The Disparities in Mental Health Between Gay and Bisexual Men Following Positive HIV Diagnosis in China: A One-Year Follow-Up Study

Abstract
:1. Introduction
2. Methods
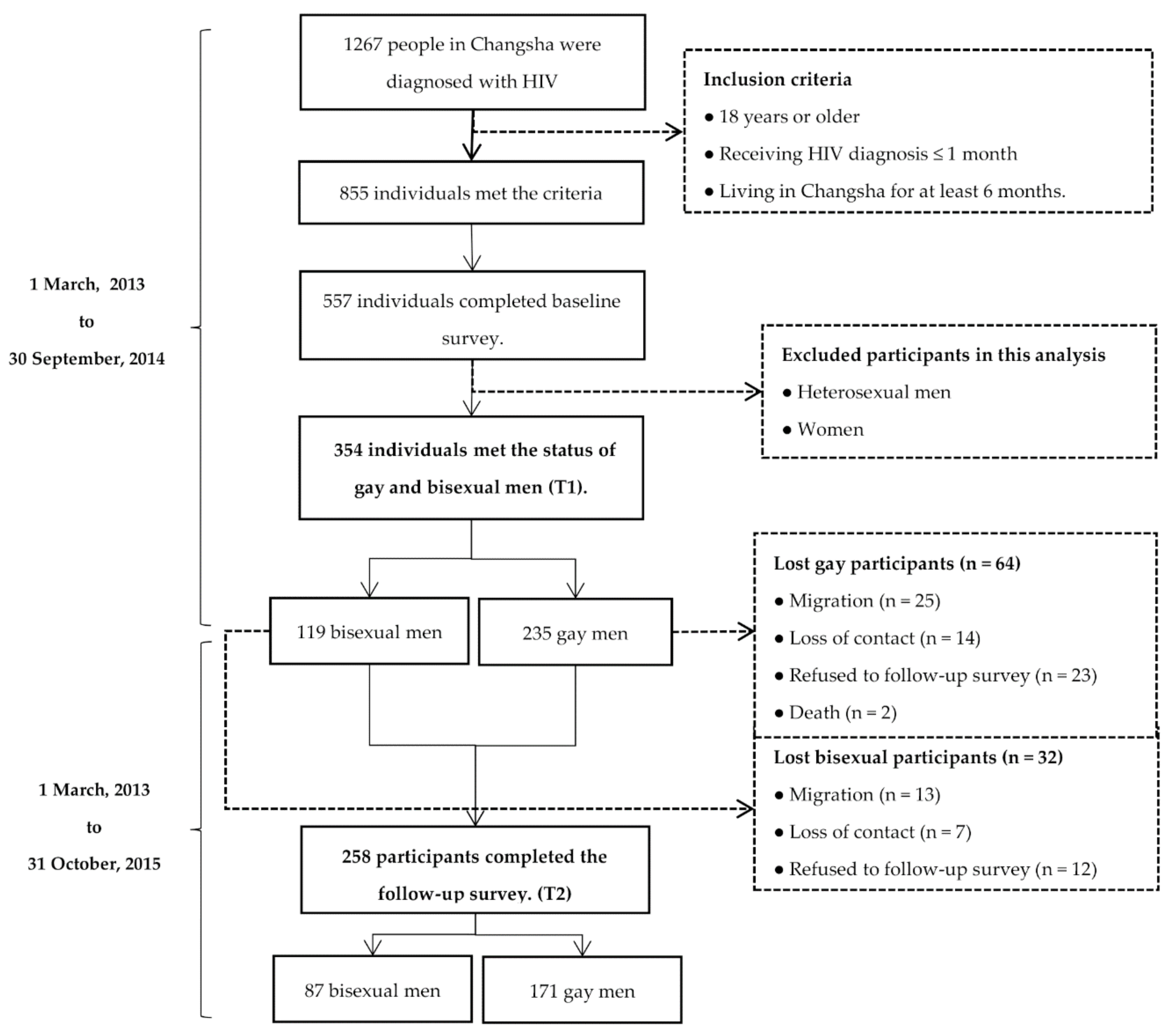
2.1. Participants
2.2. Measures
2.2.1. Socio-Demographic Information
2.2.2. Clinical Information
2.2.3. Sexual Orientation
2.2.4. HIV/AIDS-Related Stress
2.2.5. Social Support
2.2.6. Mental Health Care Utilization
2.2.7. Depression
2.2.8. Anxiety
2.3. Procedures
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Participant Characteristics
3.3. Comparisons of Psychosocial Characteristics Between the Gay and Bisexual Group
3.4. Differences in the Trajectories of Psychosocial Status between the Gay and Bisexual Group
3.5. Multivariate Analysis of the Factors Associated with Changes in Depression and Anxiety One Year After Diagnosis
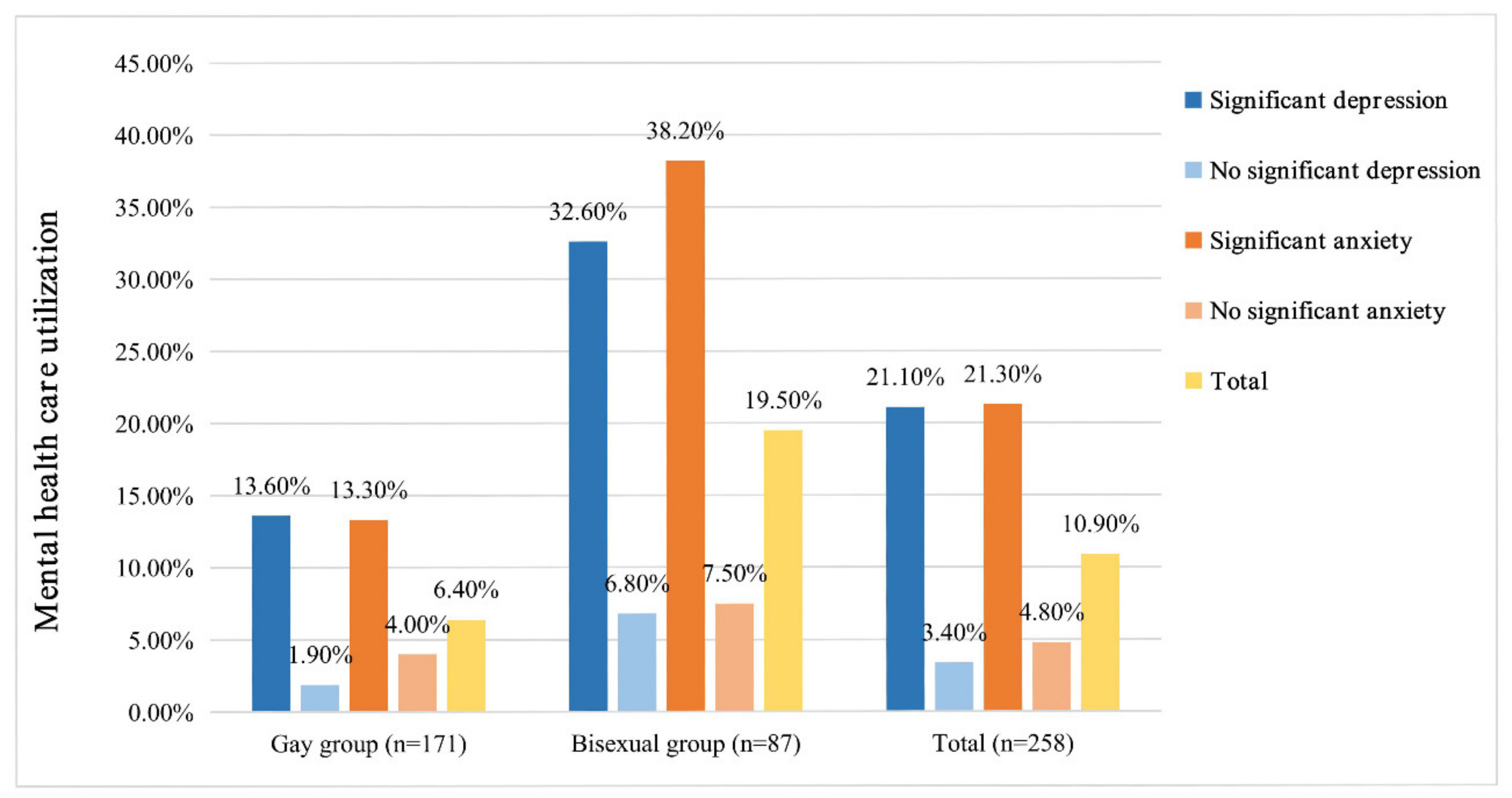
3.6. Mental Health Care Utilization Among the Gay and Bisexual Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brandt, C.; Zvolensky, M.J.; Woods, S.P.; Gonzalez, A.; Safren, S.A.; O’Cleirigh, C.M. Anxiety symptoms and disorders among adults living with HIV and aids: A critical review and integrative synthesis of the empirical literature. Clin. Psychol. Rev. 2017, 51, 164–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.T.; Fu, H.L.; Kaminga, A.C.; Li, Z.Z.; Guo, G.P.; Chen, L.Z.; Li, Q.X. Prevalence of depression or depressive symptoms among people living with HIV/aids in china: A systematic review and meta-analysis. BMC Psychiatry 2018, 18, 160. [Google Scholar] [CrossRef] [Green Version]
- Tao, J.; Qian, H.Z.; Kipp, A.M.; Ruan, Y.H.; Shepherd, B.E.; Amico, K.R.; Shao, Y.M.; Lu, H.Y.; Vermund, S.H. Effects of depression and anxiety on antiretroviral therapy adherence among newly diagnosed HIV-infected Chinese MSM. Aids 2017, 31, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myer, L.; Seedat, S.; Stein, D.J.; Moomal, H.; Williams, D.R. The mental health impact of aids-related mortality in south Africa: A national study. J. Epidemiol. Community Health 2009, 63, 293–298. [Google Scholar] [CrossRef]
- Dong, M.J.; Peng, B.; Liu, Z.F.; Ye, Q.N.; Liu, H.; Lu, X.L.; Zhang, B.; Chen, J.J. The prevalence of HIV among MSM in China: A large-scale systematic analysis. BMC Infect. Dis. 2019, 19, 1000. [Google Scholar] [CrossRef] [Green Version]
- Safren, S.A.; Blashill, A.J.; O’Cleirigh, C.M. Promoting the sexual health of MSM in the context of comorbid mental health problems. Aids Behav. 2011, 15, S30–S34. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Zhong, X.N.; Peng, B.; Zhang, Y.; Liang, H.; Dai, J.H.; Zhang, J.Y.; Zhong, X.H.; Huang, A.L. Comparison of depression and anxiety between HIV-negative men who have sex with men and women (MSMW) and men who have sex with men only (MSMO): A cross-sectional study in western china. BMJ Open 2019, 9, e023498. [Google Scholar] [CrossRef]
