In-Hospital Mortality in Patients Receiving Percutaneous Coronary Intervention According to Nurse Staffing Level: An Analysis of National Administrative Health Data


Abstract
:1. Introduction
2. Methods
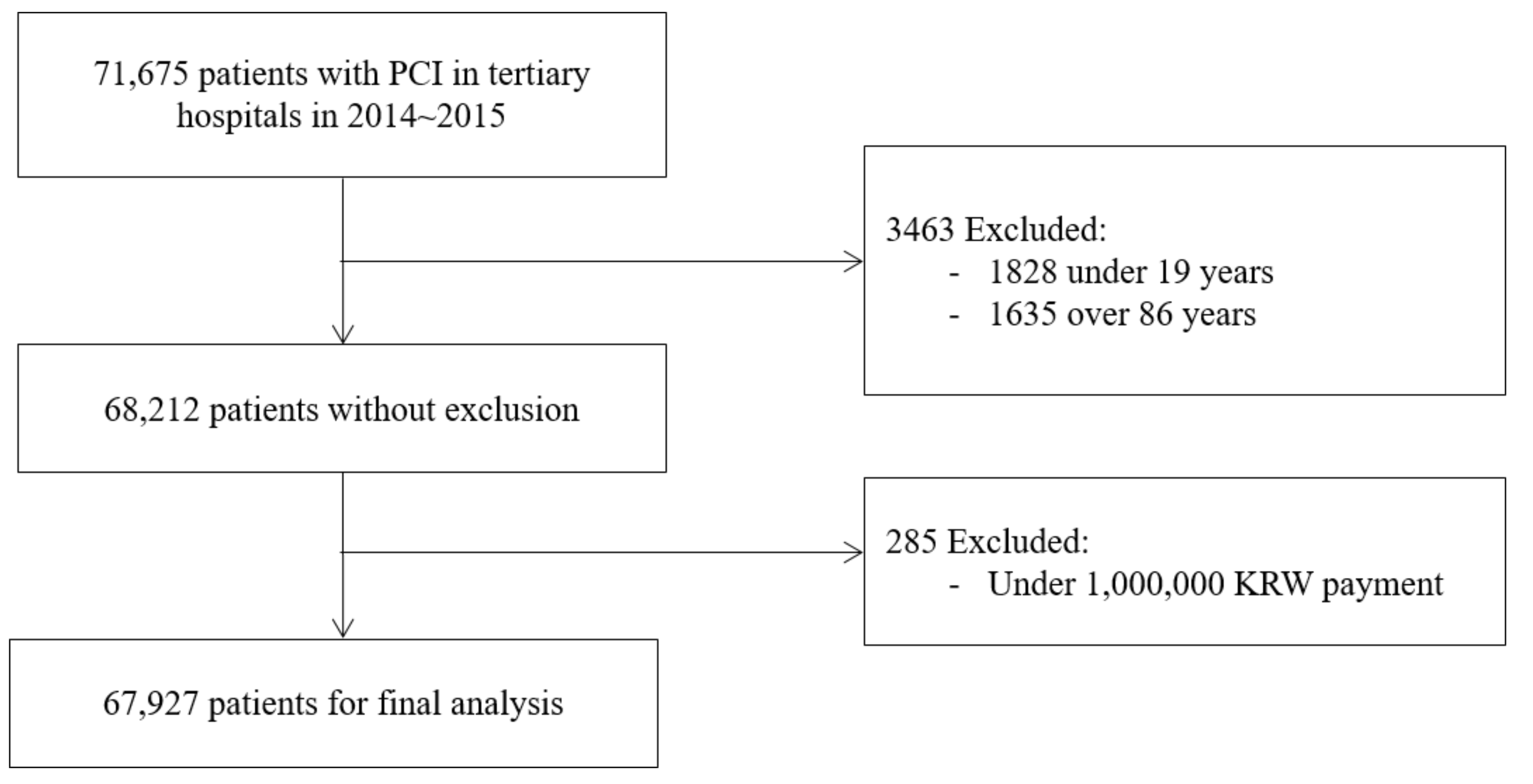
2.1. Data Source and Sample
2.2. Measurements
2.2.1. Nurse Staffing Level
2.2.2. Hospital Characteristics
2.2.3. Patient Characteristics
2.3. Data Analysis
2.4. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kim, J. Analysis of recent treatment trend of ischemic heart disease. HIRA Health Insur. Rev. Agency 2017, 11, 59–67. [Google Scholar]
- Kim, J.D.; Kang, Y.K. 2011 National Health Insurance Statistical Yearbook; HIRA (Health Insur. Rev. Agency)·NHIS (National Health Insurance Service): Seoul, Korea, 2012. [Google Scholar]
- Kim, Y.-I.; Kim, S.T. 2018 National Health Insurance Statistical Yearbook; HIRA (Health Insur. Rev. Agency)·NHIS (National Health Insurance Service): Wonju-Si, Korea, 2019. [Google Scholar]
- Korea, S. Causes of Death Statistics in 2018. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/6/2/index.board?bmode=read&bSeq=&aSeq=377606&pageNo=1&rowNum=10&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt= (accessed on 9 February 2020).
