A Multifactorial Evaluation of the Effects of Air Pollution and Meteorological Factors on Asthma Exacerbation

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patients and Outcome
2.3. Monitoring of Outdoor Air Pollution and Climate Factors
2.4. Statistical Analysis
3. Results
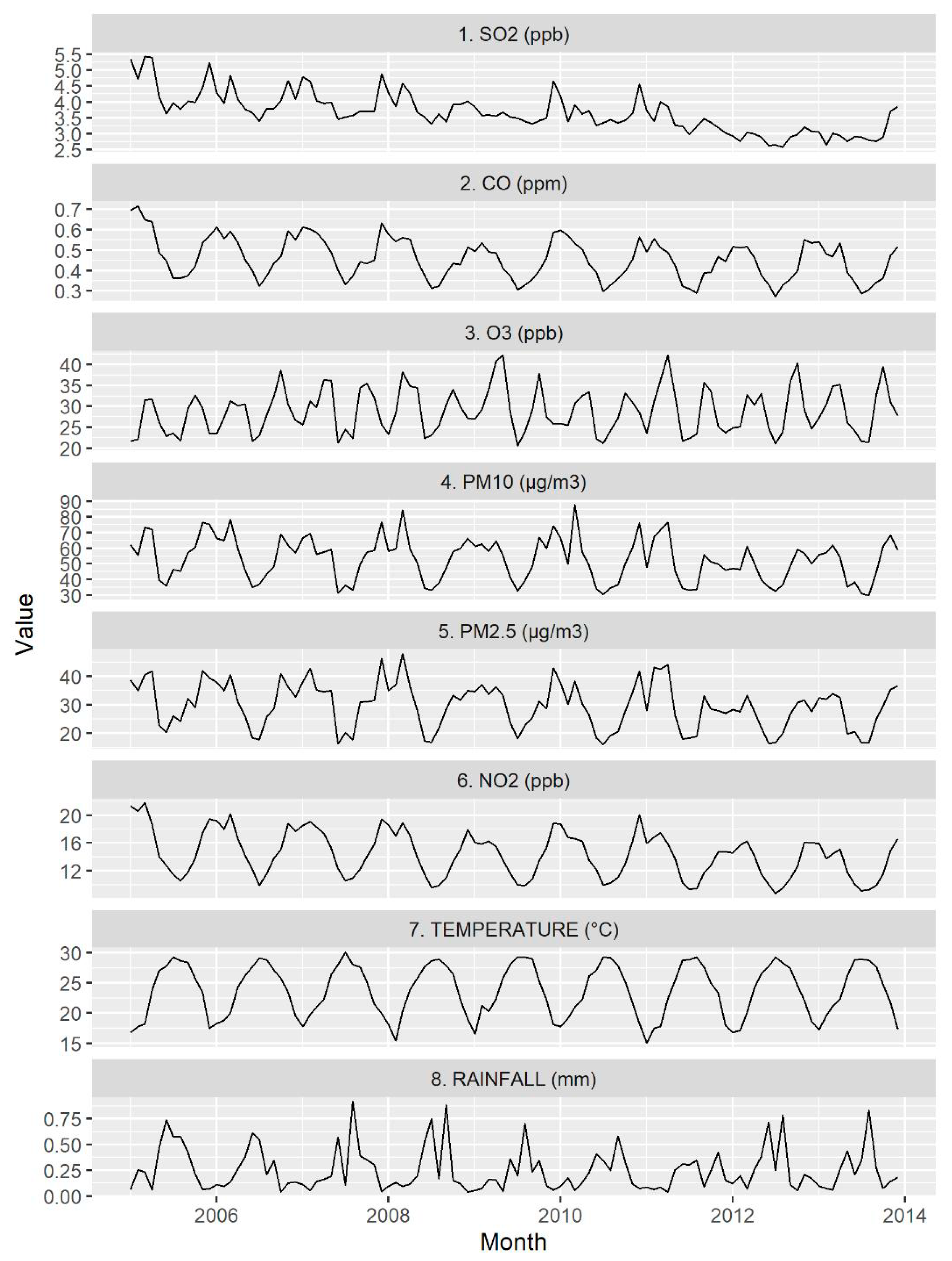
3.1. Descriptive Statistics of the Number of ER Visits, Air Pollution Levels, and Meteorological Measures
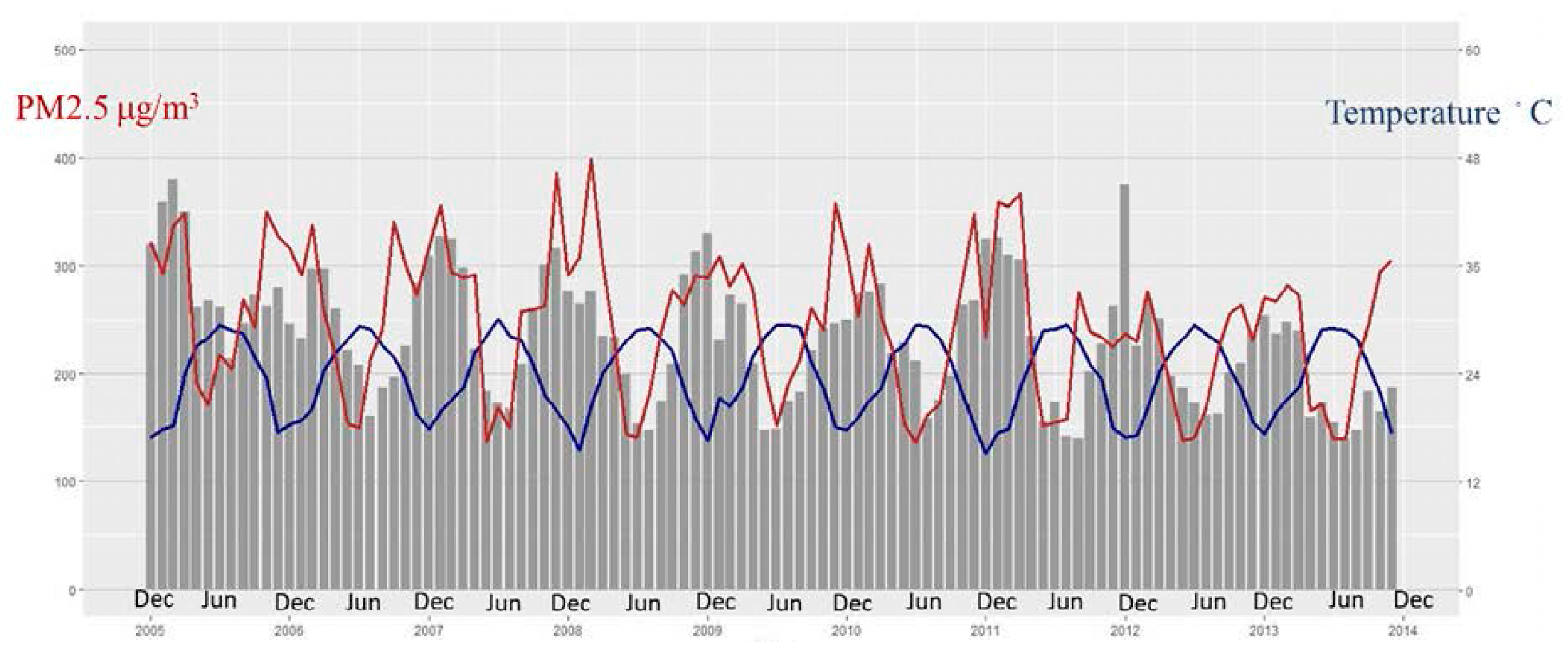
3.2. The High Correlation between the Level of Each Outdoor Air Pollutant and Meteorological Factors
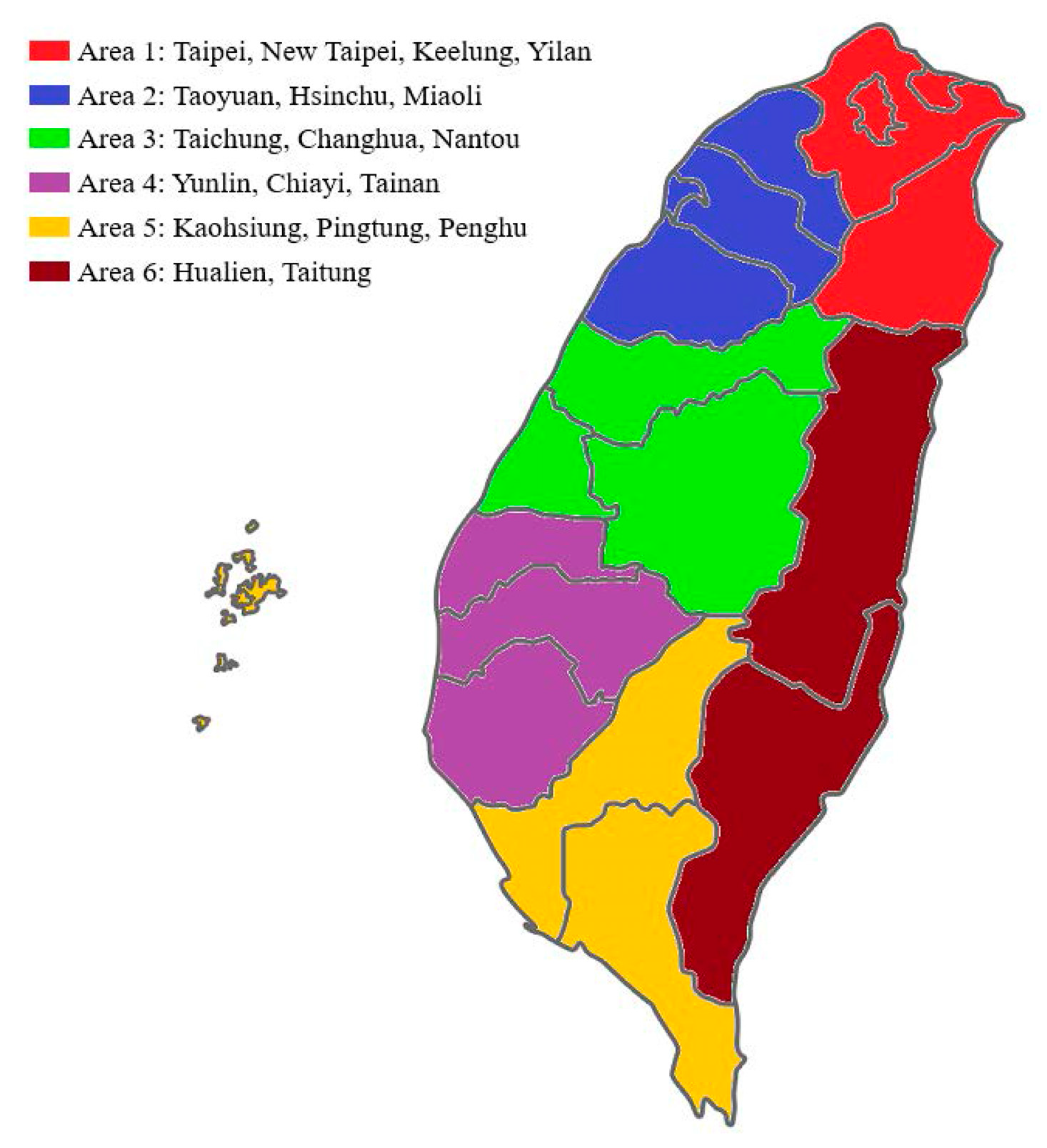
3.3. Profound Differences in Outdoor Air Pollutants among Various Geographic Areas
3.4. Relationship of Air Pollution/Meteorological Factors with ER Visits for Asthma in a Case Cross-Over Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.W.; Chow, C.M. Childhood asthma epidemiology: Insights from comparative studies of rural and urban populations. Pediatric Pulmonol. 2008, 43, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Lewis, L.M.; Mirabelli, M.C.; Beavers, S.F.; Kennedy, C.M.; Shriber, J.; Stearns, D.; Morales Gonzalez, J.J.; Santiago, M.S.; Felix, I.M.; Ruiz-Serrano, K.; et al. Characterizing environmental asthma triggers and healthcare use patterns in Puerto Rico. J. Asthma Off. J. Assoc. Care Asthma 2019, 1–12. [Google Scholar] [CrossRef]
- Perez, L.; Declercq, C.; Iniguez, C.; Aguilera, I.; Badaloni, C.; Ballester, F.; Bouland, C.; Chanel, O.; Cirarda, F.B.; Forastiere, F.; et al. Chronic burden of near-roadway traffic pollution in 10 European cities (APHEKOM network). Eur. Respir. J. 2013, 42, 594–605. [Google Scholar] [CrossRef] [Green Version]
- Munoz, X.; Barreiro, E.; Bustamante, V.; Lopez-Campos, J.L.; Gonzalez-Barcala, F.J.; Cruz, M.J. Diesel exhausts particles: Their role in increasing the incidence of asthma. Reviewing the evidence of a causal link. Sci. Total Environ. 2019, 652, 1129–1138. [Google Scholar] [CrossRef]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Delfino, R.J.; Zeiger, R.S.; Seltzer, J.M.; Street, D.H.; Matteucci, R.M.; Anderson, P.R.; Koutrakis, P. The effect of outdoor fungal spore concentrations on daily asthma severity. Environ. Health Perspect. 1997, 105, 622–635. [Google Scholar] [CrossRef]
