An Exploration of the Effectiveness of a Peer-Led Pain Management Program (PAP) for Nursing Home Residents with Chronic Pain and an Evaluation of Their Experiences: A Pilot Randomized Controlled Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methodology
2.1. Study Design
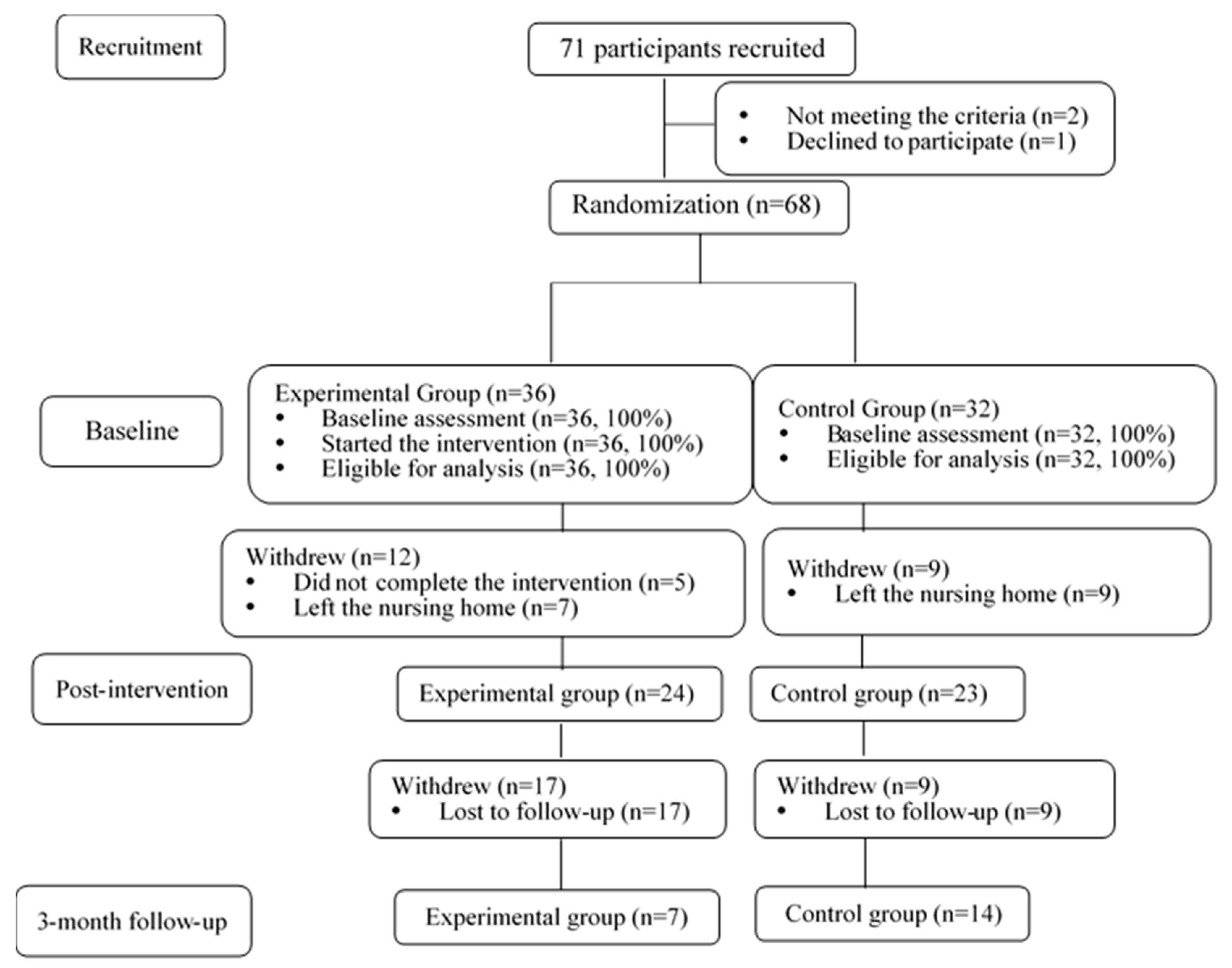
2.2. Sample and Procedure
2.2.1. PVs
- (1)
- Aged > 55 years;
- (2)
- Scored > 6 in the Abbreviated Mental Test, indicating that they had the mental/cognitive capacity to serve as elderly peer volunteers;
- (3)
- Be willing to attend training workshops and biweekly meetings with the research team for case reviews, discussions, and to reinforce strategies on pain management education;
- (4)
- Pass an exit test (including a knowledge test on pain management) showing their ability to demonstrate various non-pharmacological practices and use the teaching manual (the principal investigator and one of the co-investigators were the assessors, and supplementary classes were given to those PVs who did not pass the exit test);
- (5)
- Be willing to lead the PAP in a nursing home.
