A Practical Approach to Using Integrated Knowledge Translation to Inform a Community-Based Exercise Study

 ,
,
Abstract
:1. Introduction
1.1. Cancer and Exercise Evidence
1.2. Research Context of the Clinical Team
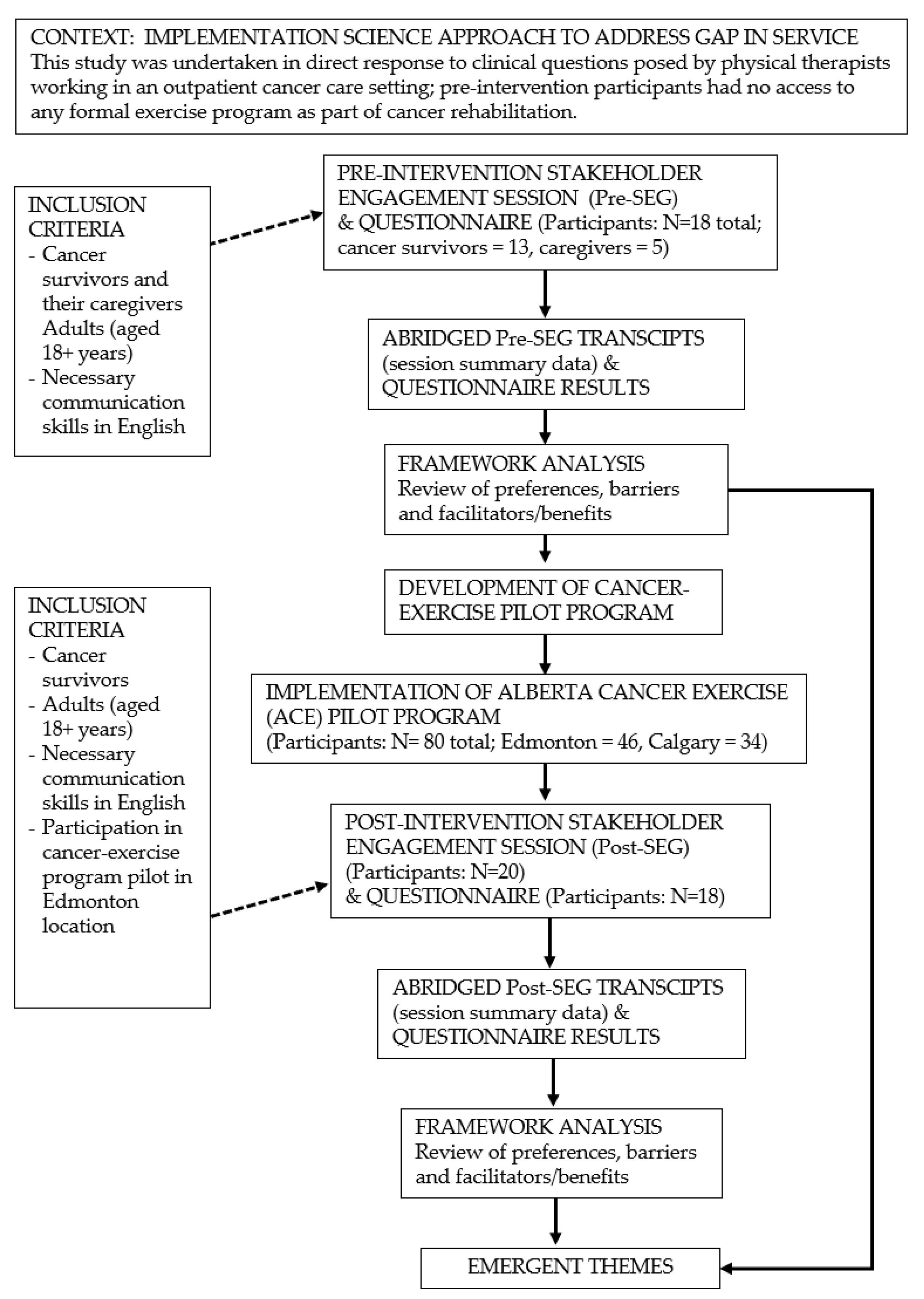
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Description of Participants
3.2. Pre-ACE Questionnaire Findings
3.3. Post-ACE Questionnaire Findings
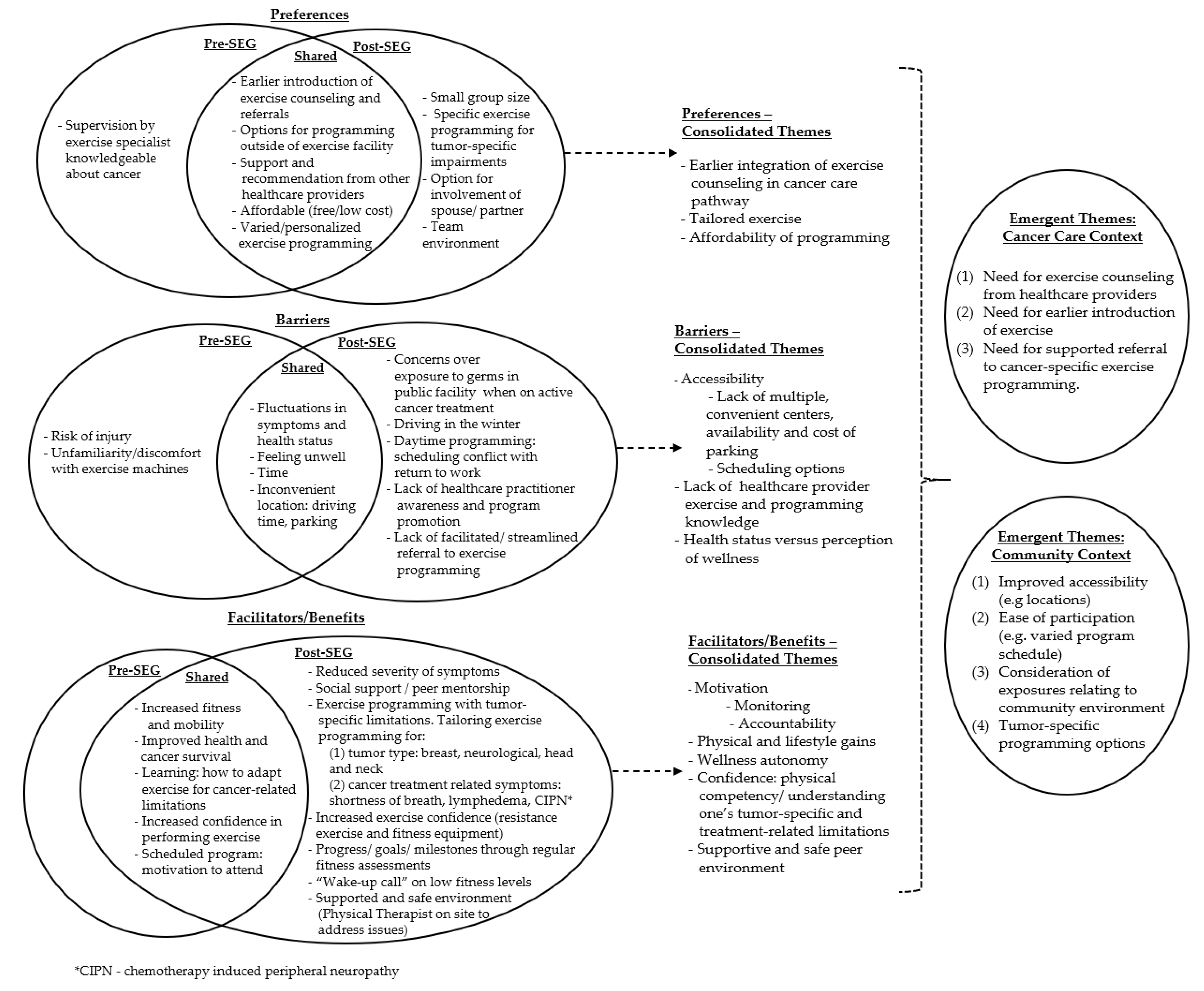
3.4. Stakeholder Engagement Group Findings
3.4.1. Exercise Preferences
“I may not have wanted or been able to take part in exercise when I was on treatment, but I would have liked to have known about the program and the option to take part later”.(ACE trial participant with lymphoma)
3.4.2. Barriers towards Exercise
“When I was on chemotherapy and my counts were low, I did not attend class”.(ACE trial participant with breast cancer)
3.4.3. Facilitators and Benefits of Exercise
“I knew it would be good for me, but I didn’t think I would look forward to going or enjoy the sessions”.(ACE trial participant with breast cancer)
“The program has given me the confidence to re-enter society”.(ACE trial participant with head and neck cancer)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Pre-ACE | Post-ACE |
|---|---|
| If Alberta’s Cancer Control were to develop a provincial cancer-specific exercise program, what should it look like? | If Alberta’s Cancer Control were to develop a provincial cancer-specific exercise program, what should it look like? |
| What do you think the benefits of participating in an exercise program would be? | What were the benefits of participating in the ACE pilot exercise program? Probe: Where there any benefits that you did not anticipate? |
| What do you feel are the main issues that might prevent you from taking part in an exercise program? | What do you feel are the main issues or barriers that might prevent you or others from taking part in the ACE program in the future? Probe: What could be done to overcome these issues? Probe: What were the negative aspects or drawbacks of participating in ACE? |
| If you were to participate in an exercise program, what types of exercise would you be most interested in doing? | If you were to participate in the ACE program again, what types of exercises would you be most interested in doing? |
| What aspects of an exercise program would be required for you to participate to comply with the program? | What components of the ACE program would motivate you to want to attend? |
