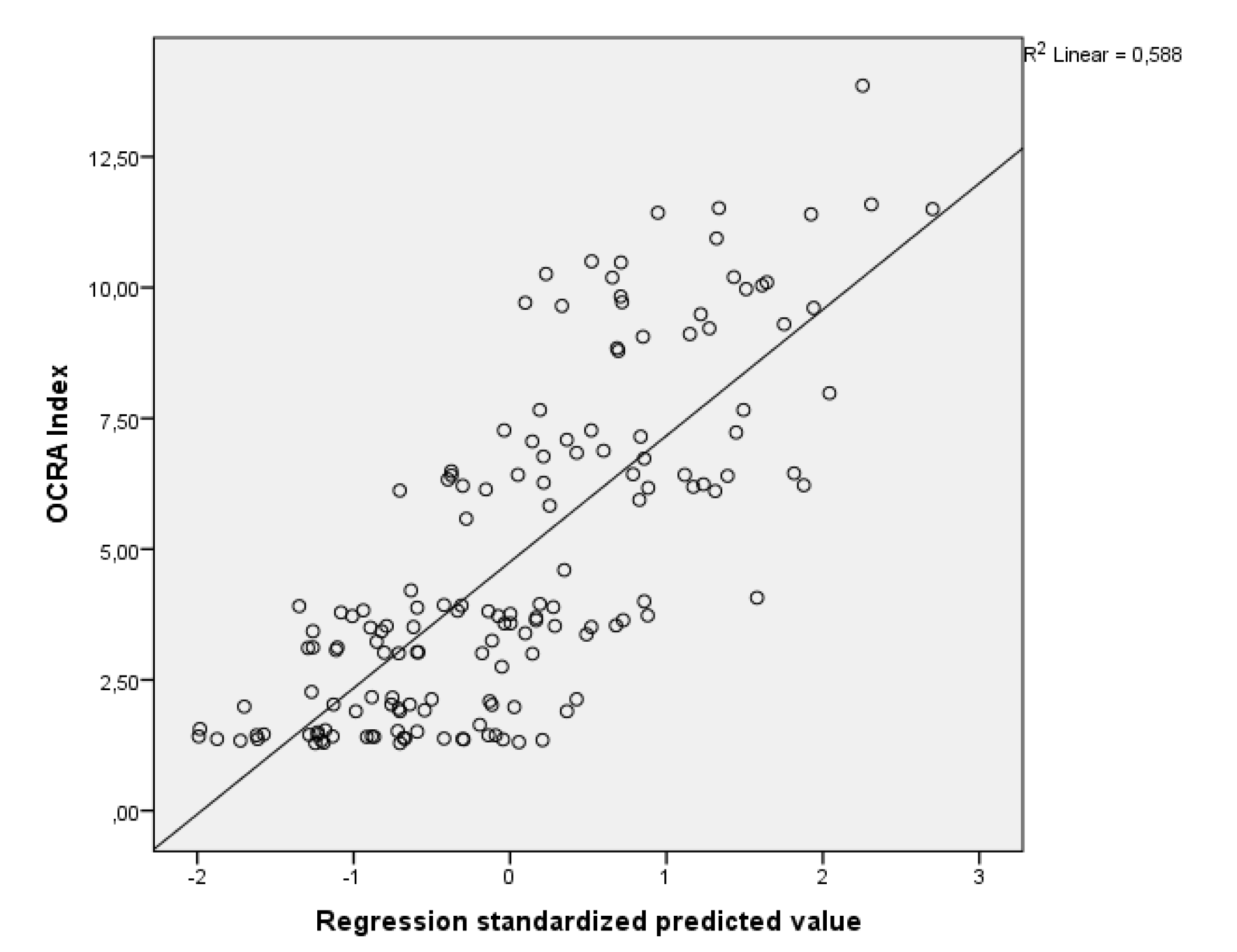
3.4. Regression Analysis
3.5. Proposal of a Rapid Tool for Risk Assessment Through Infrared Thermography Arising from Repetitive Actions of the Upper Limbs
- Phase 1—Day before risk assessment: instructions that must be passed on to workers who will participate in the risk assessment the day before the analysis, as they may interfere with the results. Examples: energy drinks, physical activity, sun exposure, andd menstrual cycle;
- Phase 2—Risk assessment day (before starting the work shift): actions that must be taken before the risk assessment begins, by the risk evaluator and the worker;
- Phase 3—Risk assessment: execution of the repetitive task by the worker and application of IT by the risk evaluator;
- Phase 4—Risk analysis: transfer of thermal images and computer analysis, application of equation 2 to calculate the Predicted OCRA Index and final risk diagnosis;
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lin, J.H.; Kirlik, A.; Xu, X. New technologies in human factors and ergonomics research and practice. Appl. Ergon. 2018, 66, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Salmon, P.M.; Macquet, A.-C. Human factors and ergonomics in sport and outdoor recreation: From individuals and their equipment to complex sociotechnical systems and their frailties. Appl. Ergon. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.R. Fundamentals of systems ergonomics/human factors. Appl. Ergon. 2014, 45, 5–13. [Google Scholar] [CrossRef]
- Buckle, P.; Dul, J.; Bruder, R.; Wilson, J.R.; Falzon, P.; van der Doelen, B.; Carayon, P.; Marras, W.S. A strategy for human factors/ergonomics: Developing the discipline and profession. Ergonomics 2012, 55, 377–395. [Google Scholar] [CrossRef] [Green Version]
- Hollnagel, E. Human factors/ergonomics as a systems discipline? “The human use of human beings” revisited. Appl. Ergon. 2014, 45, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-Castrillo, J.A.; Pérez-Mira, V.; Del Carmen Pardo-Ferreira, M.; Rubio-Romero, J.C. Analysis of required investigations of work-related musculoskeletal disorders in Spain. Int. J. Environ. Res. Public Health 2019, 16, 1682. [Google Scholar] [CrossRef] [Green Version]
- WHO Scientific Group. The Burden of Musculoskeletal Conditions at the Start of the New Millenium Report of a WHO Scientific Group; WHO: Geneva, Switzerland, 2003; pp. 1–218. [Google Scholar]
- Chiang, C.-L.; Liao, C.-Y.; Hsien-Wen, K. Postures of upper extremity correlated with carpal tunnel syndrome (CTS). Int. J. Occup. Med. Environ. Health 2017, 30, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Reste, J.; Zvagule, T.; Kurjane, N.; Martinsone, Z.; Martinsone, I.; Seile, A.; Vanadzins, I. Wrist hypothermia related to continuous work with a computer mouse: A digital infrared imaging pilot study. Int. J. Environ. Res. Public Health 2015, 12, 9265–9281. [Google Scholar] [CrossRef] [Green Version]
- Camargo, C.; Ordorica, J.; De La Vega, E.J.; Olguín, J.E.; López, O.R.; López, J.A. Analysis of temperature on the surface of the wrist due to repetitive movements using sensory thermography. Work 2012, 41, 2569–2575. [Google Scholar] [CrossRef] [Green Version]
