The Relationship between Annual Airborne Pollen Levels and Occurrence of All Cancers, and Lung, Stomach, Colorectal, Pancreatic and Breast Cancers: A Retrospective Study from the National Registry Database of Cancer Incidence in Japan, 1975–2015

Abstract
:1. Introduction
2. Materials and Methods
3. Results
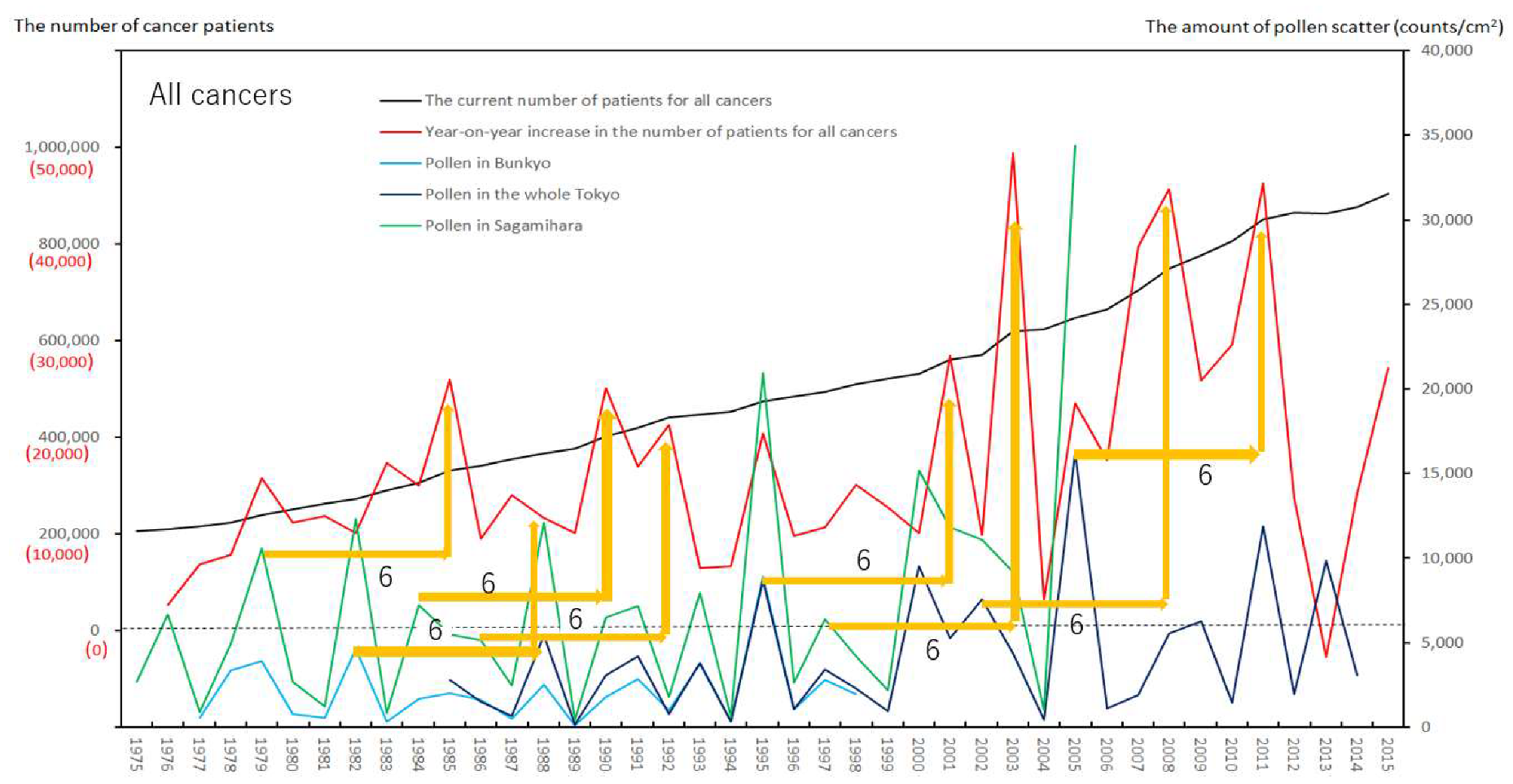
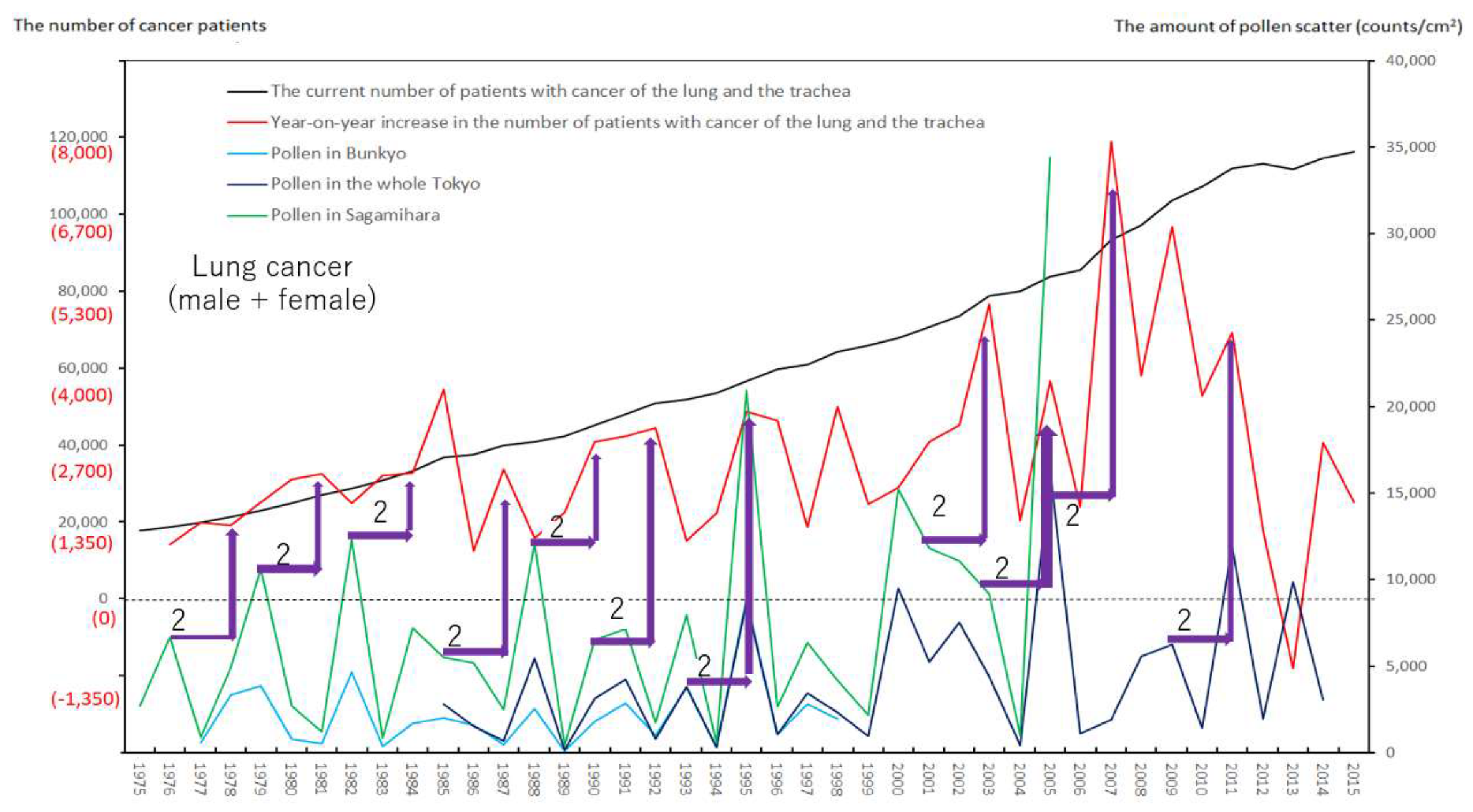
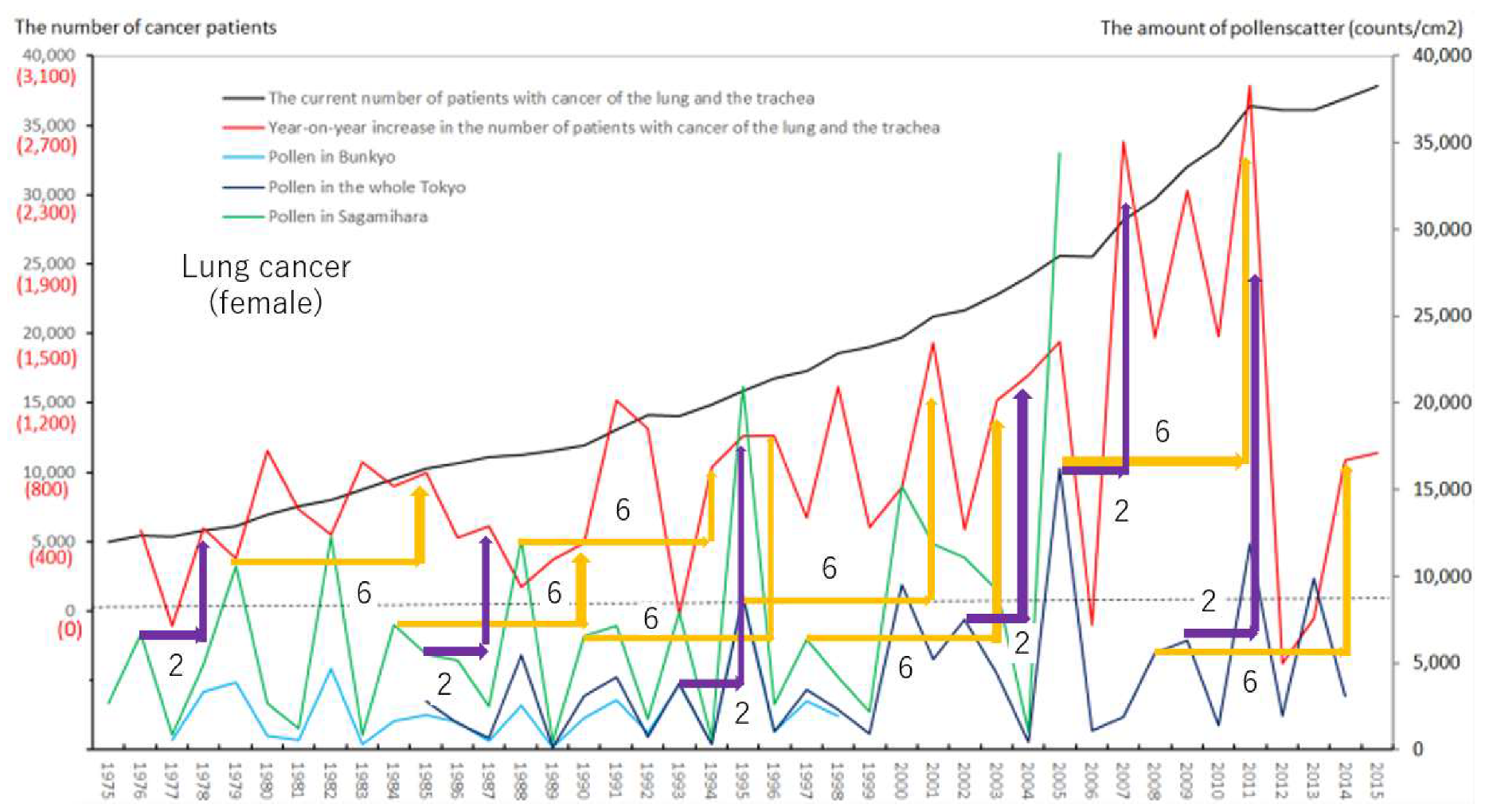
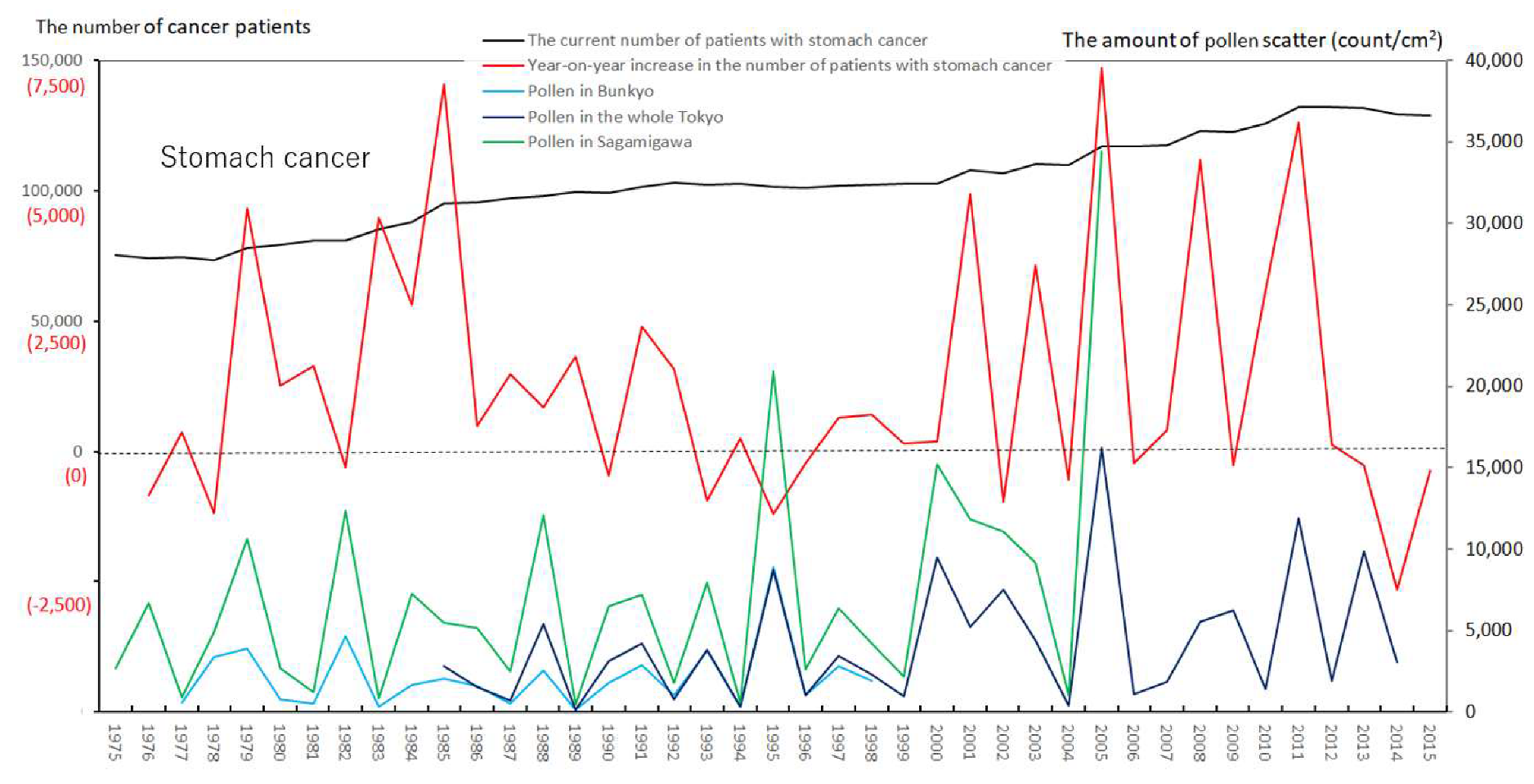
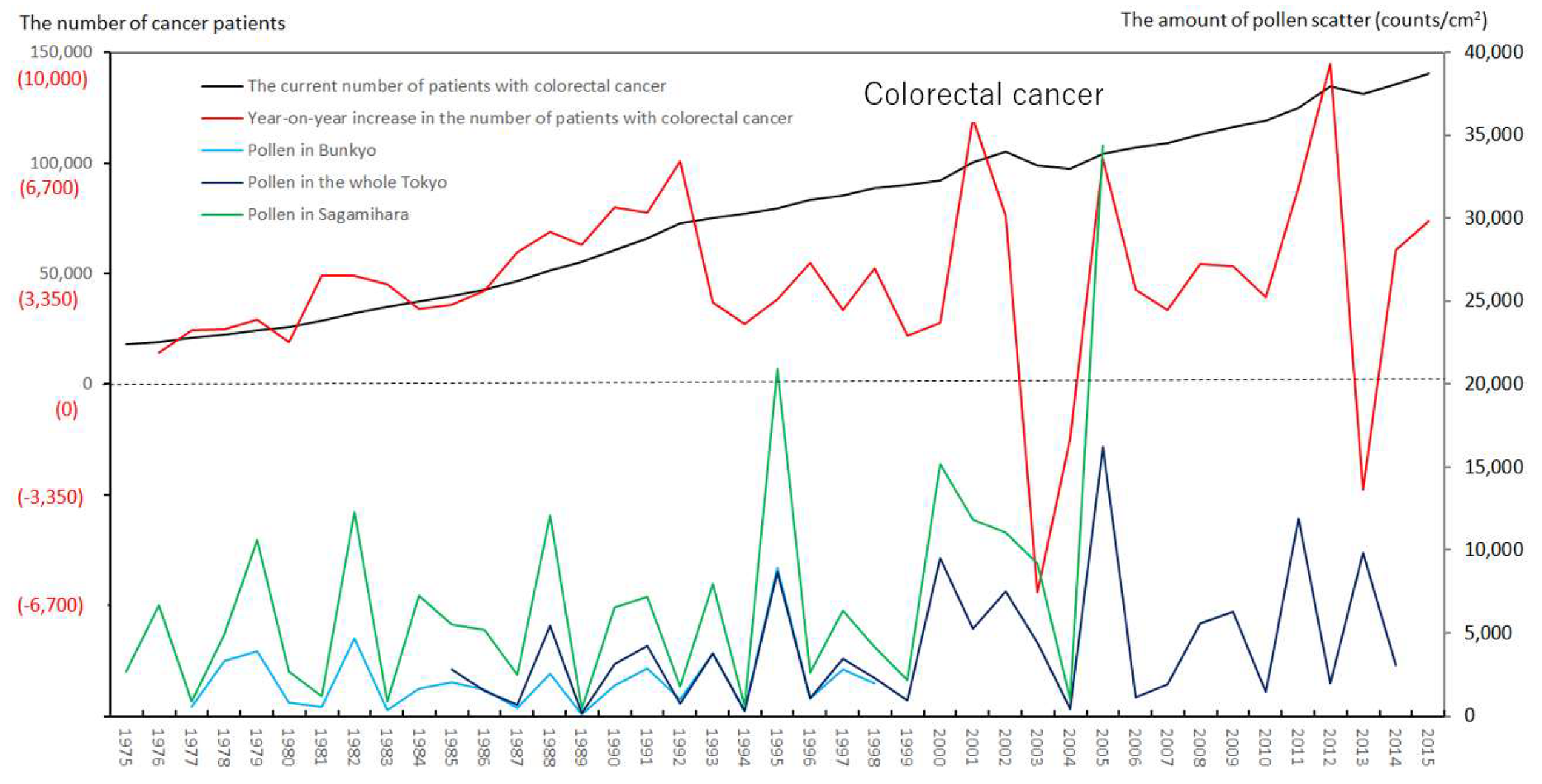
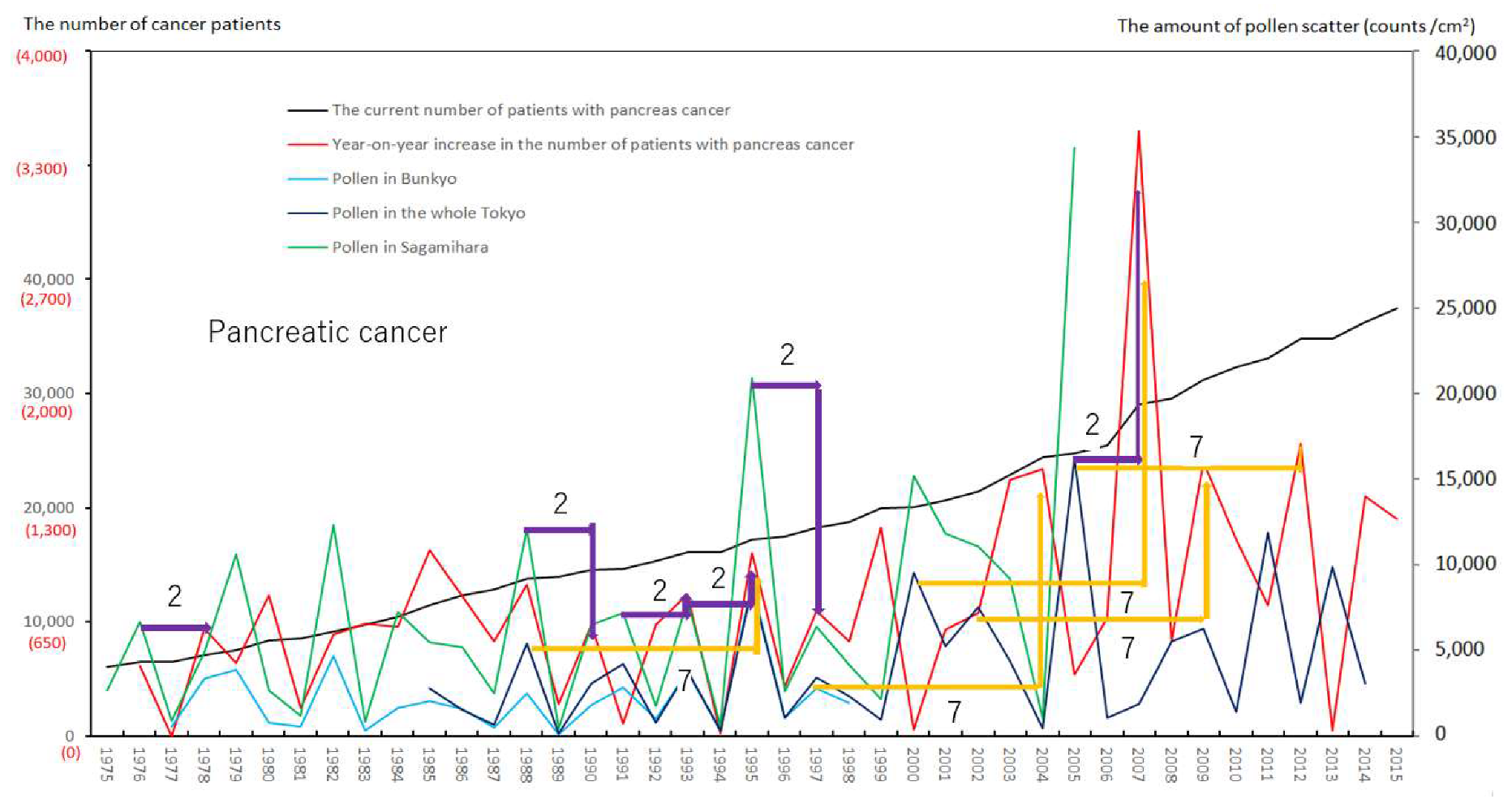
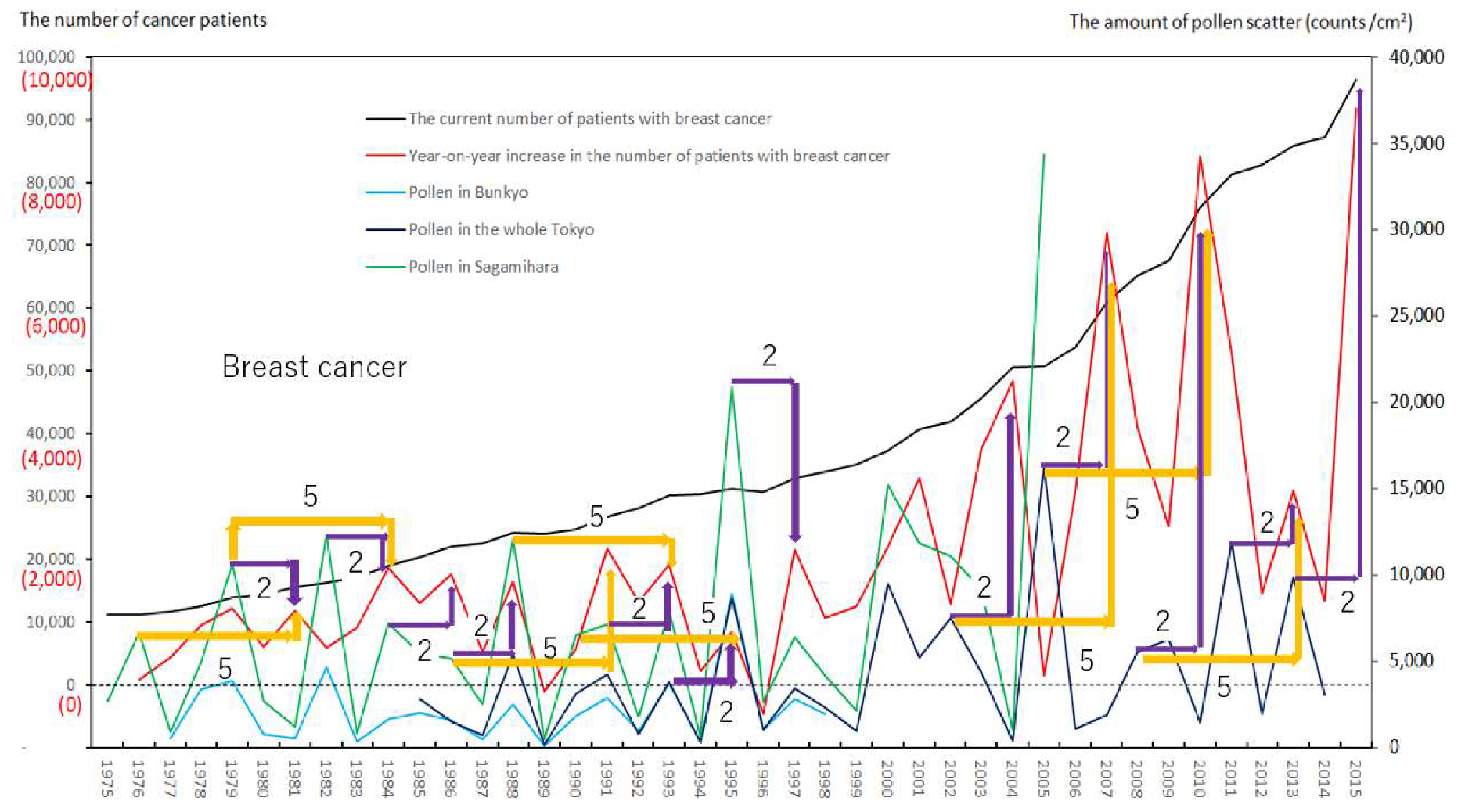
3.1. Upward Peaks in the Line Graphs of the Annual Number of Newly Registered Patients for All Cancers and for Each Cancer, in Relation to the Annual Levels of Airborne Pollen Scatter