- Ostro, B.; Lipsett, M.; Mann, J.; Braxton-Owens, H.; White, M. Air pollution and exacerbation of asthma in African-American children in Los Angeles. Epidemiology 2001, 12, 200–208. [Google Scholar] [CrossRef]
- McConnell, R.; Islam, T.; Shankardass, K.; Jerrett, M.; Lurmann, F.; Gilliland, F.; Gauderman, J.; Avol, E.; Kunzli, N.; Yao, L.; et al. Childhood incident asthma and traffic-related air pollution at home and school. Environ. Health Perspect. 2010, 118, 1021–1026. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, M.L.; Dhingra, R.; Burbank, A.J.; Todorich, K.; Loughlin, C.E.; Frye, M.; Duncan, K.; Robinette, C.; Mills, K.; Devlin, R.B.; et al. Low-level ozone has both respiratory & systemic effects in African-American adolescents with asthma despite asthma controller therapy. J. Allergy Clin. Immunol. 2018, 142, 1974–1977.e3. [Google Scholar]
- Dai, Y.; Qiu, H.; Sun, S.; Yang, Y.; Lin, H.; Tian, L. Age-dependent effect of ambient ozone on emergency asthma hospitalizations in Hong Kong. J. Allergy Clin. Immunol. 2018, 141, 1532–1534 e5. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, Y.; Lee, M.R.; Kim, J.; Jung, A.; Park, J.S.; Jang, A.S.; Park, S.W.; Uh, S.T.; Choi, J.S.; et al. Winter season temperature drops and sulfur dioxide levels affect on exacerbation of refractory asthma in South Korea: A time-trend controlled case-crossover study using soonchunhyang asthma cohort data. J. Asthma Off. J. Assoc. Care Asthma 2012, 49, 679–687. [Google Scholar] [CrossRef]
- Witten, A.; Solomon, C.; Abbritti, E.; Arjomandi, M.; Zhai, W.; Kleinman, M.; Balmes, J. Effects of nitrogen dioxide on allergic airway responses in subjects with asthma. J. Occup. Environ. Med. 2005, 47, 1250–1259. [Google Scholar] [CrossRef]
- Chauhan, A.J.; Inskip, H.M.; Linaker, C.H.; Smith, S.; Schreiber, J.; Johnston, S.L.; Holgate, S.T. Personal exposure to nitrogen dioxide (NO2) and the severity of virus-induced asthma in children. Lancet 2003, 361, 1939–1944. [Google Scholar] [CrossRef]
- Smith, B.J.; Nitschke, M.; Pilotto, L.S.; Ruffin, R.E.; Pisaniello, D.L.; Willson, K.J. Health effects of daily indoor nitrogen dioxide exposure in people with asthma. Eur. Respir. J. 2000, 16, 879–885. [Google Scholar] [CrossRef]
- Wang, I.J.; Tung, T.H.; Tang, C.S.; Zhao, Z.H. Allergens, air pollutants, and childhood allergic diseases. Int. J. Hyg. Environ. Health 2016, 219, 66–71. [Google Scholar] [CrossRef]
