Tailored Mental Health Literacy Training Improves Mental Health Knowledge and Confidence among Canadian Farmers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Training Program
2.1.2. Questionnaires
2.2. Statistical Analyses
3. Results
3.1. Participants
3.2. Participants’ Self-Reported Data
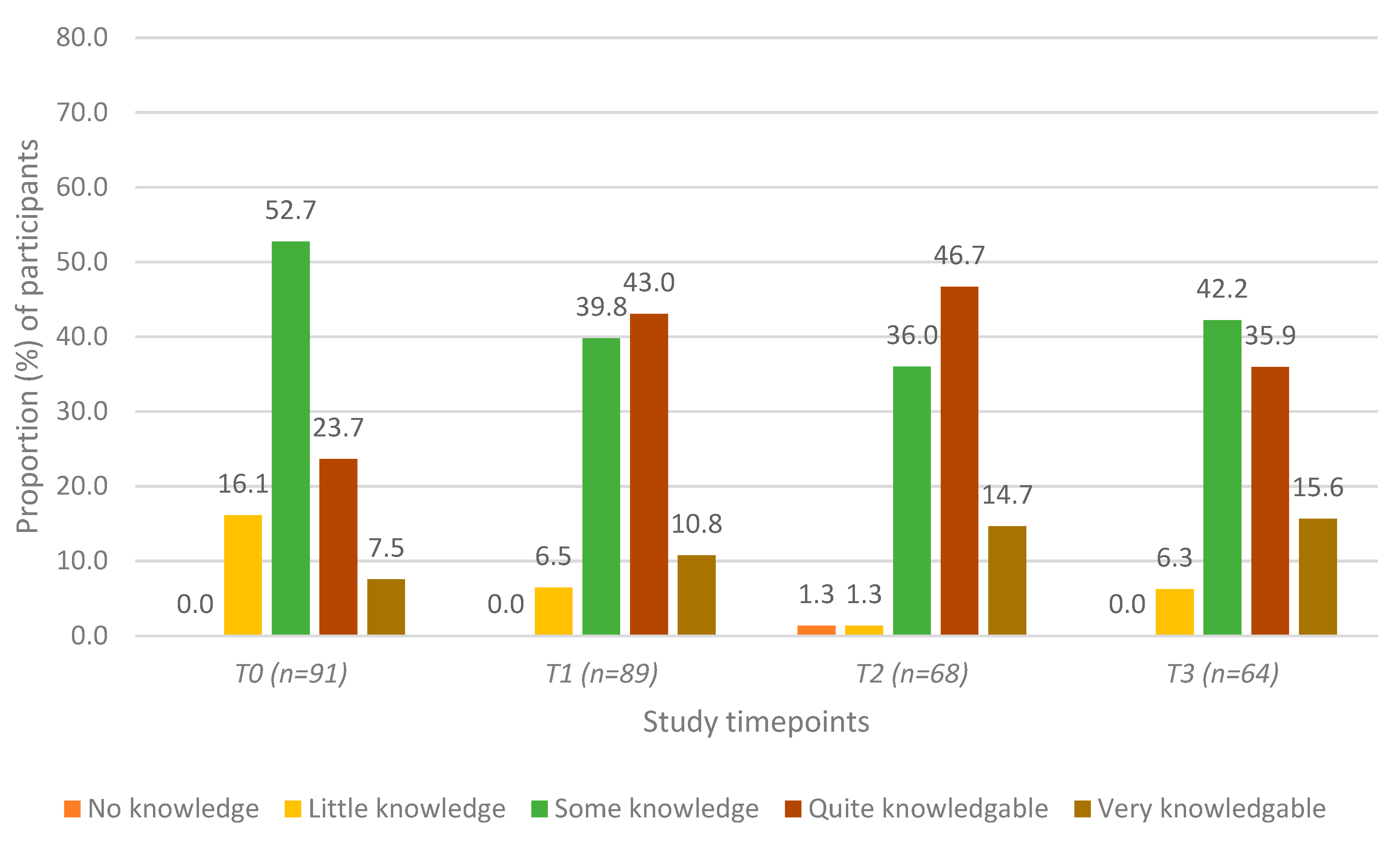
3.2.1. General Mental Health Knowledge
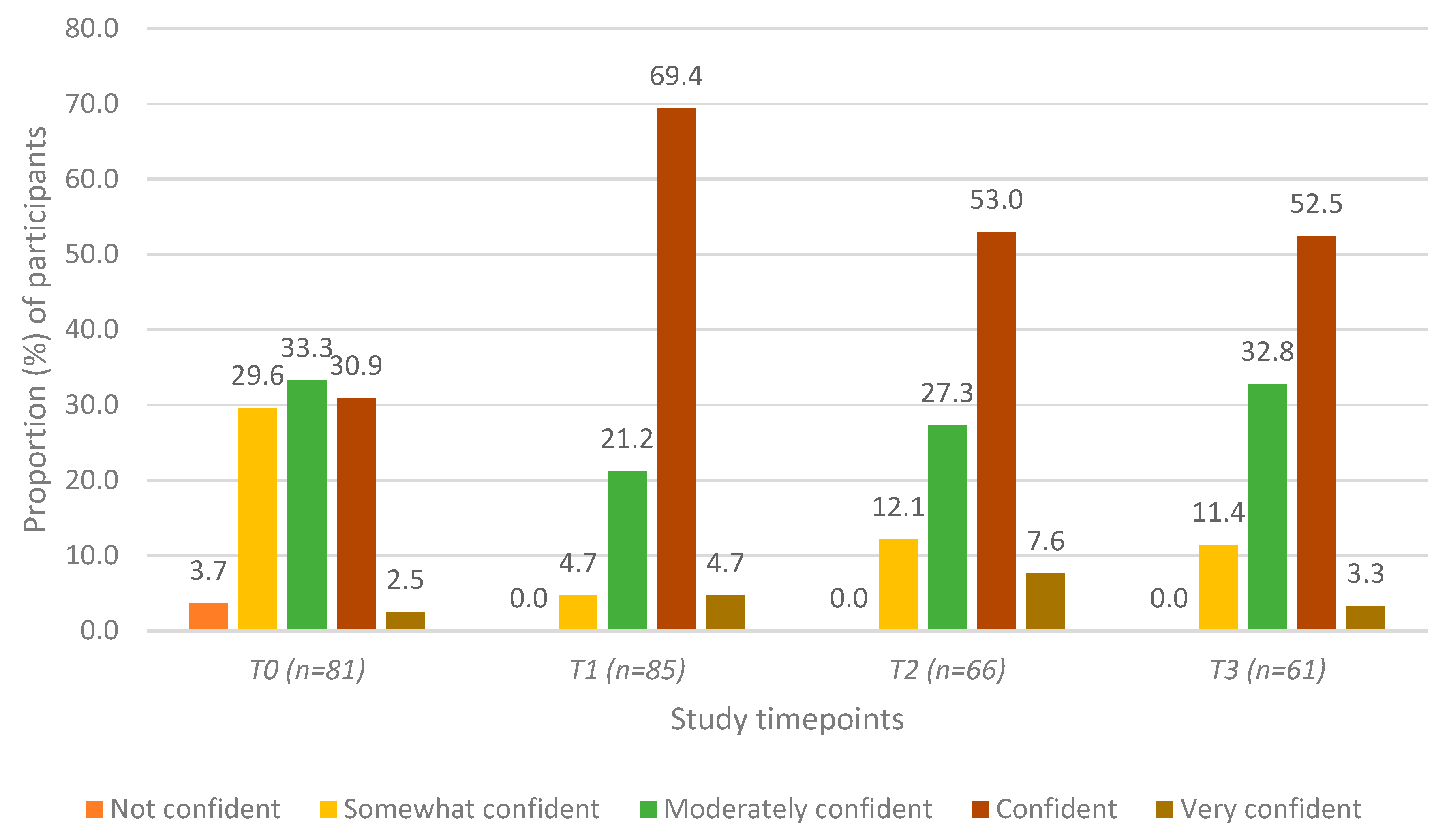
3.2.2. Confidence in Recognizing Mental Health Struggles in Others
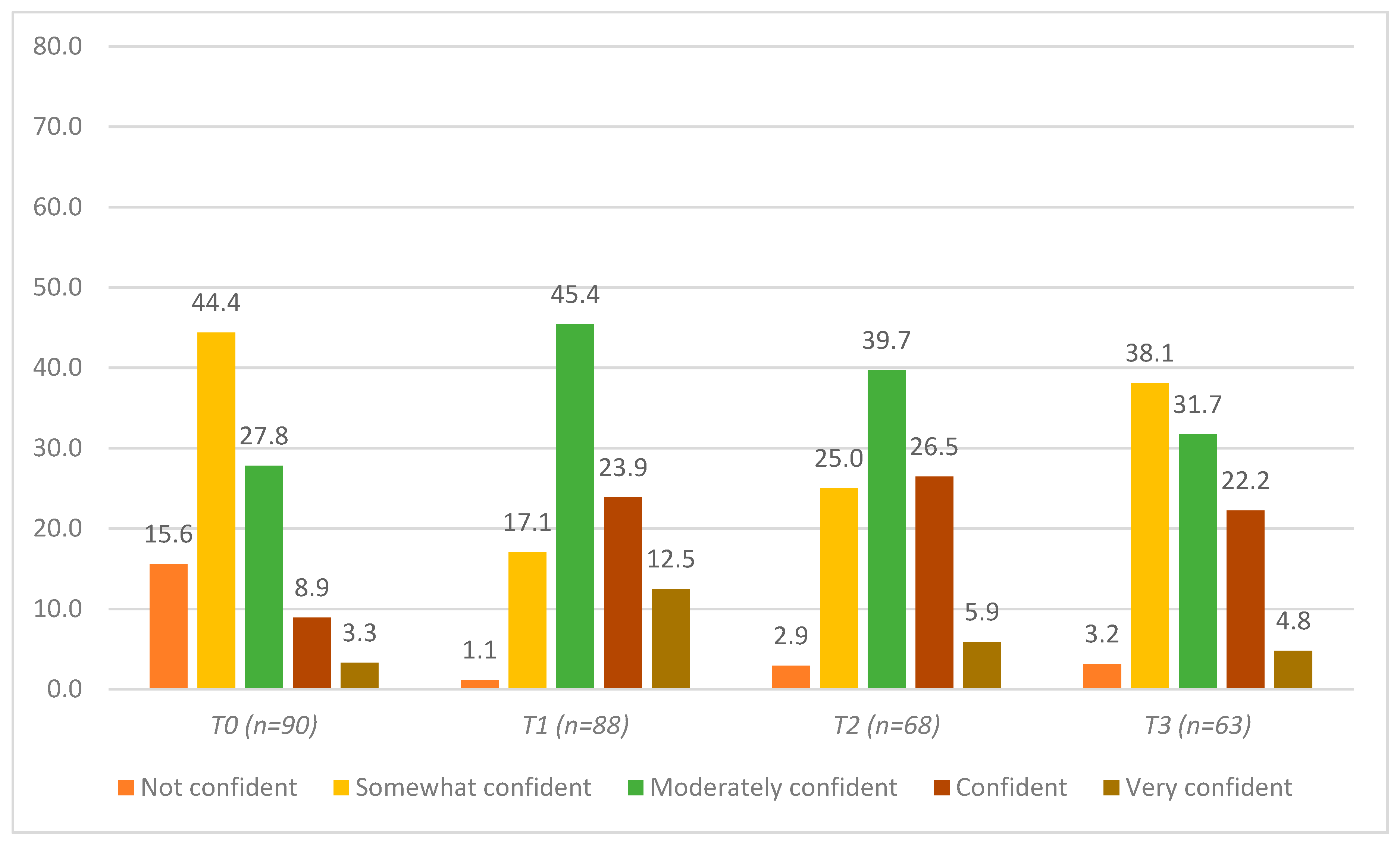
3.2.3. Confidence in Speaking to Others about Mental Health
3.2.4. Confidence in Helping Others Who May Be Struggling with Their Mental Health
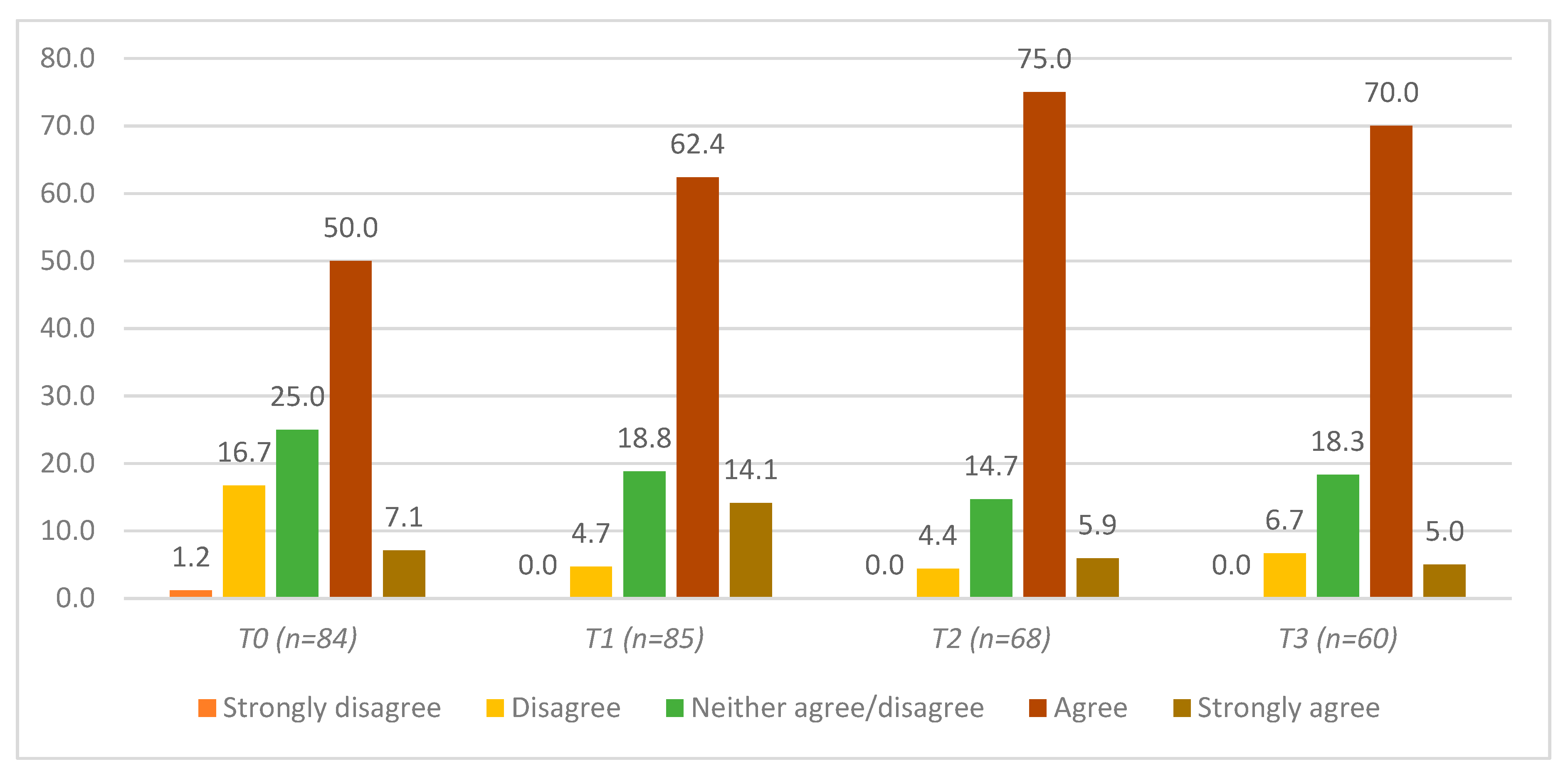
3.3. Participant Feedback on the Content, Helpfulness, Relevance, and Usefulness of “In the Know”
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Klingelschmidt, J.; Milner, A.; Khireddine-Medouni, I.; Witt, K.; Alexopoulos, E.C.; Toivanen, S.; La Montagne, A.D.; Chastang, J.-F.; Niedhammer, I.; J, K.; et al. Suicide among agricultural, forestry, and fishery workers: A systematic literature review and meta-analysis. Scand. J. Work. Environ. Health 2017, 44, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Parthasarathy, G.; Shameen. Suicides of cotton farmers in Andhra Pradesh: An exploratory study. Econ. Polit. Wkly. 1998, 33, 720–726. [Google Scholar]