3.2. Statistical Relationships between Newly Registered Patients in Each Patient-Registry Year and Airborne Pollen Levels Measured in the Same Year as or Prior to the Patient-Registry Year
4. Discussion
4.1. Trends in the Occurrence of Cancers Linked to Pollen Exposure
4.2. The Limits of Our Study, and Other Issues
4.3. Considerations for Taking Measures against Environmental Risk of Pollen Exposure
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AP | airborne pollen |
| CD | Crohn’s disease |
| DTH | delayed-type hypersensitivity |
| FH | fulminant hepatitis with intractable hepatitis |
| GPA | granulomatosis with polyangiitis |
| IBD | inflammatory bowel disease |
| IP | interstitial pneumonia |
| ITP | idiopathic thrombocytopenic purpura |
| KD | Kawasaki disease |
| LST | lymphocyte stimulation test |
| NCC | National Cancer Center |
| PAN | periarteritis nodosa |
| PBC | primary biliary cirrhosis |
| PE | pollen exposure |
| PID | pollen-induced diseases |
| RPs | registered patients |
| Sagamihara | Sagamihara City in Kanagawa Prefecture |
| SAP | severe acute pancreatitis |
| SIDs | specific intractable diseases |
| SLE | systemic lupus erythematosus |
| TAK | Takayasu arteritis |
| UC | ulcerative colitis7 |
References
- Cancer Statistics in Japan. Available online: https://ganjoho.jp/reg_stat/statistics/dl/index.html (accessed on 14 June 2017).
- Cancer Statistics in Japan 2016. Available online: https://ganjoho.jp/reg_stat/statistics/stat/annual.html (accessed on 14 June 2017).
- National Cancer Center for Public Health Sciences. Available online: https://www.ncc.go.jp/en/cpub/about/index.html (accessed on 1 July 2019).
