Caregiver Burden Domains and Their Relationship with Anxiety and Depression in the First Six Months of Cancer Diagnosis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
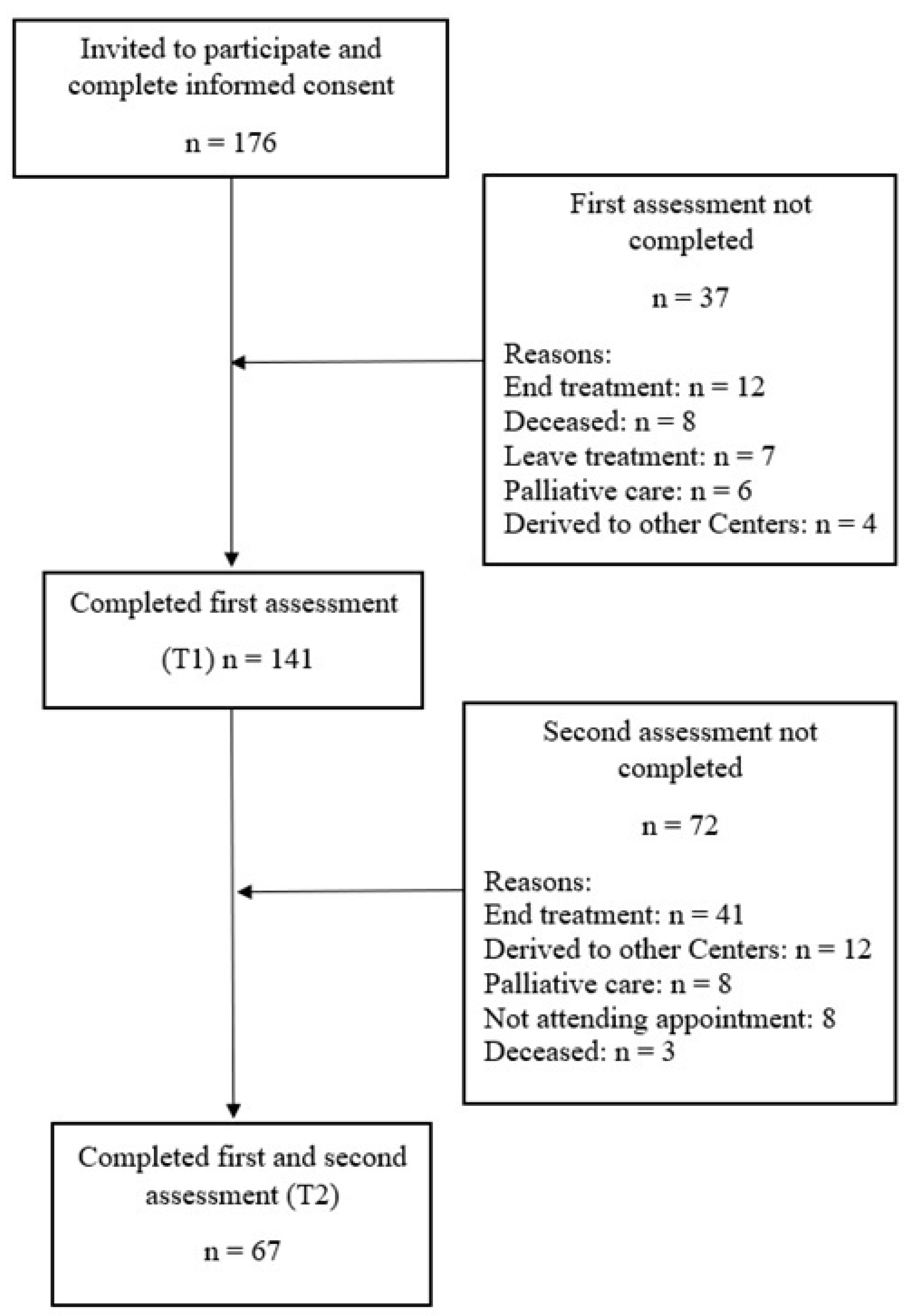
2.1. Participants
2.2. Variables and Instruments
2.3. Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sociedad Española de Oncología Médica. Las cifras del cáncer en España. 2019. Available online: https://seom.org/dmcancer/wp-content/uploads/2019/Informe-SEOM-cifras-cancer-2019.pdf (accessed on 1 October 2019).