- Tirloni, A.S.; Dos Reis, D.C.; Ramos, E.; Moro, A.R.P. Thermographic evaluation of the hands of pig slaughterhouse workers exposed to cold temperatures. Int. J. Environ. Res. Public Health 2017, 14, 838. [Google Scholar] [CrossRef]
- Sousa, E.; Vardasca, R.; Teixeira, S.; Seixas, A.; Mendes, J.; Costa-Ferreira, A. A review on the application of medical infrared thermal imaging in hands. Infrared Phys. Technol. 2017, 85, 315–323. [Google Scholar] [CrossRef]
- Ramos, E.; dos Reis, D.C.; Tirloni, A.S.; Moro, A.R.P. Thermographic analysis of the hands of poultry slaughterhouse workers exposed to artificially cold environment. Procedia Manuf. 2015, 3, 4252–4259. [Google Scholar] [CrossRef] [Green Version]
- Gold, J.E.; Cherniack, M.; Hanlon, A.; Soller, B. Skin temperature and muscle blood volume changes in the hand after typing. Int. J. Ind. Environ. 2010, 40, 161–164. [Google Scholar] [CrossRef]
- Gold, J.E.; Cherniack, M.; Hanlon, A.; Dennerlein, J.T.; Dropkin, J. Skin temperature in the dorsal hand of office workers and severity of upper extremity musculoskeletal disorders. Int. Arch. Occup. Environ. Health 2009, 82, 1281–1292. [Google Scholar] [CrossRef]
- Gold, J.E.; Cherniack, M.; Buchholz, B. Infrared thermography for examination of skin temperature in the dorsal hand of office workers. Eur. J. Appl. Physiol. 2004, 93, 245–251. [Google Scholar] [CrossRef]
- Guertler, C.; Speck, G.M.; Mannrich, G.; Merino, G.S.A.D.; Merino, E.A.D.; Seiffert, W.Q. Occupational health and safety management in Oyster culture. Aquacultural Eng. 2016, 70, 63–72. [Google Scholar] [CrossRef]
- del Carmen Flores-Olivares, B.; Yoguez-Seoane, A.; Susarrey-Huerta, O.; del Carmen Gutiérrez-Torres, C. Preliminary study on the evaluation of musculoskeletal risks through infrared thermography for drummers. Procedia Manuf. 2015, 3, 4415–4420. [Google Scholar] [CrossRef] [Green Version]
- Gold, J.E.; Hallman, D.M.; Hellström, F.; Björklund, M.; Crenshaw, A.G.; Mathiassen, S.E.; Barbe, M.F.; Ali, S. Systematic review of quantitative imaging biomarkers for neck and shoulder musculoskeletal disorders. BMC Musculoskeletal Disord. 2017, 18, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Bertmaring, I.; Babski-Reeves, K.; Nussbaum, M.A. Infrared imaging of the anterior deltoid during overhead static exertions. Ergonomics 2008, 51, 1606–1619. [Google Scholar] [CrossRef]
- Chander, D.S.; Cavatorta, M.P. An observational method for Postural Ergonomic Risk Assessment (PERA). Int. J. Ind. Ergon. 2017, 57, 32–41. [Google Scholar] [CrossRef]
- European Agency for Safety and Health at Work. Introduction to Work-Related Musculoskeletal Disorders; European Agency for Safety and Health at Work: Brussels, Belgium, 2007; Volume 1681, pp. 4–8. [Google Scholar]
- U.S. Bureau of Labor Statistics. Survey of Occupational Injuries and Illnesses Data; U.S. Bureau of Labor Statistics: Washington, WA, USA, 2018. [Google Scholar]