- Kim, Y.; Ahn, Y.; Cho, M.C.; Kim, C.J.; Kim, Y.J.; Jeong, M.H. Current status of acute myocardial infarction in Korea. Korean J. Intern. Med. 2019, 34, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Park, G.-M.; Kim, Y.-G.Y.-H.; Park, M.-W.; Her, S.H.; Lee, S.-W.; Kim, Y.-G.Y.-H. Trends, Characteristics, and Clinical Outcomes of Patients Undergoing Percutaneous Coronary Intervention in Korea between 2011 and 2015. Korean Circ. J. 2018, 48, 310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Person, S.D.; Allison, J.J.; Kiefe, C.I.; Weaver, M.T.; Williams, O.D.; Centor, R.M.; Weissman, N.W. Nurse Staffing and Mortality for Medicare Patients with Acute Myocardial Infarction. Med. Care 2004, 42, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.P.; Clark, A.M.; Dalal, H.; Welch, K.; Taylor, R.S. Patient education in the management of coronary heart disease. In Cochrane Database of Systematic Reviews; Brown, J.P., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2011. [Google Scholar]
- Kim, Y.; Kim, J. Impact of a financial incentive policy on Korean nurse staffing. Int. Nurs. Rev. 2015, 62, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-A. Reform of nursing differentiation fee regulation: For the development of hospital nursing. Webzine Daehankanho. 2007, 46, 1–4. [Google Scholar]
- Healthcare Resource Assessment Department Notification on How to Report According to the Partial Revision of the General Ward Nursing Care Fee Differential System. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020002000100&brdScnBltNo=4&brdBltNo=6762&pageIndex=1 (accessed on 15 May 2020).
- Ministry of Health and Welfare. National Health Insurance Act; Ministry of Health and Welfare: Seoul, Korea, 2019. [Google Scholar]
- h-well NHIS. Available online: https://www.nhis.or.kr/static/html/wbd/g/a/wbdga0302.html (accessed on 14 August 2019).
- Health Insurance Review & Assessment Service the Nursing Fee Differentiation Policy. Available online: http://rulesvcmr.hira.or.kr/service/law/lawFullScreenContent.do?seq=270&historySeq=18&type=0 (accessed on 3 January 2020).