| What elements would you like included in an exercise program that would motivate you to want to attend? | What aspects of the ACE program would be important to help you continue with an exercise program over the long-term? The grant funding will provide support to the ACE program for 4 years this includes resources to facilitate recruitment to the program, screening, exercise testing, referral, and exercise programming. How do you think the program should be funded over the long-term (beyond the grant funding period)? |
References
- Committee, C.C.S.A. Canadian Cancer Statistics 2019; Canadian Cancer Society: Toronto, ON, Canada, 2019. [Google Scholar]
- Hewitt, M.; Greenfield, S.; Stovall, E. From Cancer Patient to Cancer Survivor: Lost in Transition; National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Stout, N.L.; Silver, J.K.; Raj, V.S.; Rowland, J.; Gerber, L.; Cheville, A.; Ness, K.K.; Radomski, M.; Nitkin, R.; Stubblefield, M.D. Toward a national initiative in cancer rehabilitation: Recommendations from a subject matter expert group. Arch. Phys. Med. Rehabil. 2016, 97, 2006–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cormie, P.; Zopf, E.M.; Zhang, X.; Schmitz, K.H. The Impact of Exercise on Cancer Mortality, Recurrence, and Treatment-Related Adverse Effects. Epidemiol. Rev. 2017, 39, 71–92. [Google Scholar] [CrossRef] [PubMed]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E.; et al. American College of Sports Medicine Roundtable Report on Physical Activity, Sedentary Behavior, and Cancer Prevention and Control. Med. Sci. Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Blanchard, C.M.; Courneya, K.S.; Stein, K. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Boyle, T.; Vallance, J.; Ransom, E.; Lynch, B.; Vallance, J.K.; Ransom, E.K.; Lynch, B.M. How sedentary and physically active are breast cancer survivors, and which population subgroups have higher or lower levels of these behaviors? Support. Care Cancer 2016, 24, 2181–2190. [Google Scholar] [CrossRef]
- Mowls, D.; Brame, L.; Martinez, S.; Beebe, L.; Mowls, D.S.; Brame, L.S.; Martinez, S.A.; Beebe, L.A. Lifestyle behaviors among US cancer survivors. J. Cancer Surviv. 2016, 10, 692–698. [Google Scholar] [CrossRef]
- Chongya, N.; Eng, L.; Xin, Q.; Xiaowei, S.; Espin-Garcia, O.; Yuyao, S.; Pringle, D.; Mahler, M.; Halytskyy, O.; Charow, R.; et al. Lifestyle Behaviors in Elderly Cancer Survivors: A Comparison With Middle-Age Cancer Survivors. J. Oncol. Pract. 2015, 11, e450–e459. [Google Scholar]
- Schmitz, K.H.; Campbell, A.M. Exercise Is Medicine in Oncology: Engaging Clinicians to Help Patients Move Through Cancer. CA A Cancer J. Clin. 2019, 69, 468–484. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Cormie, P.; Atkinson, M.; Bucci, L.; Cust, A.; Eakin, E.; Hayes, S.; McCarthy, S.; Murnane, A.; Patchell, S.; Adams, D. Clinical Oncology Society of Australia position statement on exercise in cancer care. Med. J. Aust. 2018, 209, 184–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvão, D.A. The Exercise and Sports Science Australia position statement: Exercise medicine in cancer management. J. Sci. Med. Sport 2019, 22, 1175–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segal, R.; Zwaal, C.; Green, E.; Tomasone, J.R.; Loblaw, A.; Petrella, T. Exercise for people with cancer: A clinical practice guideline. Curr. Oncol. 2017, 24, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeely, M.L.; Culos-Reed, S.N. Alberta Cancer Exercise Pilot Randomized Trial (ACE). Available online: https://clinicaltrials.gov/ct2/show/NCT02330575 (accessed on 20 April 2020).
- McNeely, M.L.; Sellar, C.; Williamson, T.; Shea-Budgell, M.; Joy, A.A.; Lau, H.Y.; Easaw, J.C.; Murtha, A.D.; Vallance, J.; Courneya, K.; et al. Community-based exercise for health promotion and secondary cancer prevention in Canada: Protocol for a hybrid effectiveness-implementation study. BMJ Open 2019, 9, e029975. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Czosnek, L.; Rankin, N.; Zopf, E.; Richards, J.; Rosenbaum, S.; Cormie, P. Implementing Exercise in Healthcare Settings: The Potential of Implementation Science. Sports Med. 2020, 50, 1–14. [Google Scholar] [CrossRef]
- Karvinen, K.H.; Courneya, K.S.; Campbell, K.L.; Pearcey, R.G.; Dundas, G.; Capstick, V.; Tonkin, K.S. Exercise preferences of endometrial cancer survivors: A population-based study. Cancer Nurs. 2006, 29, 259–265. [Google Scholar] [CrossRef]
- ICES. Focus Groups in Health Services Research. In Institute for Clinical Evaluation Sciences; Ontario Ministry of Health: Toronto, ON, Canada, 1999; pp. 1–45. [Google Scholar]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Bryman, A.; Burgess, B. Analyzing Qualitative Data; Routledge: Abingdon, UK, 2002. [Google Scholar]
- Canadian Institutes of Health Research. Guide to Knowledge Translation Planning at CIHR: Integrated and End-of-Grant Approaches; Canadian Institutes of Health Research: Ottawa, ON, Canada, 2012. [Google Scholar]
- Fernandez, S.; Franklin, J.; Amlani, N.; DeMilleVille, C.; Lawson, D.; Smith, J. Physical activity and cancer: A cross-sectional study on the barriers and facilitators to exercise during cancer treatment. Can. Oncol. Nurs. J. 2015, 25, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Hardcastle, S.J.; Kane, R.; Chivers, P.; Hince, D.; Dean, A.; Higgs, D.; Cohen, P.A. Knowledge, attitudes, and practice of oncologists and oncology health care providers in promoting physical activity to cancer survivors: An international survey. Support. Care Cancer 2018, 26, 3711–3719. [Google Scholar] [CrossRef] [Green Version]