- Sasazuki, S.; Inoue, M.; Shimazu, T.; Wakai, K.; Naito, M.; Nagata, C.; Tanaka, K.; Tsuji, I.; Sugawara, Y.; Mizoue, T.; et al. Development and evaluation of cancer prevention strategies in Japan. Evidence-based cancer prevention recommendations for Japanese. Jpn. J. Clin. Oncol. 2018, 48, 576–586. [Google Scholar] [CrossRef]
- Awaya, A.; Sahashi, N. The aetiology of Kawasaki disease: Does intense release of pollen induce pollinosis in constitutionally allergic adults, while constitutionally allergic infants develop Kawasaki disease? Biomed. Pharmacother. 2004, 58, 136–140. [Google Scholar] [CrossRef]
- Awaya, A.; Murayama, K. Positive correlation between Japanese cedar pollen numbers and the development of Kawasaki disease. Open Allergy J. 2012, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Awaya, A.; Nishimura, C. A combination of cross correlation and trend analyses reveals that Kawasaki disease is a pollen-induced delayed-type hyper-sensitivity disease. Int. J. Environ. Res. Public Health 2014, 11, 2628–2641. [Google Scholar] [CrossRef] [Green Version]
- Awaya, A. Suppressive influence of seasonal influenza epidemic on Kawasaki disease Onset. Jpn. J. Clin. Immunol. 2016, 39, 535–544. [Google Scholar] [CrossRef] [Green Version]
- Awaya, A. Development of many so-called autoimmune diseases including various vasculitis syndromes may be commonly triggered by pollen exposure Jacobs J. Allergy Immunol. 2018, 5, 026. [Google Scholar]
- Away, A. Proposal for construction of test and evaluation method in basic research and clinical study of medicines considering the effect of pollen exposure. Res. Drug Interact. 2020, 44, 1–8. [Google Scholar]
- Away, A.; Kuroiwa, Y. A Retrospective study on the relationship between annual airborne pollen levels during four Decades of 1975–2014 and annual occurrence of ulcerative colitis, Crohn’s disease, primary biliary cirrhosis, fulminant hepatitis, severe acute pancreatitis, interstitial pneumonia, amyloidosis, based on the National Registry Database of Specific Intractable Diseases in Japan. Arch. Epidemiol. Public Health 2019, 1. [Google Scholar] [CrossRef]
- Hori, M.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H. Cancer Incidence and Incidence Rates in Japan in 2009: A Study of 32 Population-Based Cancer Registries for the Monitoring of Cancer Incidence in Japan (MCIJ) Project. Available online: https://ganjoho.jp/reg_stat/statistics/dl/index.html (accessed on 31 July 2019).