- Lotter, O.; Lieb, T.; Breul, V.; Molsner, J. Is repetitive workload a risk factor for upper extremity musculoskeletal disorders in surgical device mechanics? A cross-sectional analysis. Int. J. Env. Res. Public Health 2020, 17, 1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunnekreef, J.J.J.; Thijssen, D.H.J.; Oosterhof, J.; Hopman, M.T.E. Bilateral changes in forearm oxygen consumption at rest and after exercise in patients with unilateral repetitive strain injury: A case-control study. J. Orthop. Sports Phys. Ther. 2012, 42, 371–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roman-Liu, D. Comparison of concepts in easy-to-use methods for MSD risk assessment. Appl. Ergon. 2014, 45, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Occhipinti, E.; Colombini, D. The OCRA Method: Assessment of exposure to occupational repetitive actions of the upper limbs. Int. Encycl. Ergon. Hum. Factors 2006, 1, 3289–3297. [Google Scholar]
- Moore, J.S.; Garg, A. The strain index: A proposed method to analyze jobs for risk of distal upper extremity disorders. Am. Ind. Hyg. Assoc. J. 1995, 56, 443–458. [Google Scholar] [CrossRef]
- ACGIH. Documentation of the Threshold Limit Values of Physical Agents, 7th ed.; Amercian Conference of Governmental Industrial Hygienists: Cincinnati, OH, USA, 2001. [Google Scholar]
- Antonucci, A. Comparative analysis of three methods of risk assessment for repetitive movements of the upper limbs: OCRA index, ACGIH (TLV), and strain index. Int. J. Ind. Ergon. 2019, 70, 9–21. [Google Scholar] [CrossRef]
- ISO. ISO 11228-3-Ergonomics—Manual Handling—Part 3: Handling of Low Loads at High Frequency; International Organization for Standardization: Geneva, Switzerland, 2007; p. 76. [Google Scholar]
- CEN. EN 1005-5-Safety of Machinery—Human Physical Performance—Part 5: Risk Assessment for Repetitive Handling at High Frequency; European Committee for Standardization,: Brussels, Belgium, 2007; p. 75. [Google Scholar]
- Colombini, D.; Delleman, N.; Fallentin, N.; Kilbom, A.; Grieco, A. Exposure assessment of upper limb repetitive movements: A consensus document. Int. Encycl. Ergon. Hum. Factors 2006, 3, 55–71. [Google Scholar]
- Hall, J.E.; Guyton, A. Guyton and Hall Textbook of Medical Physiology, 13th ed.; Elsevier: Philadelphia, PA, USA, 2015; ISBN 978-1-4557-7005-2. [Google Scholar]
- Parsons, K. Human Thermal Environments: The Effects of hot, Moderate, and Cold Environments on Human Health, Comfort and Performance, 3rd ed.; Taylor & Francis Group: Boca Raton, FL, USA, 2002; ISBN 978-1-4665-9599-6. [Google Scholar]
- Pinto, N.M.; Xavier, A.A.P.; Do Amaral, R.T. Analysis of the thermal comfort model in an environment of metal mechanical branch. Work 2012, 41, 1606–1611. [Google Scholar] [CrossRef] [Green Version]
- Broday, E.E.; de Paula Xavier, A.A.; de Oliveira, R. Comparative analysis of methods for determining the clothing surface temperature (tcl) in order to provide a balance between man and the environment. Int. J. Ind. Ergon. 2017, 57, 80–87. [Google Scholar] [CrossRef]
- Zontak, A.; Sideman, S.; Verbitsky, O.; Beyar, R. Dynamic thermography: Analysis of hand temperature during exercise. Ann. Biomed. Eng. 1998, 26, 988–993. [Google Scholar] [CrossRef]