- Ma, Y.C.; Lin, C.C.; Yang, S.Y.; Chen, H.J.; Li, T.C.; Lin, J.G. Time Trend Analysis of the Prevalence and Incidence of Diagnosed Asthma and Traditional Chinese Medicine Use among Adults in Taiwan from 2000 to 2011: A Population-Based Study. PLoS ONE 2015, 10, e0140318. [Google Scholar] [CrossRef]
- Chen, B.Y.; Chen, C.H.; Chuang, Y.C.; Wu, Y.H.; Pan, S.C.; Guo, Y.L. Changes in the relationship between childhood asthma and ambient air pollution in Taiwan: Results from a nationwide survey repeated 5 years apart. Pediatric Allergy Immunol. Off. Publ. Eur. Soc. Pediatric Allergy Immunol. 2019, 30, 188–194. [Google Scholar] [CrossRef]
- Ding, P.H.; Wang, G.S.; Chen, B.Y.; Wan, G.H. Urban Air Pollution in Taiwan before and after the Installation of a Mass Rapid Transit System. J. Environ. Qual. 2016, 45, 1731–1739. [Google Scholar] [PubMed]
- Lin, S.; Luo, M.; Walker, R.J.; Liu, X.; Hwang, S.A.; Chinery, R. Extreme high temperatures and hospital admissions for respiratory and cardiovascular diseases. Epidemiology 2009, 20, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Tokuda, Y.; Ohde, S.; Ishimatsu, S.; Nakamura, T.; Birrer, R.B. The relationship of short-term air pollution and weather to ED visits for asthma in Japan. Am. J. Emerg. Med. 2009, 27, 153–159. [Google Scholar] [CrossRef]
- Ehara, A.; Takasaki, H.; Takeda, Y.; Kida, T.; Mizukami, S.; Hagisawa, M.; Yamada, Y. Are high barometric pressure, low humidity and diurnal change of temperature related to the onset of asthmatic symptoms? Pediatrics Int. Off. J. Jpn. Pediatric Soc. 2000, 42, 272–274. [Google Scholar] [CrossRef]
- Mireku, N.; Wang, Y.; Ager, J.; Reddy, R.C.; Baptist, A.P. Changes in weather and the effects on pediatric asthma exacerbations. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 2009, 103, 220–224. [Google Scholar] [CrossRef]
- Shin, S.W.; Bae, D.J.; Park, C.S.; Lee, J.U.; Kim, R.H.; Kim, S.R.; Chang, H.S.; Park, J.S. Effects of air pollution on moderate and severe asthma exacerbations. J. Asthma Off. J. Assoc. Care Asthma 2019, 1–11. [Google Scholar] [CrossRef]
- Zheng, X.Y.; Ding, H.; Jiang, L.N.; Chen, S.W.; Zheng, J.P.; Qiu, M.; Zhou, Y.X.; Chen, Q.; Guan, W.J. Association between Air Pollutants and Asthma Emergency Room Visits and Hospital Admissions in Time Series Studies: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138146. [Google Scholar] [CrossRef]