- Biegel, D.E.; Schulz, R. Family Caregiving in Chronic Illness: Alzheimer’s Disease, Cancer, Heart Disease, Mental Illness, and Stroke; Sage Publications: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Hagedoorn, M.; Sanderman, R.; Bolks, H.N.; Tuinstra, J.; Coyne, J.C. Distress in couples coping with cancer: A meta-analysis and critical review of role and gender effects. Psychol. Bull. 2008, 134, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Sherwood, P.R.; Given, B.A.; Donovan, H.; Baum, A.; Given, C.W.; Bender, C.M.; Schulz, R. Guiding research in family care: A new approach to oncology caregiving. Psychooncology 2008, 17, 986–996. [Google Scholar] [CrossRef]
- Kim, Y.; Schulz, R. Family caregivers’ strains: Comparative analysis of cancer caregiving with dementia, diabetes, and frail elderly caregiving. J. Aging Health 2008, 20, 483–503. [Google Scholar] [CrossRef]
- Andersen, N.I.; Nielsen, C.I.; Danbjørg, D.B.; Møller, P.K.; Brochstedt, K.D. Caregivers’ Need for Support in an Outpatient Cancer Setting. Oncol. Nurs. Forum 2019, 46, 757–767. [Google Scholar] [CrossRef]
- Lee, Y.H.; Liao, Y.C.; Shun, S.C.; Lin, K.C.; Liao, W.Y.; Chang, P.H.; Jhang, S.Y.; Yu, C.J.; Yang, P.C.; Hsieh, P.Y.; et al. Trajectories of caregivers burden and related factors in family caregivers of patients with lung cancer. Psychooncology 2018, 27, 1493–1500. [Google Scholar] [CrossRef]
- Girgis, A.; Lambert, S. Cost of informal caregiving in cancer care. Cancer Forum 2017, 41, 16–22. [Google Scholar]
- Goren, A.; Gilloteau, I.; Lees, M.; DaCosta Dibonaventura, M. Quantifying the burden of informal caregiving for patients with cancer in Europe. Support. Care Cancer 2014, 22, 1637–1646. [Google Scholar] [CrossRef]
- Johansen, S.; Cvancarova, M.; Ruland, C. The effect of cancer patients´ and their family caregivers´ physical and emotional symptoms on caregiver burden. Cancer Nurs. 2018, 41, 91–99. [Google Scholar] [CrossRef]
- Lambert, S.D.; Girgis, A.; Lecathelinais, C.; Stacey, F. Walking a mile in their shoes: Anxiety and depression among partners and caregivers of cancer survivors at 6 and 12 months post diagnosis. Support. Care Cancer 2013, 21, 75–85. [Google Scholar] [CrossRef]
- Saria, M.G.; Courchesne, N.S.; Evangelista, L.; Carter, J.L.; MacManus, D.A.; Gorman, M.K.; Nyamathi, A.M.; Phillips, L.R.; Piccioni, D.E.; Kesari, S.; et al. Anxiety and depression Associated with burden in caregivers of patients with brain metastases. Oncol. Nurs. Forum 2017, 44, 306–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, H.M.; Chuang, D.M.; Yang, F.; Yang, Y.; Liu, W.M.; Liu, L.H.; Tian, H.M. Prevalence and determinants of depression in caregivers of cancer patients: A systematic review and meta-analysis. Medicine (Baltimore) 2018, 97, e11863. [Google Scholar] [CrossRef]