- Ferreira, J.J.A.; Mendonça, L.C.S.; Nunes, L.A.O.; Andrade Filho, A.C.C.; Rebelatto, J.R.; Salvini, T.F. Exercise-associated thermographic changes in young and elderly subjects. Ann. Biomed. Eng. 2008, 36, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Ring, E.F.J.; Ammer, K. Infrared thermal imaging in medicine. Physiol. Meas. 2012, 33. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, B.B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Faust, O.; Rajendra Acharya, U.; Ng, E.Y.K.; Hong, T.J.; Yu, W. Application of infrared thermography in computer aided diagnosis. Infrared Phys. Technol. 2014, 66, 160–175. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.Y.K. A review of thermography as promising non-invasive detection modality for breast tumor. Int. J. Sci. 2009, 48, 849–859. [Google Scholar] [CrossRef]
- Szentkuti, A.; Kavanagh, H.S.; Grazio, S. Infrared thermography and image analysis for biomedical use. Period. Biol. 2011, 113, 385–392. [Google Scholar]
- Vardasca, R.; Ring, E.F.J.; Plassmann, P.; Jones, C. Termal symmetry of the upper and lower extremities in healthy subjects. Thermology Int. 2012, 22, 53–60. [Google Scholar]
- Zaproudina, N.; Ming, Z.; Hänninen, O.O.P. Plantar infrared thermography measurements and low back pain intensity. J. Manipulative Physiol. Ther. 2006, 29, 219–223. [Google Scholar] [CrossRef]
- Rossignoli, I.; Fernández-Cuevas, I.; Benito, P.J.; Herrero, A.J. Relationship between shoulder pain and skin temperature measured by infrared thermography in a wheelchair propulsion test. Infrared Phys. Technol. 2016, 76, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Lasanen, R.; Piippo-Savolainen, E.; Remes-Pakarinen, T.; Kröger, L.; Heikkilä, A.; Julkunen, P.; Karhu, J.; Töyräs, J. Thermal imaging in screening of joint inflammation and rheumatoid arthritis in children. Physiol. Meas. 2015, 36, 273–282. [Google Scholar] [CrossRef]
- Abate, M.; Di Carlo, L.; Di Romualdo, S.; Ionta, S.; Ferretti, A.; Romani, G.L.; Merla, A. Postural adjustment in experimental leg length difference evaluated by means of thermal infrared imaging. Physiol. Meas. 2010, 31, 35–43. [Google Scholar] [CrossRef] [PubMed]
- ISO. ISO 7730:2005-Ergonomics of the Thermal Environment—Analytical Determination and Interpretation of Thermal Comfort using Calculation of the PMV and PPD Indices and Local Thermal Comfort Criteria; International Organization for Standardization: Geneva, Switzerland, 2005. [Google Scholar]
- Dibai-Filho, A.V.; Guirro, E.C.O.; Ferreira, V.T.K.; Brandino, H.E.; Vaz, M.M.O.L.L.; Guirro, R.R.J. Reliability of different methodologies of infrared image analysis of myofascial trigger points in the upper trapezius muscle. Braz. J. Phys. Ther. 2015, 19, 122–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ring, E.F.J.; Ammer, K. The Technique of Infra red Imaging in Medicine. Thermology Int. 2000, 10, 7–14. [Google Scholar]
- Fernández-Cuevas, I.; Bouzas Marins, J.C.; Arnáiz Lastras, J.; Gómez Carmona, P.M.; Piñonosa Cano, S.; García-Concepción, M.Á.; Sillero-Quintana, M. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Phys. Technol. 2015, 71, 28–55. [Google Scholar] [CrossRef]
- Zaproudina, N.; Varmavuo, V.; Airaksinen, O.; Närhi, M. Reproducibility of infrared thermography measurements in healthy individuals. Physiol. Meas. 2008, 29, 515–524. [Google Scholar] [CrossRef]