- Buka, I.; Koranteng, S.; Osornio-Vargas, A.R. The effects of air pollution on the health of children. Paediatr. Child Health 2006, 11, 513–516. [Google Scholar]
- Johnston, N.W.; Sears, M.R. Asthma exacerbations. 1: Epidemiology. Thorax 2006, 61, 722–728. [Google Scholar] [CrossRef] [Green Version]
- Cheng, T.M. Taiwan’s new national health insurance program: Genesis and experience so far. Health Aff. 2003, 22, 61–76. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.T.; Liao, C.C.; Chang, S.N.; Yang, Y.W.; Tsai, C.H.; Chen, T.L.; Sung, F.C. Increased Risk of Depression in Patients with Parkinson Disease: A Nationwide Cohort Study. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2015, 23, 934–940. [Google Scholar] [CrossRef]
- National Health Insurance Research Database. Data Subsets. Available online: https://nhird.nhri.org.tw/en/Data_Protection.html (accessed on 5 February 2019).
- Sun, H.L.; Chou, M.C.; Lue, K.H. The relationship of air pollution to ED visits for asthma differ between children and adults. Am. J. Emerg. Med. 2006, 24, 709–713. [Google Scholar] [CrossRef]
- Bates, D.V.; Baker-Anderson, M.; Sizto, R. Asthma attack periodicity: A study of hospital emergency visits in Vancouver. Environ. Res. 1990, 51, 51–70. [Google Scholar] [CrossRef]
- Navidi, W. Bidirectional case-crossover designs for exposures with time trends. Biometrics 1998, 54, 596–605. [Google Scholar] [CrossRef]
- Kan, H.; Chen, B. A case-crossover analysis of air pollution and daily mortality in Shanghai. J. Occup. Health 2003, 45, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.; Li, S.; Fan, C.; Bai, Z.; Yang, K. The impact of PM2.5 on asthma emergency department visits: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. Int. 2016, 23, 843–850. [Google Scholar] [CrossRef]
- Chang, J.C. [An introduction of "air pollution" in Taiwan]. Hu Li Za Zhi J. Nurs. 1973, 20, 24–33. [Google Scholar]
- Yu, T.Y.; Chang, I.C. Spatiotemporal features of severe air pollution in northern Taiwan. Environ. Sci. Pollut. Res. Int. 2006, 13, 268–275. [Google Scholar] [CrossRef]
- Liu, C.M.; Young, C.Y.; Lee, Y.C. Influence of Asian dust storms on air quality in Taiwan. Sci. Total Environ. 2006, 368, 884–897. [Google Scholar] [CrossRef]