- Park, B.; Kim, S.Y.; Shin, J.Y.; Sanson-Fisher, R.W.; Shin, D.W.; Cho, J.; Park, J.H. Prevalence and predictors of anxiety and depression among family caregivers of cancer patients: A nationwide survey of patient-family caregiver dyads in Korea. Support. Care Cancer 2013, 21, 2799–2807. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.Y.; Molassiotis, A.; Lloyd-Williams, M.; Yorke, J. Burden, emotional distress and quality of life among informal caregivers of lung cancer patients: An exploratory study. Eur. J. Cancer Care 2018, 27, e12691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reblin, M.; Small, B.; Jim, H.; Weimer, J.; Sherwood, P. Mediating burden and stress over time: Caregivers of patients with primary brain tumor. Psychooncology 2018, 27, 607–612. [Google Scholar] [CrossRef]
- Karabekiroğlu, A.; Demir, E.Y.; Aker, S.; Kocamanoğlu, B.; Karabulut, G.S. Predictors of depression and anxiety among caregivers of hospitalised advanced cancer patients. Singap. Med. J. 2018, 59, 572–577. [Google Scholar] [CrossRef] [Green Version]
- Hyde, M.K.; Legg, M.; Occhipinti, S.; Lepore, S.J.; Ugalde, A.; Zajdlewicz, L.; Laurie, K.; Dunn, J.; Chambers, S.K. Predictors of long-term distress in female partners of men diagnosed with prostate cancer. Psychooncology 2018, 27, 946–954. [Google Scholar] [CrossRef]
- Milbury, K.; Badr, H.; Fossella, F.; Pisters, K.M.; Carmack, C.L. Longitudinal associations between caregiver burden and patient and spouse distress in couples coping with lung cancer. Support. Care Cancer 2013, 21, 2371–2379. [Google Scholar] [CrossRef] [Green Version]
- Family Caregiver Alliance. Caregiver Statistics: Demographics; Family Caregiver Alliance: San Francisco, CA, USA, 2016. [Google Scholar]
- Whitlatch, C.J.; Zarit, S.H.; Von Eye, A. Efficacy of interventions with caregivers: A reanalysis. Gerontologist 1991, 31, 9–14. [Google Scholar] [CrossRef]
- Martín, M.; Salvadó, I.; Nadal, S.; Miji, L.C.; Rico, J.M.; Lanz, P.; Taussig, M.I. Adaptación para nuestro medio de la Escala de Sobrecarga del Cuidador (Caregiver Burden Interview) de Zarit. Rev. Gerontol. 1996, 6, 338–346. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the psychometric characteristics of the Spanish version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [PubMed] [Green Version]
- Ge, L.; Mordiffi, S.Z. Factors associated with higher caregivers burden among family caregivers of elderly cancer patients: A systematic review. Cancer Nurs. 2017, 40, 471–478. [Google Scholar] [CrossRef]
- Friðriksdóttir, N.; Saevarsdóttir, T.; Halfdánardóttir, S.Í.; Jónsdóttir, A.; Magnúsdóttir, H.; Olafsdóttir, K.L.; Guðmundsdóttir, G.; Gunnarsdóttir, S. Family members of cancer patients: Needs, quality of life and symptoms of anxiety and depression. Acta Oncol. 2011, 50, 252–258. [Google Scholar] [CrossRef]