- Jones-Bitton, A.; Best, C.; MacTavish, J.; Fleming, S.; Hoy, S. Stress, anxiety, depression, and resilience in Canadian farmers. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 55, 229–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peck, D.F.; Grant, S.; McArthur, W.; Godden, D. Psychological impact of foot-and-mouth disease on farmers. J. Ment. Health 2002, 11, 523–531. [Google Scholar] [CrossRef]
- Fraser, C.E.; Smith, K.B.; Judd, F.; Humphreys, J.S.; Fragar, L.J.; Henderson, A. Farming and mental health problems and mental illness. Int. J. Soc. Psychiatry 2005, 51, 340–349. [Google Scholar] [CrossRef]
- Staniford, A.K.; Dollard, M.F.; Guerin, B. Stress and help-seeking for drought-stricken citrus growers in the Riverland of South Australia. Aust. J. Rural. Health 2009, 17, 147–154. [Google Scholar] [CrossRef]
- Gerrard, N. An application of a community psychology approach to dealing with farm stress. Can. J. Community Ment. Health 2000, 19, 89–100. [Google Scholar] [CrossRef]
- Brumby, S.; Smith, A. ‘Train the Trainer’ Model: Implications for Health Professionals and Farm Family Health in Australia. J. Agromed. 2009, 14, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Rosmann, M.R. Sowing the seeds of hope: Providing regional behavioral health supports to the agricultural population. J. Agric. Saf. Health 2005, 11, 431–439. [Google Scholar] [CrossRef]
- Perceval, M.; Fuller, J.; Holley, A.-M. Farm-Link. Int. J. Ment. Health 2011, 40, 88–110. [Google Scholar] [CrossRef]
- Morgaine, K.C.; Thompson, L.; Jahnke, K.; Llewellyn, R. GoodYarn: Building mental health literacy in New Zealand’s rural workforce. J. Public Ment. Health 2017, 16, 180–190. [Google Scholar] [CrossRef]