- Chuang, M.T.; Lee, C.T.; Hsu, H.C. Quantifying PM2.5 from long-range transport and local pollution in Taiwan during winter monsoon: An efficient estimation method. J. Environ. Manag. 2018, 227, 10–22. [Google Scholar] [CrossRef]
- Yeh, K.W.; Chang, C.J.; Huang, J.L. The association of seasonal variations of asthma hospitalization with air pollution among children in Taiwan. Asian Pac. J. Allergy Immunol. 2011, 29, 34–41. [Google Scholar]
- Maclure, M. The case-crossover design: A method for studying transient effects on the risk of acute events. Am. J. Epidemiol. 1991, 133, 144–153. [Google Scholar] [CrossRef]
- Hwang, S.L.; Lin, Y.C.; Lin, C.M.; Hsiao, K.Y. Effects of fine particulate matter and its constituents on emergency room visits for asthma in southern Taiwan during 2008–2010: A population-based study. Environ. Sci. Pollut. Res. Int. 2017, 24, 15012–15021. [Google Scholar] [CrossRef]
- Clougherty, J.E. A growing role for gender analysis in air pollution epidemiology. Environ. Health Perspect. 2010, 118, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Barcala, F.J.; Pertega, S.; Garnelo, L.; Castro, T.P.; Sampedro, M.; Lastres, J.S.; San Jose Gonzalez, M.A.; Bamonde, L.; Valdes, L.; Carreira, J.M.; et al. Truck traffic related air pollution associated with asthma symptoms in young boys: A cross-sectional study. Public Health 2013, 127, 275–281. [Google Scholar] [CrossRef]
- Gharibi, H.; Entwistle, M.R.; Schweizer, D.; Tavallali, P.; Cisneros, R. The association between 1,3-dichloropropene and asthma emergency department visits in California, USA from 2005 to 2011: A bidirectional-symmetric case crossover study. J. Asthma Off. J. Assoc. Care Asthma 2020, 57, 601–609. [Google Scholar] [CrossRef]
- Gharibi, H.; Entwistle, M.R.; Schweizer, D.; Tavallali, P.; Thao, C.; Cisneros, R. Methyl-bromide and asthma emergency department visits in California, USA from 2005 to 2011. J. Asthma Off. J. Assoc. Care Asthma 2019, 1–10. [Google Scholar] [CrossRef]
- Orellano, P.; Quaranta, N.; Reynoso, J.; Balbi, B.; Vasquez, J. Effect of outdoor air pollution on asthma exacerbations in children and adults: Systematic review and multilevel meta-analysis. PLoS ONE 2017, 12, e0174050. [Google Scholar] [CrossRef]