- Große, J.; Treml, J.; Kersting, A. Impact of caregiver burden on mental health in bereaved caregivers of cancer patients: A systematic review. Psychooncology 2018, 27, 757–767. [Google Scholar] [CrossRef]
- DuBenske, L.L.; Gustafson, D.H.; Namkoong, K.; Hawkins, R.P.; Atwood, A.K.; Brown, R.L.; Chih, M.Y.; McTavish, F.; Carmack, C.L.; Buss, M.K.; et al. CHESS improves cancer caregivers´burden and mood: Results of an eHealth RCT. Health Psychol. 2014, 33, 1261–1272. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Caregivers | Patients | |
|---|---|---|
| Sex | ||
| Female | 44 (65.7%) | 38(56.7%) |
| Male | 23 (34.3%) | 29 (43.3%) |
| Age M (SD) | 51.63 (13.25) | 58.60 (15.28) |
| Education | ||
| Basic | 35.8% | 41.8% |
| Vocational | 26.9% | 23.9% |
| Secondary | 14.9% | 13.4% |
| Collegue | 22.4% | 20.9% |
| Employment status | ||
| Full time job | 32.8% | 23.4% |
| Own business | 16.4% | 9.4% |
| Seasonal work | 20.9% | 17.2% |
| Unemployment | 19.4% | 17.2% |
| Rent | 1.5% | 4.7% |
| Retirement | 9% | 28.1% |
| Relation with patient | ||
| Partner | 58.2% | |
| Father/Mother | 3% | |
| Son/Daughter | 28.4% | |
| Brother/Sister | 7.5% | |
| Friend | 3% | |
| Cancer type | ||
| Head and neck | 10.8% | |
| Lung | 6.2% | |
| Breast | 21.5% | |
| Gastrointestinal | 49.2% | |
| Uterine/Ovarian | 3.1% | |
| Genitourinary | 6.2% | |
| Conective tissue/Skin | 3.1% | |
| Cancer stage | ||
| I | 17.9% | |
| II | 23.9% | |
| II | 17.9% | |
| IV | 40.3% | |
| Treatment type | ||
| Surgery | 12.1% | |
| Chemotherapy | 18.2% | |
| Radiotherapy | 1.5% | |
| Hormonal | 1.5% | |
| Surgery + Chemotherapy | 42.4% | |
| Surgery + Radiotherapy | 1.5% | |
| Surgery + Chemotherapy + Radiotherapy | 22.7% |
| ZBI Domains (Max Poss. Score) | T1 M(SD) | T2 M(SD) | t | p |
|---|---|---|---|---|
| Total burden (88) | 42.66 (12.77) | 41.16 (12.06) | 1.41 | 0.16 |
| Burden in the relationship (24) | 12.72 (4.09) | 12.15 (3.08) | 1.75 | 0.08 |
| Emotional burden (28) | 11.94 (3.97) | 11.73 (3.52) | 0.54 | 0.58 |
| Social and family life burden (16) | 7.67 (3.31) | 7.37 (2.93) | 1.19 | 0.23 |
| Financial burden (4) | 1.84 (1.06) | 1.63 (.75) | 1.80 | 0.07 |
| Loss of control over one’s life (16) | 8.61 (3.00) | 8.28 (2.71) | 1.12 | 0.26 |
| Personal strain (48) | 22.67 (6.87) | 21.84 (6.41) | 1.45 | 0.15 |
| Role strain (24) | 11.64 (4.71) | 11.06 (4.17) | 1.56 | 0.12 |
| HADS scores | T1 M(SD) | T2 M(SD) | t | p |
| HADSA (21) | 8.24 (4.06) | 8.45 (3.23) | −0.53 | 0.59 |
| HADSD (21) | 6.40 (3.91) | 7.00 (3.28) | −1.47 | 0.14 |
| ZBI Domains (T1/T2) | T1 | T2 | ||
|---|---|---|---|---|
| HADSA | HADSD | HADSA | HADSD | |
| Total Burden | 0.18 | 0.22 | 0.33 ** | 0.33 ** |
| Burden in the relationship | 0.12 | 0.12 | 0.28 * | 0.24 * |
| Emotional burden | 0.12 | 0.20 | 0.31 * | 0.35 ** |
| Social and family life burden | 0.17 | 0.17 | 0.21 | 0.24 * |
| Financial burden | −0.02 | −0.10 | 0.28 * | 0.26 * |