- Sun, S.F.; Pachankis, J.E.; Li, X.M.; Operario, D. Addressing minority stress and mental health among men who have sex with men (MSM) in china. Curr. Hiv/Aids Rep. 2020, 17, 35–62. [Google Scholar] [CrossRef]
- Kamen, C.; Flores, S.; Taniguchi, S.; Khaylis, A.; Lee, S.; Koopman, C.; Gore-Felton, C. Sexual minority status and trauma symptom severity in men living with HIV/aids. J. Behav. Med. 2012, 35, 38–46. [Google Scholar] [CrossRef] [PubMed]
- De Moraes, R.P.; Casseb, J. Depression and adherence to antiretroviral treatment in HIV-positive men in sao paulo, the largest city in south America: Social and psychological implications. Clinics 2017, 72, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Aunon, F.M.; Simoni, J.M.; Yang, J.P.; Shiu, C.S.; Chen, W.T.; Edmunds, S.R.; Ramaiya, M.; Cheng, J.; Zhao, H.X. Depression and anxiety among HIV-positive men who have sex with men and men who have sex with women in china. Aids Care Psychol. Socio Med. Asp. Aids/Hiv 2020, 32, 362–369. [Google Scholar] [CrossRef]
- Brennan, D.J.; Bauer, G.R.; Bradley, K.; Tran, O.V. Methods used and topics addressed in quantitative health research on gay, bisexual and other men who have sex with men: A systematic review of the literature. J. Homosex. 2017, 64, 1519–1538. [Google Scholar] [CrossRef] [PubMed]
- Cerwenka, S.; Brunner, F. Sexual identity, sexual attraction and sexual behavior—Dimensions of sexual orientation in survey research. Z. Fur Sex. 2018, 31, 277–294. [Google Scholar]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.X.; Choi, K. Experiences of social discrimination among men who have sex with men in Shanghai, China. Aids Behav. 2006, 10, S25–S33. [Google Scholar] [CrossRef]
- Ploderl, M.; Tremblay, P. Mental health of sexual minorities. A systematic review. Int. Rev. Psychiatry 2015, 27, 367–385. [Google Scholar] [CrossRef]
- Jorm, A.F.; Korten, A.E.; Rodgers, B.; Jacomb, P.A.; Christensen, H. Sexual orientation and mental health: Results from a community survey of young and middle-aged adults. Br. J. Psychiatry 2002, 180, 423–427. [Google Scholar] [CrossRef]
- Bostwick, W.B.; Boyd, C.J.; Hughes, T.L.; McCabe, S.E. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. Am. J. Public Health 2010, 100, 468–475. [Google Scholar] [CrossRef]
- Rich, A.J.; Armstrong, H.L.; Cui, Z.S.; Sereda, P.; Lachowsky, N.J.; Moore, D.M.; Hogg, R.S.; Roth, E.A. Sexual orientation measurement, bisexuality, and mental health in a sample of men who have sex with men in Vancouver, Canada. J. Bisex. 2018, 18, 299–317. [Google Scholar] [CrossRef]