- Villeneuve, P.J.; Chen, L.; Rowe, B.H.; Coates, F. Outdoor air pollution and emergency department visits for asthma among children and adults: A case-crossover study in northern Alberta, Canada. Environ. Health Glob. Access Sci. Source 2007, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, X.; Liu, W.; Cai, J.; Shen, L.; Zou, Z.; Lu, R.; Chang, J.; Wei, X.; Sun, C.; et al. Household indoor air quality and its associations with childhood asthma in Shanghai, China: On-site inspected methods and preliminary results. Environ. Res. 2016, 151, 154–167. [Google Scholar] [CrossRef]
- Senechal, H.; Visez, N.; Charpin, D.; Shahali, Y.; Peltre, G.; Biolley, J.P.; Lhuissier, F.; Couderc, R.; Yamada, O.; Malrat-Domenge, A.; et al. A Review of the Effects of Major Atmospheric Pollutants on Pollen Grains, Pollen Content, and Allergenicity. Sci. World J. 2015, 2015, 940243. [Google Scholar] [CrossRef] [Green Version]
- Tham, E.H.; Lee, A.J.; Bever, H.V. Aeroallergen sensitization and allergic disease phenotypes in Asia. Asian Pac. J. Allergy Immunol. 2016, 34, 181–189. [Google Scholar]
- Donoghue, A.M.; Thomas, M. Point source sulphur dioxide peaks and hospital presentations for asthma. Occup. Environ. Med. 1999, 56, 232–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characters | Mean ± SD | Min | 1st Qu. | Median | 3rd Qu. | Max |
|---|---|---|---|---|---|---|
| Number of ER visit (per day) | 7.7 ± 4.0 | 0 | 5 | 7 | 10 | 33 |
| Number of Hospitalization | 3.4 ± 2.1 | 0 | 2 | 3 | 5 | 14 |
| Air pollutants concentrations | ||||||
| SO2 (ppb) | 3.7 ± 1.0 | 1.5 | 3.1 | 3.6 | 4.1 | 9.8 |
| CO (ppm) | 0.5 ± 0.1 | 0.2 | 0.4 | 0.4 | 0.5 | 1.2 |
| O3 (ppb) | 28.9 ± 8.5 | 9.6 | 22.6 | 27.6 | 33.9 | 67.6 |
| PM10 (μg/m3) | 53.1 ± 22.2 | 17.9 | 36.8 | 49.2 | 65.0 | 370.7 |
| PM2.5 (μg/m3) | 29.8 ± 12.6 | 8.1 | 20.0 | 27.5 | 37.3 | 97.1 |
| NO2 (ppb) | 14.4 ± 4.1 | 3.3 | 11.0 | 14.0 | 16.9 | 33.9 |
| Meteorological measures | ||||||
| Temperature (°C) | 23.8 ± 4.7 | 10.1 | 20.0 | 24.6 | 28.0 | 31.3 |
| Rainfall (mm/day) | 0.3 ± 0.6 | 0 | 0.0 | 0.1 | 0.2 | 8.5 |
| Factors | SO2 | CO | O3 | PM10 | PM2.5 | NO2 | Temperature | Rainfall | Relative Humidity |
|---|---|---|---|---|---|---|---|---|---|
| SO2 | 1 | ||||||||
| CO | 0.6 | 1 | |||||||
| O3 | 0.1 | 0.1 | 1 | ||||||
| PM10 | 0.6 | 0.6 | 0.5 | 1 | |||||
| PM2.5 | 0.7 | 0.7 | 0.5 | 0.9 | 1 | ||||
| NO2 | 0.7 | 0.9 | 0.2 | 0.6 | 0.7 | 1 | |||