- Observation Data on Release of Japanese Cedar Pollens and Japanese Cypress Pollens in Tokyo in Pollen Information by Tokyo Metropolitan Institute of Public Health. Available online: http://www.fukushihoken.metro.tokyo.jp/kanho/kafun/data/index.html (accessed on 31 July 2019).
- The Number of Patients Having Medical Certificates for Diseases Specified by the Japanese Government as Being Worrisome, Having No Known Treatment and of Unknown Causes. Available online: http://www.nanbyou.or.jp/entry/1356 (accessed on 1 June 2018). (In Japanese).
- Awaya, A. Pollen-Induced Diseases No.9; Prevention of Kawasaki Disease by Pollen Avoidance Life: Decrease of Recurrence Cases and Family Cases Are Criteria. Available online: https://www.yakuji.co.jp (accessed on 20 September 2017). (In Japanese).
- The 23rd National Surveillance Results on Kawasaki Disease. Available online: www.jichi.ac.jp/dph/kawasakibyou/20150924/mcls23report1013.pdf (accessed on 24 September 2015). (In Japanese).
- Bach, J.F.; Dardenne, M.; Pleau, J.M.; Rosa, J. Biochemical characterisation of a serum thymic factor. Nature 1977, 266, 55–57. [Google Scholar] [CrossRef]
- Nagai, Y.; Osanai, T.; Sakakibara, K. Intensive suppression of EAE by serum thymic factor and therapeutic implication for multiple sclerosis. Jpn. J. Exp. Med. 1982, 52, 213–219. [Google Scholar]
- Akira, A. The important role of melanin synthesis and metabolism systems in biodefense mechanisms, and development as foods with function claims of substances having equal bioactivities to a lead compound FTSnonapeptide in drug innovation. Cell 2017, 49, 676–677. (In Japanese) [Google Scholar]
- Zhao, X.H.; Awaya, A.; Tokumitsu, Y.; Nomura, Y. Effects of repeated administrations of Facteur Thymique Serique (FTS) on biochemical changes related to aging in senescence-accelerated mouse (SAM). Jpn. J. Pharmacol. 1990, 53, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, H.; Abe, H.; Awaya, A.; Inano, H.; Shikita, M. Serum thymic factor as a radioprotective agent promoting survival after X-Irradiation. Experientia 1990, 46, 484–486. [Google Scholar] [CrossRef]
- Kobayashi, H.; Abe, H.; Ueyama, T.; Awaya, A.; Shikita, M. Radioprotective effects of serum thymic factor in mice. Radiat. Res. 1992, 129, 351–356. [Google Scholar] [CrossRef]
- Mizutani, M.; El-Fotoh, M.; Awaya, A.; Matsumoto, Y.; Onodera, T. In vivo administration of serum thymic factor (FTS) prevents EMC-D virus-induced diabetes and myocarditis in BALB/cAJcl Mice. Arch. Virol. 1996, 141, 73–83. [Google Scholar] [CrossRef]
- Kato, M.; Tsuchiya, M.; Takeda, N.; Mochizuki, S.; Nagano, M.; Awaya, A. The effects of serum thymic factor (FTS) on cardiomyopathic hamster. J. Mol. Cell. Cardiol. 1995, 27, A534 (131). [Google Scholar]
- Kato, M.; Tsuchiya, M.; Takeda, N.; Mochizuki, S.; Nagano, M.; Awaya, A. Administration of serum thymic factor (FTS) on cardiomyopathic hamster. J. Mol. Cell. Cardiol. 1996, 28, A66 (260). [Google Scholar]
- Yamanouchi, T.; Moromizato, H.; Kojima, S.; Shinohara, T.; Miyashita, H.; Akaoka, I. Prevention of diabetes by thymic hormon in alloxane-treated rats. Eur. J. Pharmacol. 1994, 25, 739–746. [Google Scholar]
- Tada, H.; Nakashima, A.; Awaya, A.; Fujisaki, A.; Inoue, K.; Kawamura, K.; Itoh, K.; Masuda, H.; Suzuki, T. Effects of thymic hormone on reactive oxygen species-scavengers and renal function in tacrolimus-induced nephrotoxicity. Life Sci. 2002, 70, 1213–1223. [Google Scholar] [CrossRef]
- Kohda, Y.; Matsunaga, Y.; Yonogi, K.; Kawai, Y.; Awaya, A.; Gemba, M. Protective effect of serum thymic factor, FTS, on cephaloridine-induced nephrotoxicity in rats. Biol. Pharm. Bull. 2005, 28, 2087–2091. [Google Scholar] [CrossRef] [Green Version]
- Kohda, Y.; Kawai, Y.; Iwamoto, N.; Matsunaga, Y.; Aiga, H.; Awaya, A.; Gemba, M. Serum thymic factor, FTS, attenuates cisplatin nephrotoxicity by suppressing cisplatin-induced ERK activation. Biochem. Pharmacol. 2005, 70, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Inagaki-Ohara, K.; Kobayashi, N.; Awaya, A.; Yoshikai, Y. Effects of a nonapeptide thymic hormone on intestinal intraepithelial lymphocytes in mice following administraion of 5-Fluorouracil. Cell. Immunol. 1996, 171, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Yamada, H.; Yoshihara, K.; Awaya, A.; Yoshikai, Y. In vivo treatment with a nonapeptide thymic hormone, Facteur Thymique Serique (FTS), ameliorates chronic colitis induced by dextran sulphate Sodium in Mice. Int. Immunopharmacol. 2007, 7, 928–936. [Google Scholar] [CrossRef]