- Ross, L.E.; Salway, T.; Tarasoff, L.A.; MacKay, J.M.; Hawkins, B.W.; Fehr, C.P. Prevalence of depression and anxiety among bisexual people compared to gay, lesbian, and heterosexual individuals: A systematic review and meta-analysis. J. Sex Res. 2018, 55, 435–456. [Google Scholar] [CrossRef] [Green Version]
- Berg, M.B.; Mimiaga, M.J.; Safren, S.A. Mental health concerns of HIV-infected gay and bisexual men seeking mental health services: An observational study. Aids Patient Care Stds 2004, 18, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Wang, S.H.; Qian, H.Z.; Ruan, Y.H.; Amico, K.R.; Vermund, S.H.; Yin, L.; Qiu, X.Q.; Zheng, S.M. Negative associations between general self-efficacy and anxiety/depression among newly HIV-diagnosed men who have sex with men in Beijing, China. Aids Care Psychol. Socio Med. Asp. Aids/HIV 2019, 31, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Vermund, S.H.; Lu, H.Y.; Ruan, Y.H.; Shepherd, B.E.; Kipp, A.M.; Amico, K.R.; Zhang, X.J.; Shao, Y.M.; Qian, H.Z. Impact of depression and anxiety on initiation of antiretroviral therapy among men who have sex with men with newly diagnosed HIV infections in china. Aids Patient Care Stds 2017, 31, 96–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, L.; Luo, D.; Chen, X.; Wang, M.; Zhou, W.; Zhang, D.X.; Xiao, S.Y. Longitudinal trajectories of emotional problems and unmet mental health needs among people newly diagnosed with HIV in china. J. Int. Aids Soc. 2019, 22, e25332. [Google Scholar] [CrossRef]
- Pakenham, K.I.; Rinaldis, M. Development of the HIV/aids stress scale. Psychol. Health 2002, 17, 203–219. [Google Scholar] [CrossRef]
- Niu, L.; Qiu, Y.Y.; Luo, D.; Chen, X.; Wang, M.; Pakenham, K.I.; Zhang, X.X.; Huang, Z.L.; Xiao, S.Y. Cross-culture validation of the HIV/aids stress scale: The development of a revised Chinese version. PLoS ONE 2016, 11, 12. [Google Scholar] [CrossRef]
- Xiao, S. The theory basis and application of the social support rating scale. J. Clin. Psychiatry Med. 1997, 4, 98–100. [Google Scholar]
- Ma, W.; Kang, D.; Song, Y.; Wei, C.; Marley, G.; Ma, W. Social support and HIV/STDs infections among a probability-based sample of rural married migrant women in Shandong province, china. BMC Public Health 2015, 15, 1170. [Google Scholar] [CrossRef] [Green Version]
- Xiaowen, W.; Guangping, G.; Ling, Z.; Jiarui, Z.; Xiumin, L.; Zhaoqin, L.; Hongzhuan, L.; Yuyan, Y.; Liyuan, Y.; Lin, L. Depression and anxiety mediate perceived social support to predict health-related quality of life in pregnant women living with HIV. AIDS Care 2018, 30, 1147–1155. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Patient Health Questionnaire, P. Validation and utility of a self-report version of prime-md—The PHQ primary care study. JAMA J. Am. Med. Assoc. 