- Kim, Y.; Kim, J.; Shin, S.A. Relationship between the legal nurse staffing standard and patient survival after perioperative cardiac arrest: A cross-sectional analysis of Korean administrative data. Int. J. Nurs. Stud. 2019, 89, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Rolley, J.X.; Davidson, P.M.; Salamonson, Y.; Fernandez, R.; Dennison, C.R. Review of nursing care for patients undergoing percutaneous coronary intervention: A patient journey approach. J. Clin. Nurs. 2009, 18, 2394–2405. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Kim, D.-H. Development of algorithm for nursing interventions after percutaneous coronary intervention. J. Korean Acad. Fundam. Nurs. 2017, 24, 18–29. [Google Scholar]
- Rolley, J.X.; Salamonson, Y.; Dennison, C.R.; Davidson, P.M. Nursing care practices following a percutaneous coronary intervention: Results of a survey of Australian and New Zealand cardiovascular nurses. J. Cardiovasc. Nurs. 2010, 25, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Throndson, K.; Sawatzky, J.-A.V. Improving outcomes following elective percutaneous coronary intervention: The key role of exercise and the advanced practice nurse. Can. J. Cardiovasc. Nurs. 2009, 19, 17–24. [Google Scholar] [PubMed]
- Throndson, K.; Sawatzky, J.A.V.; Schultz, A. Exploring the Perceptions and Health Behaviours of Patients Following an Elective Ad-hoc Percutaneous Coronary Intervention: A Qualitative Study. Can. J. Cardiovasc. Nurs. 2016, 26, 25–32. [Google Scholar] [PubMed]
- Griffiths, P.; Recio-Saucedo, A.; Dall’Ora, C.; Briggs, J.; Maruotti, A.; Meredith, P.; Smith, G.B.; Ball, J. The association between nurse staffing and omissions in nursing care: A systematic review. J. Adv. Nurs. 2018, 74, 1474–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aggarwal, B.; Ellis, S.G.; Lincoff, A.M.; Kapadia, S.R.; Cacchione, J.; Raymond, R.E.; Cho, L.; Bajzer, C.; Nair, R.; Franco, I.; et al. Cause of Death Within 30 Days of Percutaneous Coronary Intervention in an Era of Mandatory Outcome Reporting. J. Am. Coll. Cardiol. 2013, 62, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valaker, I.; Norekvål, T.M.; Råholm, M.-B.; Nordrehaug, J.E.; Rotevatn, S.; Fridlund, B. Continuity of care after percutaneous coronary intervention: The patient’s perspective across secondary and primary care settings. Eur. J. Cardiovasc. Nurs. 2017, 16, 444–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanic, V.; Vollrath, M.; Tapajner, A.; Sinkovic, A. Sex-Related 30-Day and Long-Term Mortality in Acute Myocardial Infarction Patients Treated with Percutaneous Coronary Intervention. J. Women’s Health 2017, 26, 374–379. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Category | Hospitals N (%) | Patients N (%) | Survival (%) | χ2 | p |
|---|---|---|---|---|---|---|
| Ownership | Public | 8 (18.6) | 13,927 (20.5) | 98.6 | 48.72 | <0.001 |
| Educational foundation | 30 (69.8) | 41,390 (60.9) | 98.7 | |||
| Medical corporation | 5 (11.6) | 12,610 (18.6) | 99.4 | |||
| Location | Seoul | 17 (39.6) | 29,845 (43.9) | 99.2 | 69.84 | <0.001 |
| Metropolitan | 13 (30.2) | 21,170 (31.2) | 98.5 | |||
| Small city | 13 (30.2) | 16,912 (24.9) | 98.5 | |||
| Number of PCI procedures | 62–999 | 13 (30.2) | 9470 (13.9) | 98.1 | 102.44 | <0.001 |
| 1000–1999 | 18 (41.9) | 24,337 (35.8) | 98.5 | |||
| ≥2000 | 12 (27.9) | 34,120 (50.2) | 99.2 | |||
| Number of beds per physician | <2.0 | 13 (30.2) | 27,228 (40.1) | 99.2 | 75.21 | <0.001 |
| <2.3 | 9 (20.9) | 10,901 (16.1) | 98.8 | |||
| ≥2.3 | 21 (48.8) | 29,798 (43.9) | 98.4 | |||
| Physician in charge of the ICU | No | 3 (7.0) | 1702 (2.5) | 98.5 | 1.05 | 0.305 |
| Yes | 40 (93.0) | 66,225 (97.5) | 98.8 | |||