2.2.2. Older Adults
3. Experimental Group vs. Control Group
3.1. Experimental Group
3.2. Control Group
4. Outcome Measures
4.1. Primary Outcome
Pain Self-Efficacy
4.2. Secondary Outcomes
4.2.1. Pain Intensity and Pain Interference
4.2.2. Depression
4.2.3. Pain Knowledge
4.2.4. Satisfaction and Acceptance
5. Statistical Analysis
6. Results
6.1. Demographic Characteristics
6.2. Pain Self-Efficacy, Pain Intensity and Pain Interference
6.3. Depression
6.4. Pain Knowledge
6.5. Satisfaction and Acceptance
6.5.1. Feedback and Comments from PVs
6.5.2. Feedback and Comments from the Older Adults
7. Discussion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Patel, K.V.; Guralnik, J.M.; Dansie, E.J.; Turk, D.C. Prevalence and impact of pain among older adults in the United States: Findings from the 2011 National Health and Aging Trends Study. Pain 2013, 154, 2649–2657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulla, A.; Adams, N.; Bone, M.; Elliott, A.M.; Gaffin, J.; Jones, D.; Knaggs, R.; Martin, D.; Sampson, L.; Schofield, P. Guidance on the management of pain in older people. Age Ageing 2013. [Google Scholar] [CrossRef] [Green Version]
- Kaye, A.D.; Baluch, A.; Scott, J.T. Pain management in the elderly population: A review. Ochsner J. 2010. [Google Scholar]
- Thielke, S.; Sale, J.; Reid, M.C. Aging: Are these 4 pain myths complicating care? J. Fam. Pract. 2012. [Google Scholar]
- Tse, M.M.Y.; Sin Vong, S.K.; Ho, S.S.K. The effectiveness of an integrated pain management program for older persons and staff in nursing homes. Arch. Gerontol. Geriatr. 2012. [Google Scholar] [CrossRef] [PubMed]
- Kawi, J. Self-management and support in chronic pain subgroups: Integrative review. J. Nurse Pract. 2013. [Google Scholar] [CrossRef]
- Cooper, K.; Wilcock, S. The effectiveness of peer support interventions for community-dwelling adults with chronic non-cancer pain: a systematic review protocol. JBI Database Syst. Rev. Implement. Reports 2013. [Google Scholar] [CrossRef]
- Tse, M.M.Y.; Yeung, S.S.Y.; Lee, P.H.; Ng, S.S.M. Effects of a peer-led pain management program for nursing home residents with chronic pain: A pilot study. Pain Med. (United States) 2016. [Google Scholar] [CrossRef] [Green Version]
- Tse, M.M.Y.; Ng, S.S.M.; Bai, X.; Lee, P.H.; Lo, R.; Cheung, D.S.K.; Cheung, K.; Yeung, S.S.Y. Lesson learned from peer volunteers in a peer-led pain management program among nursing home residents. Int. J. Environ. Res. Public Health 2019, 16, 3097. [Google Scholar] [CrossRef] [Green Version]