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Lowe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Manea, L.; Gilbody, S.; McMillan, D. A diagnostic meta-analysis of the patient health questionnaire-9 (phq-9) algorithm scoring method as a screen for depression. Gen. Hosp. Psychiatry 2015, 37, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Bian, Q.; Zhao, Y.; Li, X.; Wang, W.; Du, J.; Zhang, G.; Zhou, Q.; Zhao, M. Reliability and validity of the Chinese version of the patient health questionnaire (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2014, 36, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Lowe, B. A brief measure for assessing generalized anxiety disorder—The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Li, C.; Qian, J.; Cui, H.S.; Wu, W.Y. Reliability and validity of a generalized anxiety scale in general hospital outpatients. Shanghai Arch Psychiatry 2010, 22, 200–203. [Google Scholar]
- Tong, X.; An, D.; McGonigal, A.; Park, S.P.; Zhou, D. Validation of the generalized anxiety disorder-7 (gad-7) among Chinese people with epilepsy. Epilepsy Res. 2016, 120, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Halkitis, P.N.; Krause, K.D.; Vieira, D.L. Mental health, psychosocial challenges and resilience in older adults living with HIV. Interdiscip. Top. Gerontol. Geriatr. 2017, 42, 187–203. [Google Scholar] [PubMed]
- Rooks-Peck, C.R.; Adegbite, A.H.; Wichser, M.E.; Ramshaw, R.; Mullins, M.M.; Higa, D.; Sipe, T.A. Mental health and retention in HIV care: A systematic review and meta-analysis. Health Psychol. 2018, 37, 574–585. [Google Scholar] [CrossRef]
- Vreeman, R.C.; McCoy, B.M.; Lee, S. Mental health challenges among adolescents living with HIV. J. Int. AIDS Soc. 2017, 20, 21497. [Google Scholar] [CrossRef]
- Niu, L.; Luo, D.; Liu, Y.; Silenzio, V.M.B.; Xiao, S.Y. The mental health of people living with HIV in china, 1998-2014: A systematic review. PLoS ONE 2016, 11, 18. [Google Scholar] [CrossRef]
- Gelberg, L.; Andersen, R.M.; Leake, B.D. The behavioral model for vulnerable populations: Application to medical care use and outcomes for homeless people. Health Serv. Res. 2000, 34, 1273–1302. [Google Scholar] [PubMed]
- Churcher, S. Stigma related to HIV and aids as a barrier to accessing health care in Thailand: A review of recent literature. WHO South East Asia J. Public Health 2013, 2, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Stockton, M.A.; Giger, K.; Nyblade, L. A scoping review of the role of HIV-related stigma and discrimination in noncommunicable disease care. PLoS ONE 2018, 13, e0199602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadele, G.; Amde, W.K. Health needs, health care seeking behaviour, and utilization of health services among lesbians, gays and bisexuals in Addis Ababa, Ethiopia. Int. J. Equity Health 2019, 18, 86. [Google Scholar] [CrossRef]