- Ring, F.; Ammer, K.; Wiecek, B.; Plassmann, P.; Jones, C.D.; A, J.; P, M. Quality assurance of thermal imaging systems in medicine. Thermology Int. 2007, 17, 103–106. [Google Scholar]
- Pagani, R.N.; Kovaleski, J.L.; Resende, L.M. Methodi Ordinatio: A proposed methodology to select and rank relevant scientific papers encompassing the impact factor, number of citation, and year of publication. Scientometrics 2015, 105, 2109–2135. [Google Scholar] [CrossRef]
- Govindu, N.K.; Babski-Reeves, K. Reliability of thermal readings of the skin surface over the anterior deltoid during intermittent, overhead tapping tasks. Int. J. Ind. Ergon. 2012, 42, 136–142. [Google Scholar] [CrossRef]
- Kenny, G.P.; Jay, O. Thermometry, calorimetry, and mean body temperature during heat stress. Compr. Physiol. 2013, 3, 1689–1719. [Google Scholar] [CrossRef]
- Ammer, K. Temperature readings from thermal images are less dependent on the number of pixels of the measurement area than on variation of room temperature. Thermology Int. 2005, 15, 131–133. [Google Scholar]
- Abate, M.; Carlo, L.; Donato, L.; Romani, G.; Merla, A. Comparison of cutaneous termic response to a standardised warm up in trained and untrained individuals. J. Sports Med. Phys. Fitness 2013, 53, 209–215. [Google Scholar] [PubMed]
- Ludwig, N.; Formenti, D.; Gargano, M.; Alberti, G. Skin temperature evaluation by infrared thermography: Comparison of image analysis methods. Infrared Phys. Technol. 2014, 62, 1–6. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of Correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- Vardasca, R.; Magalhaes, C.; Silva, P.; Abreu, P.; Mendes, J.; Restivo, M.T. Biomedical musculoskeletal applications of infrared thermal imaging on arm and forearm: A systematic review. J. Therm. Biol. 2019, 82, 164–177. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Sánchez, E.; Vergara-Hernández, C.; Cibrián, R.M.; Salvador, R.; Sanchis, E.; Codoñer-Franch, P. Infrared thermal imaging in the diagnosis of musculoskeletal injuries: A systematic review and meta-analysis. Am. J. Roentgenol. 2014, 203, 875–882. [Google Scholar] [CrossRef]
- Amaro, A.M.; Paulino, M.F.; Neto, M.A.; Roseiro, L. Hand-arm vibration assessment and changes in the thermal map of the skin in tennis athletes during the service. Int. J. Environ. Res. Public Health 2019, 16, 5117. [Google Scholar] [CrossRef] [Green Version]
- Merla, A.; Mattei, P.A.; Di Donato, L.; Romani, G.L. Thermal imaging of cutaneous temperature modifications in runners during graded exercise. Ann. Biomed. Eng. 2010, 38, 158–163. [Google Scholar] [CrossRef]
- Bartuzi, P.; Roman-Liu, D.; Wiśniewski, T. The influence of fatigue on muscle temperature. Int. J. Occup. Saf. Environ. 2012, 18, 233–243. [Google Scholar] [CrossRef] [Green Version]
- Akimov, E.B.; Son’kin, V.D. Skin temperature and lactate threshold during muscle work in athletes. Hum. Physiol. 2011, 37, 120–128. [Google Scholar] [CrossRef]
- Kenny, G.P.; Mcginn, R. Restoration of thermoregulation after exercise. J. Appl. Physiol. 2017, 122, 933–944. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 32) | Male (n = 16) | Female (n = 16) |