- Nyrop, K.A.; Deal, A.M.; Williams, G.R.; Guerard, E.J.; Pergolotti, M.; Muss, H.B. Physical activity communication between oncology providers and patients with early-stage breast, colon, or prostate cancer. Cancer 2016, 122, 470–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clifford, B.K.; Mizrahi, D.; Sandler, C.X.; Barry, B.K.; Simar, D.; Wakefield, C.E.; Goldstein, D. Barriers and facilitators of exercise experienced by cancer survivors: A mixed methods systematic review. Support. Care Cancer 2018, 26, 685–700. [Google Scholar] [CrossRef] [PubMed]
- Santa Mina, D.; Petrella, A.; Currie, K.L.; Bietola, K.; Alibhai, S.M.H.; Trachtenberg, J.; Ritvo, P.; Matthew, A.G. Enablers and barriers in delivery of a cancer exercise program: The Canadian experience. Curr. Oncol. 2015, 22, 374–384. [Google Scholar] [CrossRef] [Green Version]
- McNeely, M.L.; Dolgoy, N.; Onazi, M.; Suderman, K. The Interdisciplinary Rehabilitation Care Team and the Role of Physical Therapy in Survivor Exercise. Clin. J. Oncol. Nurs. 2016, 20, S8–S16. [Google Scholar] [CrossRef]
- Yang, D.D.; Hausien, O.; Aqeel, M.; Klonis, A.; Foster, J.; Renshaw, D.; Thomas, R. Physical activity levels and barriers to exercise referral among patients with cancer. Patient Educ. Couns. 2017, 100, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Suderman, K.; McIntyre, C.; Sellar, C.; McNeely, M.L. Implementing Cancer Exercise Rehabilitation: An Update on Recommendations for Clinical Practice. Curr. Cancer Ther. Rev. 2019, 15, 100–109. [Google Scholar] [CrossRef]
- Wong, J.N.; McAuley, E.; Trinh, L. Physical activity programming and counseling preferences among cancer survivors: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 48. [Google Scholar] [CrossRef] [Green Version]
- Demark-Wahnefried, W.; Aziz, N.M.; Rowland, J.H.; Pinto, B.M.; Demark-Wahnefried, W.; Aziz, N.M.; Rowland, J.H.; Pinto, B.M. Riding the crest of the teachable moment: Promoting long-term health after the diagnosis of cancer. J. Clin. Oncol. 2005, 23, 5814–5830. [Google Scholar] [CrossRef] [Green Version]
- Smith-Turchyn, J.; Richardson, J.; Tozer, R.; McNeely, M.; Thabane, L. Physical activity and breast cancer: A qualitative study on the barriers to and facilitators of exercise promotion from the perspective of health care professionals. Physiother. Can. 2016, 68, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Nadler, M.; Bainbridge, D.; Tomasone, J.; Cheifetz, O.; Juergens, R.; Sussman, J.; Juergens, R.A. Oncology care provider perspectives on exercise promotion in people with cancer: An examination of knowledge, practices, barriers, and facilitators. Support. Care Cancer 2017, 25, 2297–2304. [Google Scholar] [CrossRef]