| Loss control over one´s life | 0.27 * | 0.33 ** | 0.38 ** | 0.37 ** |
| Personal Strain | 0.14 | 0.24 * | 0.36 ** | 0.34 ** |
| Role strain | 0.16 | 0.13 | 0.18 | 0.21 |
| Anxiety | b | SE b | β | t |
|---|---|---|---|---|
| Model 1 | ||||
| Constant | 9.78 | 1.98 | 4.92 *** | |
| Cancer type | −0.04 | 0.29 | −0.02 | −0.15 |
| Treatment | −0.18 | 0.18 | −0.13 | −1.00 |
| Cancer stage | 0.27 | 0.34 | 0.10 | 0.80 |
| Type of relationship | −0.26 | 0.33 | −0.10 | −0.78 |
| Employment status | −0.34 | 0.24 | −0.18 | −1.40 |
| Model 2 | ||||
| constant | 7.02 | 2.19 | 3.19 ** | |
| Cancer type | −0.09 | 0.28 | −0.04 | −0.33 |
| Treatment | −1.34 | 0.18 | −0.09 | −0.73 |
| Cancer stage | 0.25 | 0.33 | 0.10 | 0.77 |
| Type of relationship | −0.38 | 0.32 | −0.15 | −1.18 |
| Employment status | −2.87 | 0.23 | −0.15 | −1.20 |
| Emotional burden | 0.23 | 0.09 | 0.31 | 2.50 * |
| Depression | b | SE b | β | t |
|---|---|---|---|---|
| Model 1 | ||||
| Constant | 9.22 | 2.01 | 4.57 *** | |
| Cancer type | 0.04 | 0.27 | 0.01 | 0.14 |
| Treatment | −0.24 | 0.19 | −0.16 | −1.27 |
| Cancer stage | −0.03 | 0.35 | −0.01 | −0.10 |
| Type of relationship | −0.38 | 0.34 | −0.14 | −1.10 |
| Employment status | −0.26 | 0.25 | −0.13 | −1.04 |
| Model 2 | ||||
| constant | 6.00 | 2.19 | 2.74 ** | |
| Cancer type | −0.01 | 0.28 | −0.007 | −0.95 |
| Treatment | −0.18 | 0.18 | −0.12 | −0.99 |
| Cancer stage | −0.59 | 0.33 | −0.02 | −0.18 |
| Type of relationship | −0.52 | 0.32 | −0.20 | −1.59 |
| Employment status | −0.19 | 0.23 | −0.09 | −0.79 |
| Emotional burden | 0.27 | 0.09 | 0.36 | 2.92 ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Torres, F.; Jabłoński, M.J.; Gómez Solís, Á.; Jaén-Moreno, M.J.; Gálvez-Lara, M.; Moriana, J.A.; Moreno-Díaz, M.J.; Aranda, E. Caregiver Burden Domains and Their Relationship with Anxiety and Depression in the First Six Months of Cancer Diagnosis. Int. J. Environ. Res. Public Health 2020, 17, 4101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114101
García-Torres F, Jabłoński MJ, Gómez Solís Á, Jaén-Moreno MJ, Gálvez-Lara M, Moriana JA, Moreno-Díaz MJ, Aranda E. Caregiver Burden Domains and Their Relationship with Anxiety and Depression in the First Six Months of Cancer Diagnosis. International Journal of Environmental Research and Public Health. 2020; 17(11):4101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114101
Chicago/Turabian StyleGarcía-Torres, Francisco, Marcin J. Jabłoński, Ángel Gómez Solís, María José Jaén-Moreno, Mario Gálvez-Lara, Juan A. Moriana, María José Moreno-Díaz, and Enrique Aranda. 2020. "Caregiver Burden Domains and Their Relationship with Anxiety and Depression in the First Six Months of Cancer Diagnosis" International Journal of Environmental Research and Public Health 17, no. 11: 4101. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114101