|---|---|---|---|
| Age (years) | 25.84 (4.90) | 26.38 (5.25) | 25.31 (4.63) |
| Weight (kg) | 71.16 (15.00) | 77.63 (15.60) | 64.69 (11.52) |
| Height (m) | 1.72 (0.10) | 1.78 (0.08) | 1.65 (0.07) |
| BMI (Kg/m²) | 24.05 (4.00) | 24.29 (3.99) | 23.82 (4.14) |
| Zone | OCRA Index | Risk Level |
|---|---|---|
| Green | OCRA ≤ 2.2 | Acceptable |
| Yellow | 2.2 < OCRA ≤ 3.5 | Conditionally Acceptable |
| Orange | 3.5 < OCRA ≤ 4.5 | Low |
| Red | 4.5 < OCRA ≤ 9 | Medium |
| Purple | OCRA > 9 | High |
| Zone | Recovery Periods | Technical Actions and Repetitiveness |
|---|---|---|
| Green | Journey: 9 h; Break for meal: 1 h break; Other breaks: 20 min. Non-repetitive tasks: 20 min; Experiment: 20 min. | Rate of 40 bpm per technical action, 19 technical actions, 40-s cycles and 660 cycles per journey. |
| Yellow | Rate of 50 bpm per technical action, 24 technical actions, 38-s cycles and 694 cycles per journey. | |
| Orange | Rate of 60 bpm per technical action, 23 technical actions, 32-s cycles and 825 cycles per journey. | |
| Red | Rate of 60 bpm per technical action, 41 technical actions, 42-s cycles and 623 cycles per journey. | |
| Purple | Rate of 110 bpm per technical action, 51 technical actions, 42-s cycles and 630 cycles per journey. |
| Zone | Posture | Force |
|---|---|---|
| Green | Arm: abduction < 45°; Elbow: pronation, supination, flexion and extension > 60°; Wrist: ulnar deviation > 20°; Hand: pinch grip. | Actions that required lifting pieces corresponded to 0.5 in the Borg Scale, while other cases corresponded to 0. |
| Yellow | ||
| Orange | Arm: abduction between 45° and 80°; Elbow: pronation, supination, flexion and extension > 60°; Wrist: ulnar deviation > 20°; Hand: pinch grip. | |
| Red | ||
| Purple |
| Zone | Mean | Standard Deviation | Standard Error | Minimum | Maximum |
|---|---|---|---|---|---|
| Green | 1.413 | 0.082 | 0.014 | 1.29 | 1.64 |
| Yellow | 2.563 | 0.606 | 0.107 | 1.90 | 3.92 |
| Orange | 3.716 | 0.291 | 0.051 | 3.16 | 4.60 |
| Red | 6.562 | 0.519 | 0.092 | 5.58 | 7.66 |
| Purple | 10.261 | 1.149 | 0.203 | 7.98 | 13.86 |
| Zone | Mean | Standard Deviation | Standard Error | Minimum | Maximum | Paired t-Test | |
|---|---|---|---|---|---|---|---|
| dF | p-Value | ||||||
| Green | 0.881 | 0.621 | 0.120 | −0.60 | 1.80 | 31 | 0.000 * |
| Yellow | 1.175 | 0.594 | 0.105 | 0.00 | 2.50 | 31 | 0.000 * |
| Orange | 1.425 | 0.655 | 0.116 | −0.40 | 2.80 | 31 | 0.000 * |
| Red | 1.734 | 0.691 | 0.122 | 0.30 | 2.90 | 31 | 0.000 * |
| Purple | 1.772 | 0.666 | 0.118 | 0.60 | 3.10 | 31 | 0.000 * |
| Zone | Mean | Standard Deviation | Standard Error | Minimum | Maximum | Paired t-Test | |
|---|---|---|---|---|---|---|---|
| dF | p-Value | ||||||
| Green | 0.706 | 0.629 | 0.111 | −0.30 | 2.10 | 31 | 0.000 * |
| Yellow | 0.869 | 0.594 | 0.105 | −0.10 | 2.00 | 31 | 0.000 * |
| Orange | 1.400 | 0.663 | 0.117 | 0.00 | 2.90 | 31 | 0.000 * |
| Red | 1.919 | 0.858 | 0.152 | 0.20 | 3.70 | 31 | 0.000 * |
| Purple | 2.488 | 0.865 | 0.153 | 0.90 | 4.10 | 31 | 0.000 * |
| Zone | Mean | Standard Deviation | Standard Error | Minimum | Maximum | Paired t-Test | |