- Courtenay-Quirk, C.; Wolitski, R.J.; Parsons, J.T.; Gomez, C.A.; Seropositive Urban Mens Study, T. Is HIV/aids stigma dividing the gay community? Perceptions of HIV-positive men who have sex with men. Aids Educ. Prev. 2006, 18, 56–67. [Google Scholar] [CrossRef] [Green Version]
- Ash, M.; Mackereth, C. Assessing the mental health and wellbeing of the lesbian, gay, bisexual and transgender population. Community Pract. 2013, 86, 24–27. [Google Scholar]
- McCann, E.; Sharek, D. Challenges to and opportunities for improving mental health services for lesbian, gay, bisexual, and transgender people in Ireland: A narrative account. Int. J. Ment. Health Nurs. 2014, 23, 525–533. [Google Scholar] [CrossRef]
- Lee, C.; Oliffe, J.L.; Kelly, M.T.; Ferlatte, O. Depression and suicidality in gay men: Implications for health care providers. Am. J. Mens Health 2017, 11, 910–919. [Google Scholar] [CrossRef]
- Parcesepe, A.M.; Mugglin, C.; Nalugoda, F.; Bernard, C.; Yunihastuti, E.; Althoff, K.; Jaquet, A.; Haas, A.D.; Duda, S.N.; Wester, C.W.; et al. Screening and management of mental health and substance use disorders in HIV treatment settings in low- and middle-income countries within the global iedea consortium. J. Int. Aids Soc. 2018, 21, e25101. [Google Scholar] [CrossRef]
- Cohen, M.S.; Chen, Y.Q.; Fleming, T.R.; Team, H.S. Prevention of HIV-1 infection with antiretroviral therapy reply. N. Engl. J. Med. 2011, 365, 493–505. [Google Scholar] [CrossRef] [Green Version]
- Nachega, J.B.; Mutamba, B.; Basangwa, D.; Nguyen, H.; Dowdy, D.W.; Mills, E.J.; Katabira, E.; Nakimuli-Mpungu, E. Severe mental illness at art initiation is associated with worse retention in care among HIV-infected ugandan adults. Trop. Med. Int. Health 2013, 18, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Velloza, J.; Celum, C.; Haberer, J.E.; Ngure, K.; Irungu, E.; Mugo, N.; Baeten, J.M.; Heffron, R.; Partners Demonstration, P. Depression and art initiation among HIV serodiscordant couples in Kenya and Uganda. Aids Behav. 2017, 21, 2509–2518. [Google Scholar] [CrossRef]
- Dutra, B.S.; Ledo, A.P.; Lins-Kusterer, L.; Luz, E.; Prieto, I.R.; Brites, C. Changes health-related quality of life in HIV-infected patients following initiation of antiretroviral therapy: A longitudinal study. Braz. J. Infect. Dis. 2019, 23, 211–217. [Google Scholar] [CrossRef]
- Huang, Y.; Luo, D.; Chen, X.; Zhang, D.; Huang, Z.; Xiao, S. HIV-related stress experienced by newly diagnosed people living with HIV in china: A 1-year longitudinal study. Int. J. Environ. Res. Public Health 2020, 17, 2681. [Google Scholar] [CrossRef] [Green Version]