- Cooper, K.; Schofield, P.; Smith, B.H.; Klein, S. PALS: peer support for community dwelling older people with chronic low back pain: a feasibility and acceptability study. Physiotherapy 2020. [Google Scholar] [CrossRef] [Green Version]
- Cooper, K.; Schofield, P.; Klein, S.; Smith, B.H.; Jehu, L.M. Exploring peer-mentoring for community dwelling older adults with chronic low back pain: a qualitative study. Physiotherapy 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ersek Mary, A.; Turner Judith, M.; Mccurry Susan, M.; Gibbons Laura, M.; Kraybill Beth, M. Efficacy of a Self-Management Group Intervention for Elderly Persons With Chronic Pain. Clin. J. Pain 2003, 19, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Chen, P.P.; Wong, T.C.M.; Gin, T.; Wong, E.; Chan, I.S.F.; Chu, J. Validation of the Chinese version of pain self-efficacy questionnaire. Anesth. Analg. 2007, 104, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Wang Xin, S.; Mendoza Tito, R.; Gao Shuo-Zheng, S.; Cleeland Charles, S. The chinese version of the brief pain inventory (BPI-C): its development and use in a study of cancer pain. Pain 1996, 67, 407–416. [Google Scholar] [CrossRef]
- Boey, K.W.; Chiu, H.F.K. Assessing psychological well-being of the old-old: A comparative study of GDS-15 and GHQ-12. Clin. Gerontol. 1998. [Google Scholar] [CrossRef]
- Wegener, S.T.; Mackenzie, E.J.; Ephraim, P.; Ehde, D.; Williams, R. Self-Management Improves Outcomes in Persons With Limb Loss. Arch. Phys. Med. Rehabil. 2009, 90, 373–380. [Google Scholar] [CrossRef]
- Dear, B.F.; Gandy, M.; Karin, E.; Ricciardi, T.; Fogliati, V.J.; McDonald, S.; Staples, L.G.; Perry, K.N.; Sharpe, L.; Nicholas, M.K.; et al. The pain course: A randomised controlled trial comparing a remote-delivered chronic pain management program when provided in online and workbook formats. Pain 2017. [Google Scholar] [CrossRef]
- Chou, K.L.; Chi, I. Prevalence and correlates of depression in Chinese oldest-old. Int. J. Geriatr. Psychiatry 2005. [Google Scholar] [CrossRef]
- Yang, Y. How does functional disability affect depressive symptoms in late life? The role of perceived social support and psychological resources. J. Health Soc. Behav. 2006. [Google Scholar] [CrossRef]
- Zivin, K.; Llewellyn, D.J.; Lang, I.A.; Vijan, S.; Kabeto, M.U.; Miller, E.M.; Langa, K.M. Depression among older adults in the United States and England. Am. J. Geriatr. Psychiatry 2010. [Google Scholar] [CrossRef] [Green Version]
- Census and Statistics DepartmentSocio-demographic Profile, Health Status and Self-care Capability of Older Persons. Available online: https://www.statistics.gov.hk/pub/B11302402009XXXXB0100.pdf (accessed on 17 April 2020).