| Temperature | −0.3 | −0.6 | −0.1 | −0.4 | −0.4 | −0.7 | 1 | ||
| Rainfall | −0.3 | −0.2 | −0.2 | −0.3 | −0.3 | −0.3 | 0.2 | 1 | |
| Relative Humidity | −0.5 | −0.0 | −0.4 | −0.4 | −0.4 | −0.1 | 0.1 | 0.5 | 1 |
| Factors | OR | 95% CI | p-Value |
|---|---|---|---|
| All | |||
| SO2 | 0.954 | 0.934–0.974 | <0.001 |
| CO | 1.002 | 0.976–1.028 | 0.898 |
| O3 | 1.002 | 1.000–1.004 | 0.126 |
| PM10 | 0.999 | 0.998–1.001 | 0.235 |
| PM2.5 | 1.004 | 1.001–1.007 | 0.017 |
| NO2 | 0.999 | 0.992–1.007 | 0.788 |
| Temperature | 0.986 | 0.980–0.991 | <0.001 |
| Rainfall | 0.991 | 0.972–1.011 | 0.390 |
| Relative humidity | 0.998 | 0.996–1.001 | 0.197 |
| Factors | Male | Female | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| 0–17-year-olds | ||||||
| SO2 | 0.946 | 0.905–0.989 | 0.013 | 0.934 | 0.879–0.991 | 0.024 |
| CO | 0.987 | 0.934–1.042 | 0.628 | 0.944 | 0.875–1.019 | 0.138 |
| O3 | 1.004 | 0.999–1.009 | 0.097 | 1.007 | 1.000–1.013 | 0.041 |
| PM10 | 1.001 | 0.999–1.003 | 0.362 | 1.001 | 0.997–1.004 | 0.753 |
| PM2.5 | 0.999 | 0.994–1.005 | 0.780 | 1.004 | 0.996–1.012 | 0.343 |
| NO2 | 1.005 | 0.989–1.021 | 0.549 | 1.019 | 0.997–1.041 | 0.085 |
| Temperature | 0.982 | 0.970–0.994 | 0.003 | 0.979 | 0.963–0.995 | 0.012 |
| Rainfall | 0.963 | 0.922–1.006 | 0.089 | 0.972 | 0.914–1.034 | 0.375 |
| Relative humidity | 1.002 | 0.997–1.008 | 0.437 | 0.999 | 0.992–1.007 | 0.860 |
| 18–64-year-olds | ||||||
| SO2 | 0.963 | 0.915–1.012 | 0.139 | 0.968 | 0.923–1.016 | 0.191 |
| CO | 1.027 | 0.967–1.092 | 0.384 | 1.035 | 0.976–1.098 | 0.252 |
| O3 | 1.001 | 0.996–1.006 | 0.656 | 1.001 | 0.996–1.006 | 0.713 |
| PM10 | 0.999 | 0.995–1.002 | 0.418 | 0.998 | 0.994–1.002 | 0.281 |
| PM2.5 | 1.004 | 0.997–1.011 | 0.254 | 1.003 | 0.996–1.010 | 0.401 |
| NO2 | 0.987 | 0.969–1.004 | 0.140 | 0.99 | 0.974–1.007 | 0.267 |
| Temperature | 0.984 | 0.970–0.998 | 0.021 | 0.986 | 0.973–0.999 | 0.032 |
| Rainfall | 1.019 | 0.978–1.062 | 0.372 | 1.028 | 0.984–1.073 | 0.221 |
| Relative humidity | 0.999 | 0.993–1.005 | 0.757 | 0.996 | 0.990–1.002 | 0.149 |
| Factors | Male | Female | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| 6–11-year-olds | ||||||
| SO2 | 0.929 | 0.857–1.008 | 0.076 | 0.952 | 0.843–1.076 | 0.432 |
| CO | 0.989 | 0.892–1.096 | 0.833 | 0.873 | 0.739–1.031 | 0.109 |
| O3 | 1.007 | 0.998–1.017 | 0.110 | 1.014 | 1.000–1.029 | 0.056 |