- Rueda, S.; Mitra, S.; Chen, S.; Gogolishvili, D.; Globerman, J.; Chambers, L.; Wilson, M.; Logie, C.H.; Shi, Q.Y.; Morassaei, S.; et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/aids: A series of meta-analyses. BMJ Open 2016, 6, e011453. [Google Scholar] [CrossRef]
- Isay, R.A. Heterosexually married homosexual men: Clinical and developmental issues. Am. J. orthopsychiatry 1998, 68, 424–432. [Google Scholar] [CrossRef]
- Flowers, P.; Duncan, B.; Frankis, J. Community, responsibility and culpability: HIV risk-management amongst scottish gay men. J. Community Appl. Soc. Psychol. 2000, 10, 285–300. [Google Scholar] [CrossRef]
- Smit, P.J.; Brady, M.; Carter, M.; Fernandes, R.; Lamore, L.; Meulbroek, M.; Ohayon, M.; Platteau, T.; Rehberg, P.; Rockstroh, J.K.; et al. HIV-related stigma within communities of gay men: A literature review. Aids Care Psychol. Socio Med. Asp. Aids/HIV 2012, 24, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Cain, D.N.; Mirzayi, C.; Rendina, H.J.; Ventuneac, A.; Grov, C.; Parsons, J.T. Mediating effects of social support and internalized homonegativity on the association between population density and mental health among gay and bisexual men. LGBT Health 2017, 4, 352–359. [Google Scholar] [CrossRef] [Green Version]
- Tabler, J.; Mykyta, L.; Schmitz, R.M.; Kamimura, A.; Martinez, D.A.; Martinez, R.D.; Flores, P.; Gonzalez, K.; Marquez, A.; Marroquin, G.; et al. Getting by with a little help from our friends: The role of social support in addressing HIV-related mental health disparities among sexual minorities in the lower rio grande valley. J. Homosex. 2019, 14, 1–21. [Google Scholar] [CrossRef]
- Garrido-Hernansaiz, H.; Alonso-Tapia, J. Associations among resilience, posttraumatic growth, anxiety, and depression and their prediction from stress in newly diagnosed people living with HIV. J. Assoc. Nurses Aids Care 2017, 28, 289–294. [Google Scholar] [CrossRef]
- Khan, A.; Husain, A. Social support as a moderator of positive psychological strengths and subjective well-being. Psychol. Rep. 2010, 106, 534–538. [Google Scholar] [CrossRef]
- Liu, Y.; Ruan, Y.H.; Vermund, S.H.; Osborn, C.Y.; Wu, P.S.; Jia, Y.J.; Shao, Y.M.; Qian, H.Z. Predictors of antiretroviral therapy initiation: A cross-sectional study among Chinese HIV-infected men who have sex with men. BMC Infect. Dis. 2015, 15, 570. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.; Biello, K.; Rosenberger, J.G.; Novak, D.; Mayer, K.; Carey, K.; Mimiaga, M.J. The impact of social support and partner relationship dynamics on engagement in HIV care and antiretroviral treatment adherence among MSM in Latin America. Aids Care Psychol. Socio Med. Asp. Aids/HIV 2018, 30, 1406–1412. [Google Scholar] [CrossRef]
- Mao, Y.C.; Qiao, S.; Li, X.M.; Zhao, Q.; Zhou, Y.J.; Shen, Z.Y. Depression, social support, and adherence to antiretroviral therapy among people living with HIV in Guangxi, China: A longitudinal study. Aids Educ. Prev. 2019, 31, 38–50. [Google Scholar] [CrossRef]