- Fong, A.J.; Faulkner, G.; Jones, J.M.; Sabiston, C.M. A qualitative analysis of oncology clinicians’ perceptions and barriers for physical activity counseling in breast cancer survivors. Support. Care Cancer 2018, 26, 3117–3126. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W.; Courneya, K.S.; Fairey, A.S.; Mackey, J.R. Effects of an oncologist’s recommendation to exercise on self-reported exercise behavior in newly diagnosed breast cancer survivors: A single-blind, randomized controlled trial. Ann. Behav. Med. 2004, 28, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Culos-Reed, S.N.; Dew, M.; Shank, J.; Langelier, D.M.; McDonough, M. Qualitative Evaluation of a Community-Based Physical Activity and Yoga Program for Men Living With Prostate Cancer: Survivor Perspectives. Glob. Adv. Health Med. 2019, 8, 2164956119837487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leach, H.J.; Danyluk, J.M.; Nishimura, K.C.; Culos-Reed, S.N. Evaluation of a Community-Based Exercise Program for Breast Cancer Patients Undergoing Treatment. Cancer Nurs. 2015, 38, 417–425. [Google Scholar] [CrossRef] [PubMed]


| Participant Characteristics | Pre-Intervention | Post-Intervention |
|---|---|---|
| (n = 13; n = 5), No. (%) | (n = 20), No. (%) | |
| Sex | ||
| Male survivor | 4 (31) | 3 (15) |
| Caregiver | 1 | |
| Female survivor | 9 (69) | 17 (85) |
| Caregiver | 4 | |
| Age | ||
| 26–39 | 2 (15) | 1 (5) |
| 40–54 | 4 (31) | 6 (30) |
| 55–69 | 6 (46) | 7 (35) |
| >70 | 1 (8) | 6 (30) |
| Tumor Type | ||
| Breast | 7 (54) | 12 (60) |
| Caregiver | 1 | |
| Head and neck | 3 (23) | 4 (20) |
| Caregiver | 1 | |
| Lymphoma | 1 (8) | 1 (5) |
| Gastrointestinal | 2 (15) | 2 (10) |
| Caregiver | 1 | |
| Prostate | - | 1 (5) |
| Other | 1 | - |
| Caregiver multiple myeloma | ||
| Cancer Treatment | ||
| Surgery, radiation, chemotherapy | 7 (54) | 9 (45) |
| Surgery, radiation | 2 (15) | 7 (35) |
| Surgery, chemotherapy | 2 (15) | 2 (10) |
| Surgery alone | 1(8) | 1(5) |
| Chemotherapy alone | 1(8) | 1(5) |
| Location of Residence | ||
| Edmonton (urban) | 12 (67) | 16 (80) |
| Within 100 km of Edmonton | 5 (28) | 4 (20) |
| Rural > 100 kms | 1(5) | - |
| Preferences Related to Exercise Programming: n = 13 Survivors and n = 5 Caregivers | |||
| Where would you prefer to exercise? | Rank: 1. Community based, 2. Home based | ||
| What type of exercise would you like to do? | Rank: 1. Aerobic, 2. Walking, 3. Resistance exercise | ||
| How many times a week would you like to exercise? | Rank: 1. Two times per week; 2. Three times per week | ||
| How long would you like each session to last? | Rank: 1. One hour per session | ||
| What intensity of exercise would you prefer? | Rank: 1. Mild to moderate, 2. Moderate | ||
| Who would you prefer to exercise with? | Rank: 1. Other cancer survivors, 2. Partner/support person | ||
| Preferences Related to Exercise Counseling: n = 13 (%) | |||