| ICU nurse staffing | First grade | 7 (16.3) | 20,696 (30.5) | 99.5 | 123.21 | <0.001 |
| Second grade | 23 (53.5) | 32,036 (47.2) | 98.6 | |||
| Third grade | 11 (25.6) | 13,744 (20.2) | 98.3 | |||
| Fifth grade | 2 (4.7) | 1451 (2.1) | 97.7 | |||
| General-ward nurse staffing | First grade | 6 (14.0) | 15,440 (22.7) | 99.5 | 88.89 | <0.001 |
| Second grade | 19 (44.2) | 27,781 (40.9) | 98.7 | |||
| Third grade | 18 (41.9) | 24,706 (36.4) | 98.5 |
| Variable | Category | Patients N (%) | Survivors N (%) | χ2 | p |
|---|---|---|---|---|---|
| Sex | Male | 47,489 (69.9) | 46,967 (98.9) | 13.86 | <0.001 |
| Female | 20,438 (30.1) | 20,144 (98.6) | |||
| Age, years | 20–29 | 1038 (1.5) | 1035 (99.7) | 464.62 | <0.001 |
| 30–39 | 2281 (3.4) | 2277 (99.8) | |||
| 40–49 | 7205 (10.6) | 7172 (99.5) | |||
| 50–59 | 16,278 (24.0) | 16,188 (99.5) | |||
| 60–69 | 18,824 (27.7) | 18,691 (99.3) | |||
| 70–84 | 22,301 (32.8) | 21,748 (97.5) | |||
| Type of procedure | PCI with AMI | 17,534 (25.8) | 17,060 (97.3) | 576.12 | <0.001 |
| PCI without AMI accompanied by stent placement | 28,236 (41.6) | 28,101 (99.5) | |||
| PCI without AMI not accompanied by stent placement | 2982 (4.4) | 2949 (98.9) | |||
| PCI for arrhythmia therapy | 8667 (12.8) | 8665 (100.0) | |||
| Other PCIs | 10,508 (15.5) | 10,336 (98.4) | |||
| Disease severity | No complication or comorbidity | 50,018 (73.6) | 49,691 (99.4) | 479.45 | <0.001 |
| Minor complication or comorbidity | 12,990 (19.1) | 12,632 (97.2) | |||
| Moderate complication or comorbidity | 4919 (7.2) | 4788 (97.3) | |||
| Insurance type | Locally provided policyholder | 15,101 (22.2) | 14,951 (99.0) | 188.20 | <0.001 |
| Locally provided dependent | 5073 (7.5) | 4987 (98.3) | |||
| Employer-provided policyholder | 16,988 (25.0) | 16,930 (99.7) | |||
| Employer-provided dependent | 27,255 (40.1) | 26,798 (98.3) | |||
| Patient eligible for medical benefit | 3078 (4.5) | 3024 (98.3) | |||
| Dependent eligible for medical benefit | 432 (0.6) | 421 (97.5) | |||
| Admission path | Outpatient clinic | 43,143 (63.5) | 43,020 (99.7) | 836.29 | <0.001 |
| Emergency room | 24,784 (36.5) | 24,091 (97.2) | |||
| Admission to the ICU | No | 37,767 (55.6) | 37,648 (99.7) | 562.84 | <0.001 |
| Yes | 30,160 (44.4) | 29,463 (97.7) |
| Variable | Category | OR | (95% CI) | p |
|---|---|---|---|---|
| ICU nursing staff (ref = fifth grade) | First grade | 0.33 | (0.23–0.48) | <0.001 |
| Second grade | 0.55 | (0.40–0.77) | <0.001 | |
| Third grade | 0.71 | (0.53–0.95) | 0.022 | |
| General-ward nursing staff (ref = third grade) | First grade | 1.13 | (0.63–2.03) | 0.682 |
| Second grade | 1.00 | (0.73–1.35) | 0.985 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kim, J. In-Hospital Mortality in Patients Receiving Percutaneous Coronary Intervention According to Nurse Staffing Level: An Analysis of National Administrative Health Data. Int. J. Environ. Res. Public Health 2020, 17, 3799. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113799
Kim Y, Kim J. In-Hospital Mortality in Patients Receiving Percutaneous Coronary Intervention According to Nurse Staffing Level: An Analysis of National Administrative Health Data. International Journal of Environmental Research and Public Health. 2020; 17(11):3799. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113799
Chicago/Turabian StyleKim, Yunmi, and Jiyun Kim. 2020. "In-Hospital Mortality in Patients Receiving Percutaneous Coronary Intervention According to Nurse Staffing Level: An Analysis of National Administrative Health Data" International Journal of Environmental Research and Public Health 17, no. 11: 3799. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113799