- Yara, S.; Kawakami, K.; Awaya, A.; Saito, A. FTS reduces bleomycin-induced cytokine and chemokine production and inhibits pulmonary fibrosis in mice. Clin. Exp. Immunol. 2001, 124, 77–85. [Google Scholar] [CrossRef]
- Hirai, N.; Furuyama, H.; Awaya, A.; Onuma, M. Effect of administration of serum thymic factor (FTS) in calves and rabbits infected with bovine immunodeficiency-like virus. J. Vet. Med. Sci. 1995, 57, 307–310. [Google Scholar] [CrossRef] [Green Version]
- Onodera, T.; Yoshihara, K.; Awaya, A.; Yukawa, M. Resistance to pseudorabies virus with enhanced interferon production and natural killer cell activity in mice treated with serum thymic factor. Microbiol. Immunol. 1994, 38, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Onodera, T.; Taniguchi, T.; Awaya, A.; Hayashi, T. Thymic atrophy in type 2 reovirus infected mice: Immunosuppression and effects of thymic hormone. Thymic Atrophy Caused reo-2. Thymus 1991, 18, 95–109. [Google Scholar]
- Miyauchi, M.; Koshikawa, N.; Awaya, A.; Maruyama, K. Augmentation with serum thymic factor of suppressive effects on retroviral tumor development in hosts immune to V-onc product. Leukemia 1997, 11, 213–215. [Google Scholar]
- Fuchikami, J.; Chihara, M.; Takahashi, M.; Saitou, A.; Ikezawa, K.; Fujino, A.; Awaya, A. Effect of serum thymic factor (FTS) on antigen induced early and late phase nasal blockage in a Guinea pig model of allergic rhinitis. J. Pharmacol. Sci. 2006, 100, 231. [Google Scholar]
- Imai, S.-I.; Guarente, L. NAD+ and sirtuins in aging and disease. Trends Cell Biol. 2014, 24, 464–471. [Google Scholar] [CrossRef]
- Cellular Canceration Mechanism. Available online: https://ganjoho.jp/public/dia_tre/knowledge/cancerous_change.html (accessed on 21 December 2017).
- Awaya, A.; Sugane, K.; Yamauchi, J. Stimulation of lymphocytes of patients administered with a trypsin inhibitor, trasylol (basic pancreatic trypsin inhibitor pharmaceutical), In vitro with BPTI and other several stimulants. Jpn. J. Exp. Med. 1975, 45, 541–549. [Google Scholar]
- Awaya, A.; Takeuchi, T.; Saito, T. Studies on a patient whose lymphocytes were stimulated in vitro with aprotinin in spite of having no history of therapy with aprotinin preparation. Rinshomeneki 1979, 10, 1093–1100. (In Japanese) [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| α | All Cancers | Lung Cancer Male + Female) | Lung Cancer (Male) | Lung Cancer (Female) | Stomach Cancer | Colorectal Cancer | Pancreatic Cancer | Breast Cancer | |
|---|---|---|---|---|---|---|---|---|---|
| 0 | T | ||||||||
| S | |||||||||
| 1 | T | ||||||||
| S | |||||||||
| 2 | T | 0.03 * | 0.008 ** | ||||||
| S | 0.008 ** | 0.02 * | 0.07 † | 0.00003 **** | 0.002 *** | ||||
| 3 | T | ||||||||
| S | |||||||||
| 4 | T | ||||||||
| S | |||||||||
| 5 | T | ||||||||
| S | 0.04 * | ||||||||
| 6 | T | 0.08 † | |||||||
| S | 0.04 * | 0.07 † | |||||||
| 7 | T | 0.05 † | |||||||
| S |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Awaya, A.; Kuroiwa, Y. The Relationship between Annual Airborne Pollen Levels and Occurrence of All Cancers, and Lung, Stomach, Colorectal, Pancreatic and Breast Cancers: A Retrospective Study from the National Registry Database of Cancer Incidence in Japan, 1975–2015. Int. J. Environ. Res. Public Health 2020, 17, 3950. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113950
Awaya A, Kuroiwa Y. The Relationship between Annual Airborne Pollen Levels and Occurrence of All Cancers, and Lung, Stomach, Colorectal, Pancreatic and Breast Cancers: A Retrospective Study from the National Registry Database of Cancer Incidence in Japan, 1975–2015. International Journal of Environmental Research and Public Health. 2020; 17(11):3950. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113950
Chicago/Turabian StyleAwaya, Akira, and Yoshiyuki Kuroiwa. 2020. "The Relationship between Annual Airborne Pollen Levels and Occurrence of All Cancers, and Lung, Stomach, Colorectal, Pancreatic and Breast Cancers: A Retrospective Study from the National Registry Database of Cancer Incidence in Japan, 1975–2015" International Journal of Environmental Research and Public Health 17, no. 11: 3950. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113950