- Assemie, M.A.; Alene, M.; Ketema, D.B.; Mulatu, S. Treatment failure and associated factors among first line patients on highly active antiretroviral therapy in Ethiopia: A systematic review and meta-analysis. Glob. Health Res. Policy 2019, 4, 32. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Gay Men (n = 171) | Bisexual Men (n = 87) | p |
|---|---|---|---|
| Age | |||
| 18–29 | 115 (67.3%) | 60 (69.0%) | 0.781 |
| >29 | 56 (32.7%) | 27 (31.0%) | |
| Marital status | |||
| Single | 141 (82.5%) | 62 (71.3%) | 0.048 |
| Married | 18 (10.5%) | 19 (21.8%) | |
| Divorced | 12 (7.0%) | 6 (6.9%) | |
| Employment | |||
| Employed | 111 (64.9%) | 57 (65.5%) | 0.565 |
| Unemployed | 60 (35.1%) | 30 (34.5%) | |
| Education background | |||
| Senior or lower | 70 (40.9%) | 38 (43.7%) | 0.673 |
| College or higher | 101 (59.1%) | 49 (56.3%) | |
| Monthly income (Yuan) | |||
| ≤4000 | 96 (56.1%) | 54(62.1%) | 0.361 |
| >4000 | 75 (43.9%) | 33 (37.9%) | |
| Living alone | |||
| Yes | 46 (26.9%) | 29 (33.3%) | 0.282 |
| No | 125 (73.1%) | 58 (66.7%) | |
| Children | |||
| With | 21 (12.3%) | 21 (24.1%) | 0.015 |
| Without | 150 (87.7%) | 66 (75.9%) | |
| HIV-related symptoms | |||
| With | 61 (35.7%) | 37 (42.5%) | 0.283 |
| Without | 110 (64.3%) | 50 (57.5%) | |
| CD4 counts (cells/mm3) | |||
| ≤350 | 66 (38.6%) | 40 (46.0%) | 0.255 |
| >350 | 105 (61.4%) | 47 (54.0%) | |
| ART initiation status | |||
| Yes | 38 (22.2%) | 36 (41.4%) | <0.001 |
| No | 133 (77.8%) | 51 (58.6%) | |
| Mental health care | |||
| Utilize | 11 (6.4%) | 17 (19.5%) | <0.001 |
| Not utilize | 160 (93.6%) | 70 (80.5%) |
| Psychosocial Characteristics | Baseline (n = 258) | Follow-Up (n = 258) | ||||
|---|---|---|---|---|---|---|
| Gay Men (n = 171) | Bisexual Men (n = 87) | p | Gay Men (n = 171) | Bisexual Men (n = 87) | p | |
| Depressive symptoms | ||||||
| No significant | 105 (61.4%) | 44 (50.6%) | 0.096 1 | 145 (84.8%) | 77 (88.5%) | 0.416 1 |
| Significant | 66 (38.6%) | 43 (49.4%) | 26 (15.2%) | 10 (11.5%) | ||
| Anxiety symptoms | ||||||
| No significant | 124 (72.5%) | 53 (60.9%) | 0.058 1 | 148 (86.5%) | 82 (94.3%) | 0.060 1 |
| Significant | 47 (27.5%) | 34 (39.1%) | 23 (13.5%) | 5 (5.7%) | ||
| PHQ-9 | 8 (4, 13) | 9 (4, 15) | 0.111 2 | 5 (1, 8) | 3 (1, 5) | 0.021 2 |
| GAD-7 | 6 (3, 10) | 7 (4, 13) | 0.101 2 | 4 (0, 7) | 2 (0, 5) | 0.021 2 |
| HIV/AIDS-related stress | 21 (14, 30) | 24 (13, 35) | 0.268 2 | 14 (8, 21) | 13 (6, 20) | 0.625 2 |
| Social stress | 12 (7, 16) | 12 (8, 16) | 0.394 2 | 7 (5, 13) | 6 (3, 11) | 0.097 2 |
| Emotional stress | 6 (3, 10) | 6 (3, 12) | 0.448 2 | 3 (1, 6) | 3 (1, 6) | 0.893 2 |
| Instrumental stress | 4 (1, 7) | 5 (2, 8) | 0.191 2 | 2 (1, 5) | 2 (0, 5) | 0.906 2 |