| PM10 | 1.004 | 1.000–1.009 | 0.077 | 1.001 | 0.992–1.010 | 0.823 |
| PM2.5 | 0.997 | 0.986–1.007 | 0.541 | 0.995 | 0.977–1.014 | 0.591 |
| NO2 | 1.012 | 0.983–1.042 | 0.421 | 1.054 | 1.007–1.102 | 0.023 |
| Temperature | 0.972 | 0.949–0.995 | 0.018 | 0.969 | 0.934–1.005 | 0.086 |
| Rainfall | 0.897 | 0.816–0.986 | 0.025 | 1.019 | 0.887–1.171 | 0.790 |
| Relative humidity | 1.009 | 0.998–1.021 | 0.106 | 0.995 | 0.978–1.012 | 0.559 |
| 12–17-year-olds | ||||||
| SO2 | 0.983 | 0.854–1.131 | 0.806 | 0.831 | 0.691–0.999 | 0.049 |
| CO | 0.858 | 0.725–1.017 | 0.077 | 0.876 | 0.697–1.101 | 0.256 |
| O3 | 1.011 | 0.997–1.005 | 0.123 | 0.997 | 0.978–1.015 | 0.719 |
| PM10 | 0.998 | 0.990–0.123 | 0.550 | 1.004 | 0.997–1.012 | 0.270 |
| PM2.5 | 1.006 | 0.988–1.024 | 0.531 | 1.006 | 0.982–1.030 | 0.624 |
| NO2 | 1.030 | 0.983–1.080 | 0.215 | 1.049 | 0.983–1.120 | 0.145 |
| Temperature | 0.981 | 0.945–1.019 | 0.322 | 0.992 | 0.943–1.044 | 0.769 |
| Rainfall | 0.961 | 0.836–1.104 | 0.571 | 1.088 | 0.940–1.258 | 0.258 |
| Relative humidity | 1.007 | 0.990–1.0.24 | 0.432 | 1.000 | 0.979–1.022 | 0.997 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.-R.; Lin, C.-H.R.; Tsai, J.-H.; Hsieh, Y.-T.; Tsai, T.-A.; Tsai, C.-K.; Lee, Y.-C.; Liu, T.-Y.; Tsai, C.-M.; Chen, C.-C.; et al. A Multifactorial Evaluation of the Effects of Air Pollution and Meteorological Factors on Asthma Exacerbation. Int. J. Environ. Res. Public Health 2020, 17, 4010. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114010
Yu H-R, Lin C-HR, Tsai J-H, Hsieh Y-T, Tsai T-A, Tsai C-K, Lee Y-C, Liu T-Y, Tsai C-M, Chen C-C, et al. A Multifactorial Evaluation of the Effects of Air Pollution and Meteorological Factors on Asthma Exacerbation. International Journal of Environmental Research and Public Health. 2020; 17(11):4010. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114010
Chicago/Turabian StyleYu, Hong-Ren, Chun-Hung Richard Lin, Jui-Hsiu Tsai, Yun-Ting Hsieh, Ti-An Tsai, Chang-Ku Tsai, Yi-Chen Lee, Ta-Yu Liu, Chih-Min Tsai, Chih-Cheng Chen, and et al. 2020. "A Multifactorial Evaluation of the Effects of Air Pollution and Meteorological Factors on Asthma Exacerbation" International Journal of Environmental Research and Public Health 17, no. 11: 4010. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114010