- Kennedy, A.; Brumby, S.; Versace, V.; Brumby-Rendell, T. Online assessment of suicide stigma, literacy and effect in Australia’s rural farming community. BMC Public Health 2018, 18, 846. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; McGrath, P.; Hayden, J.A.; Kutcher, S. Mental health literacy measures evaluating knowledge, attitudes and help-seeking: A scoping review. BMC Psychiatry 2015, 15, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudolphi, J.M.; Barnes, K.L. Farmers’ Mental Health: Perceptions from a Farm Show. J. Agromed. 2019, 25, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Hadlaczky, G.; Hökby, S.; Mkrtchian, A.; Carli, V.; Wasserman, D. Mental Health First Aid is an effective public health intervention for improving knowledge, attitudes, and behaviour: A meta-analysis. Int. Rev. Psychiatry 2014, 26, 467–475. [Google Scholar] [CrossRef]
- Evans, R.E.; Craig, P.; Hoddinott, P.; Littlecott, H.; Moore, L.; Murphy, S.; O’Cathain, A.; Pfadenhauer, L.; Rehfuess, E.; Segrott, J.; et al. When and how do ‘effective’ interventions need to be adapted and/or re-evaluated in new contexts? The need for guidance. J. Epidemiol. Community Health 2019, 73, 481–482. [Google Scholar] [CrossRef] [Green Version]