| Did you receive counseling about exercise at any point from diagnosis to treatment completion? | Not discussed: 10 (77) | Survivor-initiated discussion: 0 (0) | Oncologist-initiated discussion: 3 (23) |
| Would you have preferred to be counseled about exercise? | Yes: 11 (85) | Maybe: 0 (0) | No: 2 (15) |
| When would you prefer this counseling? | Before/during treatment: 2 (15) | After treatment: 2 (15) | Multiple time points: 9 (69) |
| Where would you prefer this counseling to happen? | Cancer centre: 7 (54) | Community fitness centre: 2 (15) | Any location: 4 (31) |
| Who should provide the counseling? | Exercise specialist: 8 (62) | Health care provider: 3 (23) | Other cancer survivor: 2 (15) |
| What would be your preferred format of counseling? | Face to face: 10 (77) | Written materials: 2 (15) | Other: telephone/internet: 1 (1) |
| Barriers to Exercise (n = 18) | Facilitators (n = 18) | Benefits (n = 18) | |
| Lack of time Instructors unfamiliar with cancer Injury risk Intimidation/insecurity in public facility Feeling unwell Symptoms, e.g., fatigue Financial: cost of program Lack of personalized exercise programming | Instructor who is knowledgeable Instructor who is fun Convenient location Free parking, public transit access Support of other health care providers: nurse, physical therapist | Increases fitness Better health and overall survival Improved mobility Emotional support Better mental health Confidence in exercise | |
| Top Preferences Related to Exercise Programming (n = 18; Counts When More Than One Option Allowed) | |||
| Location of program (n = 21) | Community fitness centre: 12 (57%); home/outdoors: 7 (33%) | ||
| Type of exercise (n = 22) | Combined aerobic and resistance: 18 (82%) | ||
| Frequency and Duration (n = 22) | 2× or 3× per week: 16 (72%) | ||
| Duration (n = 22) | 50–60 min sessions: 16 (72%) | ||
| Intensity (n = 22) | Moderate intensity (not exhausting, light perspiration): 17 (77%) | ||
| Who would you prefer to exercise with? (n = 24) | Other cancer patients: 13 (54%), spouse/friend: 9 (38%) | ||
| Barriers to Exercise Participation (n = 18) | |||
| Never | Rarely–Occasionally | Often–Very Often | |
| Fatigue | 4 (22) | 11 (61) | 3 (17) |
| Lack of enjoyment | 11 (61) | 5 (28) | 2 (11) |
| Lack of self-discipline | 6 (33) | 11 (61) | 1 (6) |
| Pain | 7 (39) | 9 (50) | 2 (11) |
| Weather | 12 (67) | 4 (22) | 2 (11) |
| Exercise is boring | 14 (78) | 4 (22) | - |
| Muscle weakness | 6 (33) | 7 (39) | 5 (28) |
| Lack of time | 12 (67) | 5 (28) | 1 (6) |
| Lack of confidence in exercise abilities | 14 (78) | 4 (22) | - |
| Facilitators/Benefits of Exercise program on (n = 17) | |||
| Very Much—Slightly Worse | No Change—Slightly Improved | Somewhat—Very Much Approved | |