| Social support | 28 (23, 33) | 28 (23, 32) | 0.840 2 | 26 (20, 32) | 28 (22, 33) | 0.286 2 |
| Subjective support | 13 (10, 17) | 14 (11, 19) | 0.579 2 | 13 (11, 18) | 14 (11, 19) | 0.156 2 |
| Objective support | 8 (6, 10) | 8 (5, 9) | 0.432 2 | 6 (4, 8) | 6 (5, 7) | 0.750 2 |
| Support utilization | 6 (5, 7) | 6 (5, 7) | 0.896 2 | 6 (5, 7) | 6 (5, 8) | 0.455 2 |
| Psychosocial Characteristics | Change in Scores | p | |
|---|---|---|---|
| Gay Men (n = 171) | Bisexual Men (n = 87) | ||
| PHQ-9 | −2 (−7, 1) | −4 (−10, −1) | 0.001 |
| GAD-7 | −2 (−7, 1) | −4 (−9, −1) | 0.003 |
| HIV/AIDS-related stress | −6 (−15, 1) | −9 (−18, −1) | 0.105 |
| Social stress | −3 (−8, 2) | −5 (−9, 0) | 0.044 |
| Emotional stress | −2 (−6, 0) | −2 (−7, 0) | 0.376 |
| Instrumental stress | −1 (−4, 1) | −1 (−5, 1) | 0.270 |
| Social support | −1 (−6, 2) | 0 (−5, 4) | 0.381 |
| Subjective support | 0 (−4, 4) | 1 (−4, 5) | 0.357 |
| Objective support | −1 (−3, 1) | −1 (−3, 1) | 0.812 |
| Support utilization | 0 (−1, 1) | 0 (−1, 1) | 0.446 |
| Variables | Change in PHQ-9 | Change in GAD-7 | ||
|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | |
| Sexual orientation | ||||
| Bisexual | Ref | 0.041 | Ref | 0.027 |
| Gay | 1.61 (0.06, 3.14) | 1.54 (0.18, 2.91) | ||
| Mental health care | ||||
| Not utilize | Ref | 0.003 | Ref | <0.001 |
| Utilize | −3.51 (−5.80, −1.23) | -3.81 (−5.85, −1.79) | ||
| ART initiation status | ||||
| No | Ref | 0.008 | Ref | 0.006 |
| Yes | −2.14 (−3.71, −0.57) | −2.00 (−3.34, −0.56) | ||
| Change in social stress scores | 0.43 (0.32, 0.53) | <0.001 | 0.40 (0.30, 0.49) | <0.001 |
| Change in objective support scores | −0.37 (−0.57, −0.17) | <0.001 | −0.36 (−0.54, −0.18) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, R.; Silenzio, V.M.B.; Huang, Y.; Chen, X.; Luo, D. The Disparities in Mental Health Between Gay and Bisexual Men Following Positive HIV Diagnosis in China: A One-Year Follow-Up Study. Int. J. Environ. Res. Public Health 2020, 17, 3414. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103414
Luo R, Silenzio VMB, Huang Y, Chen X, Luo D. The Disparities in Mental Health Between Gay and Bisexual Men Following Positive HIV Diagnosis in China: A One-Year Follow-Up Study. International Journal of Environmental Research and Public Health. 2020; 17(10):3414. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103414
Chicago/Turabian StyleLuo, Rui, Vincent M.B. Silenzio, Yunxiang Huang, Xi Chen, and Dan Luo. 2020. "The Disparities in Mental Health Between Gay and Bisexual Men Following Positive HIV Diagnosis in China: A One-Year Follow-Up Study" International Journal of Environmental Research and Public Health 17, no. 10: 3414. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103414