- Chou, K.L.; Chi, I. Reciprocal relationship between social support and depressive symptoms among Chinese elderly. Aging Ment. Heal. 2003. [Google Scholar] [CrossRef] [PubMed]
- Greenglass, E.; Fiksenbaum, L.; Eaton, J. The relationship between coping, social support, functional disability and depression in the elderly. Anxiety Stress Coping 2006. [Google Scholar] [CrossRef]
- Yeung, D.Y.; Fung, H.H.; Lang, F.R. Gender differences in social network characteristics and psychological well-being among Hong Kong Chinese: The role of future time perspective and adherence to Renqing. Aging Ment. Heal. 2007. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total (N = 68) (N, %) | Experimental Group (n = 36) (n, %) | Control Group (n = 32) (n, %) | p-Value * |
|---|---|---|---|---|
| Gender | 0.771 | |||
| Female | 50 (73.5) | 27 (75.0) | 23 (71.9) | |
| Male | 18 (26.5) | 9 (25.0) | 9 (28.1) | |
| Age group (years) | 0.649 | |||
| 60–70 | 3 (4.4) | 1 (2.8) | 2 (6.2) | |
| 71–80 | 15 (22.1) | 6 (16.7) | 9 (28.1) | |
| 81–90 | 33 (48.5) | 19 (52.8) | 14 (43.8) | |
| 91–100 | 16 (23.5) | 9 (25.0) | 7 (21.9) | |
| Marital status | 0.293 | |||
| Single | 1 (1.5) | 1 (2.8) | 0 | |
| Married | 18 (26.5) | 8 (22.2) | 10 (31.3) | |
| Divorced | 2 (2.9) | 0 | 2 (6.3) | |
| Widowed | 45 (66.2) | 25 (69.4) | 20 (62.5) | |
| Education level | 0.939 | |||
| Uneducated | 25 (36.8) | 13 (36.1) | 13 (40.6) | |
| Primary school | 26 (38.2) | 13 (36.1) | 13 (40.6) | |
| Secondary school | 15 (22.1) | 9 (25.0) | 6 (18.8) | |
| University or above | 1 (2.9) | 1 (2.8) | 1 (3.) | |
| Occupation | 0.807 | |||
| Physical laborer | 27 (39.7) | 15 (41.7) | 12 (37.5) | |
| Technical job | 15 (22.1) | 9 (25.0) | 6 (18.8) | |
| Clerk | 10 (14.7) | 6 (16.7) | 4 (12.6) | |
| Housewife | 8 (11.8) | 3 (8.3) | 5(15.6) | |
| Others | 7 (10.3) | 3 (8.3) | 4(12.6) | |
| Length of institutionalization | 0.531 | |||
| <1 year | 15 (22.1) | 8 (22.2) | 7 (21.9) | |
| 1–3 years | 28 (41.2) | 13 (36.1) | 15 (37.5) | |
| 4–5 years | 7 (10.3) | 2 (5.6) | 5 (15.6) | |
| 6–10 years | 6 (8.8) | 4 (11.1) | 2 (6.3) | |
| >10 years | 4 (5.9) | 3 (8.3) | 1 (3.1) | |
| Chronic diseases | ||||
| Heart disease | 9 (13.4) | 4 (11.1) | 5 (15.6) | 0.648 |
| Diabetes | 22 (32.4) | 10 (27.8) | 12 (37.5) | 0.486 |
| Hypertension | 27 (39.7) | 13 (36.1) | 14 (43.8) | 0.649 |
| Tracheal disease | 2 (2.9) | 0 | 2 (6.3) | 0.139 |
| Cataract | 16 (23.5) | 8 (22.2) | 8 (25.0) | 0.889 |
| Stroke | 7 (10.3) | 5 (13.9) | 2 (6.3) | 0.265 |
| Parkinson disease | 1 (1.5) | 0 | 1 (3.1) | 0.299 |
| Arthritis | 8 (11.8) | 2 (5.6) | 6 (18.8) | 0.109 |
| Physical disability | 1 (1.5) | 0 | 1 (3.1) | 0.299 |
| Other chronic disease | 5 (7.6) | 3 (8.3) | 2 (6.3) | 0.693 |
| Group | Experimental Group | Control Group | Between Group p-Value * | Cohen’s d^ (95% CI) | |
|---|---|---|---|---|---|
| Time Point | |||||
| Pain self-efficacy | |||||
| T0 | 37.56 ± 13.38 | 39.67 ± 12.78 | 0.502 | −0.16(−8.26–4.04) | |
| T1 | 41.60 ± 11.55 a1 | 40.33 ± 12.10 b1 | 0.674 | 0.11(−4.64–7.19) | |
| T2 | 46.56 ± 10.81 a2 | 38.77 ± 5.27 b2 | 0.040 | 0.92(0.37–15.22) | |