- Hagen, B.; Albright, A.; Sargeant, J.; Winder, C.B.; Harper, S.L.; O’Sullivan, T.L.; Jones-Bitton, A. Research trends in farmers’ mental health: A scoping review of mental health outcomes and interventions among farming populations worldwide. PLoS ONE 2019, 14, e0225661. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, J.; Madden, K.; Fletcher, A.; Midgley, L.; Grant, A.; Cox, G.; Moore, L.; Campbell, R.; Murphy, S.; Bonell, C.; et al. Development of a framework for the co-production and prototyping of public health interventions. BMC Public HealTH 2017, 17, 689. [Google Scholar] [CrossRef]
- Massey, J.; Brooks, M.; Burrow, J. Evaluating the Effectiveness of Mental Health First Aid Training Among Student Affairs Staff at a Canadian University. J. Stud. Aff. Res. Pract. 2014, 51, 323–336. [Google Scholar] [CrossRef]
- Petrie, A.; Watson, P. Statistics for Veterinary and Animal Science, 2nd ed.; Blackwell Publishing: Oxford, UK, 2006. [Google Scholar]
- Jané-Llopis, E.; Barry, M.M. What makes mental health promotion effective? Promot. Educ. 2005, 12, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Richardson, R.; Dale, H.E.; Wellby, G.; McMillan, D.; Churchill, R. Mental Health First Aid as a tool for improving mental health and well-being. Cochrane Database Syst. Rev. 2018, 2018. [Google Scholar] [CrossRef]
- Baruch, Y. Response rate in academic studies—A comparative analysis. Hum. Relat. 1999, 52, 421–438. [Google Scholar] [CrossRef]
- Baruch, Y.; Holtom, B.C. Survey response rate levels and trends in organizational research. Hum. Relat. 2008, 61, 1139–1160. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Demographics | n (%) |
|---|---|
| Gender: | |