|---|---|---|---|---|---|---|---|
| dF | p-Value | ||||||
| Green | −0.150 | 1.080 | 0.191 | −2.90 | 2.00 | 31 | 0.438 |
| Yellow | −0.022 | 0.945 | 0.167 | −1.70 | 2.30 | 31 | 0.897 |
| Orange | 0.344 | 0.950 | 0.168 | −1.10 | 2.40 | 31 | 0.049 * |
| Red | 0.581 | 1.126 | 0.199 | −1.10 | 2.80 | 31 | 0.006 * |
| Purple | 1.150 | 1.256 | 0.222 | −1.40 | 3.70 | 31 | 0.000 * |
| Statistics | ΔT_S × OCRA | ΔT_F × OCRA | ΔT_H × OCRA |
|---|---|---|---|
| N | 160 | 160 | 160 |
| Pearson Correlation (r) | 0.426 | 0.658 | 0.423 |
| p-value | 0.000 * | 0.000 * | 0.000 * |
| Model | B | 95% B Confidence Interval | Standard Error | t | Pearson Correlation (r) | Significance |
|---|---|---|---|---|---|---|
| Constant | 1.684 | 0.989–2.379 | 0.352 | 4.786 | - | 0.000 |
| ΔT_F (°C) | 2.181 | 1.788–2.573 | 0.199 | 10.973 | 0.658 | 0.000 * |
| Model | B | Pearson Correlation (r) | Standard Error | t | Significance |
|---|---|---|---|---|---|
| Gender (M; F) | 0.893 | 0.017 | 0.503 | 1.775 | 0.078 |
| Age (years) | −0.035 | 0.038 | 0.041 | −0.852 | 0.395 |
| Weight (Kg) | 0.174 | 0.002 | 0.110 | 1.587 | 0.115 |
| Height (m) | −14.045 | −0.020 | 9.596 | −1.464 | 0.145 |
| BMI (Kg/m²) | −0.480 | 0.019 | 0.329 | −1.462 | 0.146 |
| Air temperature (°C) | 0.614 | 0.439 | 0.115 | 5.325 | 0.000 * |
| Relative humidity (%) | −0.010 | −0.090 | 0.023 | −0.422 | 0.673 |
| ΔT_F (°C) | 2.116 | 0.658 | 0.193 | 10.983 | 0.000 * |
| Model | B | 95% B Confidence Interval | Standard Error | t | Pearson Correlation (r) | Significance |
|---|---|---|---|---|---|---|
| Constant | −10.173 | −14.406–5.939 | 2.143 | −4.747 | - | 0.000 |
| Air temperature | 0.567 | 0.362−0.772 | 0.104 | 5.458 | 0.422 | 0.000 * |
| ΔT_F | 2.083 | 1.749−2.418 | 0.169 | 12.305 | 0.713 | 0.000 * |
| Paired t-Test | Standard Deviation | N | dF | t | p-Value |
|---|---|---|---|---|---|
| Calculated OCRA Index x Predicted OCRA Index | 2018 | 155 | 154 | 0.000 | 1000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares, A.L.; Xavier, A.A.d.P.; Michaloski, A.O. Occupational Risk Evaluation through Infrared Thermography: Development and Proposal of a Rapid Screening Tool for Risk Assessment Arising from Repetitive Actions of the Upper Limbs. Int. J. Environ. Res. Public Health 2020, 17, 3390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103390
Soares AL, Xavier AAdP, Michaloski AO. Occupational Risk Evaluation through Infrared Thermography: Development and Proposal of a Rapid Screening Tool for Risk Assessment Arising from Repetitive Actions of the Upper Limbs. International Journal of Environmental Research and Public Health. 2020; 17(10):3390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103390
Chicago/Turabian StyleSoares, André Luiz, Antonio Augusto de Paula Xavier, and Ariel Orlei Michaloski. 2020. "Occupational Risk Evaluation through Infrared Thermography: Development and Proposal of a Rapid Screening Tool for Risk Assessment Arising from Repetitive Actions of the Upper Limbs" International Journal of Environmental Research and Public Health 17, no. 10: 3390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103390