| Physical functioning | - | 2 (12) | 15 (88) |
| Muscle strength | - | 3 (18) | 14 (82) |
| Overall quality of life | - | 4 (24) | 13 (76) |
| Fatigue | - | 6 (35) | 11 (65) |
| Energy level | - | 6 (35) | 11 (65) |
| Ability to perform ADL | - | 7 (41) | 10 (59) |
| Treatment recovery | - | 8 (47) | 9 (53) |
| ACE Exercise Program Satisfaction (n = 17) | |||
| Not at All | A Little Bit/Somewhat | Quite a Bit/Very Much | |
| How beneficial was the program? | - | - | 17 (100) |
| How enjoyable was the program? | - | 2 (12) | 15 (88) |
| How supportive were your friends and family? | - | 2 (12) | 15 (88) |
| How motivated were you (to?) participate? | - | 3 (18) | 14 (82) |
| How difficult was it for you to participate? | 6 (35) | 11 (65) | - |
| How difficult will it be for you to continue to exercise? | 9 (53) | 7 (41) | 1 (6) |
| CONTEXT | THEME | ACTIONABLE ITEMS |
|---|---|---|
| Cancer Care Setting | Need for exercise counseling from health care provider |
|
| Need for earlier introduction of exercise | ||
| Need for supported referral to cancer-specific exercise programming | ||
| Community-Based Setting | Improved accessibility (e.g., locations) |
|
| Ease of participation (e.g., varied program schedule) | Where possible offer varied scheduling of cancer-specific exercise programming (e.g., morning/afternoon/evening options) | |
| Consideration of exposures relating to community environment |
| |
| Tumor-specific programming options | Development of subset programming to meet specific needs (e.g., breast, head and neck, neurological tumor-specific exercise programming) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suderman, K.; Dolgoy, N.; Yurick, J.; Sellar, C.; Nishimura, K.; Culos-Reed, S.N.; Joy, A.A.; McNeely, M.L. A Practical Approach to Using Integrated Knowledge Translation to Inform a Community-Based Exercise Study. Int. J. Environ. Res. Public Health 2020, 17, 3911. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113911
Suderman K, Dolgoy N, Yurick J, Sellar C, Nishimura K, Culos-Reed SN, Joy AA, McNeely ML. A Practical Approach to Using Integrated Knowledge Translation to Inform a Community-Based Exercise Study. International Journal of Environmental Research and Public Health. 2020; 17(11):3911. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113911
Chicago/Turabian StyleSuderman, Kirsten, Naomi Dolgoy, Janice Yurick, Christopher Sellar, Kathryn Nishimura, S. Nicole Culos-Reed, Anil A. Joy, and Margaret L. McNeely. 2020. "A Practical Approach to Using Integrated Knowledge Translation to Inform a Community-Based Exercise Study" International Journal of Environmental Research and Public Health 17, no. 11: 3911. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113911