| Male | 35 (38.5) |
| Female | 52 (57.1) |
| Declined to answer | 4 (4.4) |
| Age: | |
| 18–29 | 16 (17.6) |
| 30–39 | 28 (30.8) |
| 40–49 | 18 (19.8) |
| 50–59 | 22 (24.2) |
| 60–69 | 5 (5.5) |
| 70+ | 2 (2.2) |
| Education: | |
| High school | 12 (13.0) |
| College diploma/university degree | 54 (59.3) |
| Graduate degree | 23 (25.3) |
| Declined to answer | 2 (2.2) |
| Agricultural Employment: | |
| Farmer | 34 (37.4) |
| Government extension agent | 8 (8.8) |
| Veterinarian | 4 (4.4) |
| Agronomist | 6 (6.6) |
| Administrative support | 4 (4.4) |
| Engineer | 3 (3.3) |
| Manager/team leader | 4 (4.4) |
| Graduate student/research assistant | 3 (3.3) |
| Livestock/production specialist | 6 (6.6) |
| Banker/insurance adjuster | 4 (4.4) |
| Consultant | 3 (3.3) |
| Other 1 | 8 (8.8) |
| Declined to answer | 4 (4.4) |
| Outcome | Pre-Training (T0) (n = 97) | Post-Training (T1) (n = 97) | 3 Months Post (T2) (n = 78) | 6 Months Post (T3) (n = 75) | |
|---|---|---|---|---|---|
| Row A. General mental health knowledge | Pre-training | - | <0.0001 | <0.0001 | 0.0003 |
| Post-training | <0.00011 | - | 0.732 | 0.8589 | |
| 3 months post | <0.0001 | 0.732 | - | 0.4962 | |
| 6 months post | 0.0003 | 0.8589 | 0.4962 | - | |
| Row B. Confidence recognizing mental health struggles | Pre-training | - | <0.0001 | <0.0001 | <0.0001 |
| Post-training | <0.0001 | - | 0.0285 | 0.0065 | |
| 3 months post | <0.0001 | 0.0285 | - | 0.9561 | |
| 6 months post | <0.0001 | 0.0065 | 0.9561 | - | |