| Pain intensity | |||||
| T0 | 5.69 ± 3.01 | 5.63 ± 2.39 | 0.914 | 0.02(−1.33–1.19) | |
| T1 | 5.08 ± 3.13 a3 | 5.43 ± 2.47 b3 | 0.738 | −0.12(−1.27–1.79) | |
| T2 | 5.00 ± 2.83 a4 | 5.36 ± 3.46 b4 | 0.471 | −0.11(−3.39–1.57) | |
| Pain interference | |||||
| T0 | 2.63 ± 2.46 | 2.75 ± 2.07 | 0.819 | −0.05(−1.18–0.94) | |
| T1 | 2.11 ± 2.23 a5 | 2.48 ± 1.99 b5 | 0.710 | −0.18(−1.32–0.90) | |
| T2 | 2.16 ± 1.68 a6 | 2.69 ± 2.68 b6 | 0.731 | −0.24(−1.44–2.05) | |
| Group | Experimental Group | Control Group | Between Group p-Value * | Cohen’s d^ (95% CI) | |
|---|---|---|---|---|---|
| Time Point | |||||
| Geriatric Depression Scale | |||||
| T0 | 4.36 ± 3.10 | 4.44 ± 2.75 | 0.913 | −0.027(−1.28–1.45) | |
| T1 | 3.50 ± 2.30 a7 | 4.04 ± 3.27 b7 | 0.704 | −0.191(−1.18–1.74) | |
| T2 | 3.86 ± 1.68 a8 | 4.21 ± 2.46 b8 | 0.848 | −0.166(−1.43–1.74) | |
| Group | Experimental Group | Control Group | Between Group p-Value * | Cohen’s d^ (95% CI) | |
|---|---|---|---|---|---|
| Time Point | |||||
| Pain knowledge | |||||
| T0 | 45.45 ± 19.59 | 44.95 ± 20.61 | 0.916 | 0.02(−8.19–9.92) | |
| T1 | 53.41 ± 21.33 a9 | 51.38 ± 16.13 b9 | 0.538 | 0.11(−13.64–7.12) | |
| T2 | 59.74 ± 19.44 a10 | 55.84 ± 21.91 b10 | 0.865 | 0.19(−16.65–19.82) | |
| Categories | Feedback and Comments from Older Adults |
|---|---|
| About the program | I like this program. |
| I feel happy and relaxed when taking part in the program every week. | |
| Some of the contents are really helpful, e.g., exercise. | |
| I like the massage part most, because I cannot do it by myself. | |
| The various activities in the program make it interesting. | |
| Some of the contents are difficult to memorize. | |
| About the peer volunteers (Experimental group only) | The volunteers are very patient and nice. |
| I like the volunteers. | |
| I hope the volunteers can come and visit us more often. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tse, M.; Li, Y.; Tang, S.K.; Ng, S.S.M.; Bai, X.; Lee, P.H.; Lo, R.; Yeung, S.S.Y. An Exploration of the Effectiveness of a Peer-Led Pain Management Program (PAP) for Nursing Home Residents with Chronic Pain and an Evaluation of Their Experiences: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 4090. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114090
Tse M, Li Y, Tang SK, Ng SSM, Bai X, Lee PH, Lo R, Yeung SSY. An Exploration of the Effectiveness of a Peer-Led Pain Management Program (PAP) for Nursing Home Residents with Chronic Pain and an Evaluation of Their Experiences: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(11):4090. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114090
Chicago/Turabian StyleTse, Mimi, Yajie Li, Shuk Kwan Tang, Shamay S. M. Ng, Xue Bai, Paul H. Lee, Raymond Lo, and Suey Shuk Yu Yeung. 2020. "An Exploration of the Effectiveness of a Peer-Led Pain Management Program (PAP) for Nursing Home Residents with Chronic Pain and an Evaluation of Their Experiences: A Pilot Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 11: 4090. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114090