| Row C. Comfort speaking to others about mental health | Pre-training | - | <0.0001 | 0.0004 | 0.0504 |
| Post-training | <0.0001 | - | 0.3743 | 0.1493 | |
| 3 months post | 0.0004 | 0.3743 | - | 1.0000 | |
| 6 months post | 0.0504 | 0.1493 | 1.0000 | - | |
| Row D. Comfort in helping others | Pre-training | - | <0.0001 | <0.0001 | <0.0001 |
| Post-training | <0.0001 | - | 0.0203 | <0.0001 | |
| 3 months post | <0.0001 | 0.0203 | - | 0.6469 | |
| 6 months post | <0.0001 | <0.0001 | 0.6469 | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagen, B.N.M.; Harper, S.L.; O’Sullivan, T.L.; Jones-Bitton, A. Tailored Mental Health Literacy Training Improves Mental Health Knowledge and Confidence among Canadian Farmers. Int. J. Environ. Res. Public Health 2020, 17, 3807. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113807
Hagen BNM, Harper SL, O’Sullivan TL, Jones-Bitton A. Tailored Mental Health Literacy Training Improves Mental Health Knowledge and Confidence among Canadian Farmers. International Journal of Environmental Research and Public Health. 2020; 17(11):3807. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113807
Chicago/Turabian StyleHagen, Briana N. M., Sherilee L. Harper, Terri L. O’Sullivan, and Andria Jones-Bitton. 2020. "Tailored Mental Health Literacy Training Improves Mental Health Knowledge and Confidence among Canadian Farmers" International Journal of Environmental Research and Public Health 17, no. 11: 3807. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113807