Associations of City-Level Active Aging and Age Friendliness with Well-Being among Older Adults Aged 55 and Over in Taiwan


Abstract
:1. Introduction
1.1. Active Aging and Age Friendly City
1.2. Theoretical Explanations of Contextual Influence
1.3. Older People’s Well-Being: Individual- and Community-Level Factors and Age Friendly Environment
1.4. Older People’s Active Aging: Individual- and Community-Level Factors and Age Friendly Environment
1.5. Background
2. Materials and Methods
2.1. Data and Sample
2.2. Measures
2.2.1. Individual-Level Data
- Life satisfaction: Life satisfaction was scored from one to five, to indicate very unsatisfactory to very satisfactory, respectively (score 1–5).
- HRQoL: The HRQoL variable was measured based on the 12-Item Short-Form Health Survey HRQoL [52]. Only six variables were covered in the survey. The variables for the physical domain of HRQOL were self-rated health, physical role limitations, and difficulty carrying groceries. The variables for the mental domain of HRQoL were social role limitations, feeling energetic, and feeling depressed. The scoring for each variable was converted to a value of zero to 100, with a higher score representing better health. Thus, the total HRQOL score ranged from zero to 600, with physical HRQOL and mental HRQOL scored of zero to 300 each. The HRQOL variables were only available for the questionnaire for those aged 65 and older.
- Employment: Work (yes/no).
- Social participation: Social participation included volunteering, political participation, family caregiving (children or older family members), and participating in other social group. Each variable was scored yes or no.
- Independent, healthy, and secure living: Physical function independence was measured as having no difficulties or only one item of difficulty in activities of daily living (eating, dressing, transferring, walking indoors, going to the bathroom, bathing). Living independently was defined as living alone or only with a spouse. The financial security variables included home ownership (yes/no) and non-poverty (i.e., a personal income of more than U.S. $600 per month).
- Capacity and supportive environment: Social connection was defined as contact with family or friends at least once a week. Use of information and communications technology (ICT) was defined as using the Internet at least once a week. Mental well-being was defined by not being depressed (yes/no) used for life satisfaction models, and happiness item (yes/no) used for HRQOL models. Lifelong learning was measured by participation in any kind of education program. The public transportation convenience and safety items were coded as either inconvenient, convenient, or not used. Elderly respect was rated as whether the public respects the elderly or not. The control variables for the participants include age (ages 55–59, 60–64, 65–69, 70–74, and 75 and above), gender, education (ordinal), marital status (married or not), and self-rated health (with a score of one to five).
2.2.2. City-Level Data
- Housing: Housing affordability rate.
- Outdoor spaces and buildings: Rate of barrier-free public buildings, rate of barrier-free pathways outside the home, the crime rate, and the neighborhood safety rating.
- Community support and health services: number of medical professionals per population, number of hospital beds per population, and numbers of public libraries.
- Communication and information: Internet usage rate and lifelong learning rate.
- Civic participation and employment: Work rate.
- Social participation: Social group participation rate, volunteer rate, and family caregiving rate.
- Respect and social inclusion: Elderly abuse rate, social connection rate, low-income people percentage of the population, proportion of the elderly who felt respected.
2.3. Analysis
3. Results
4. Discussion
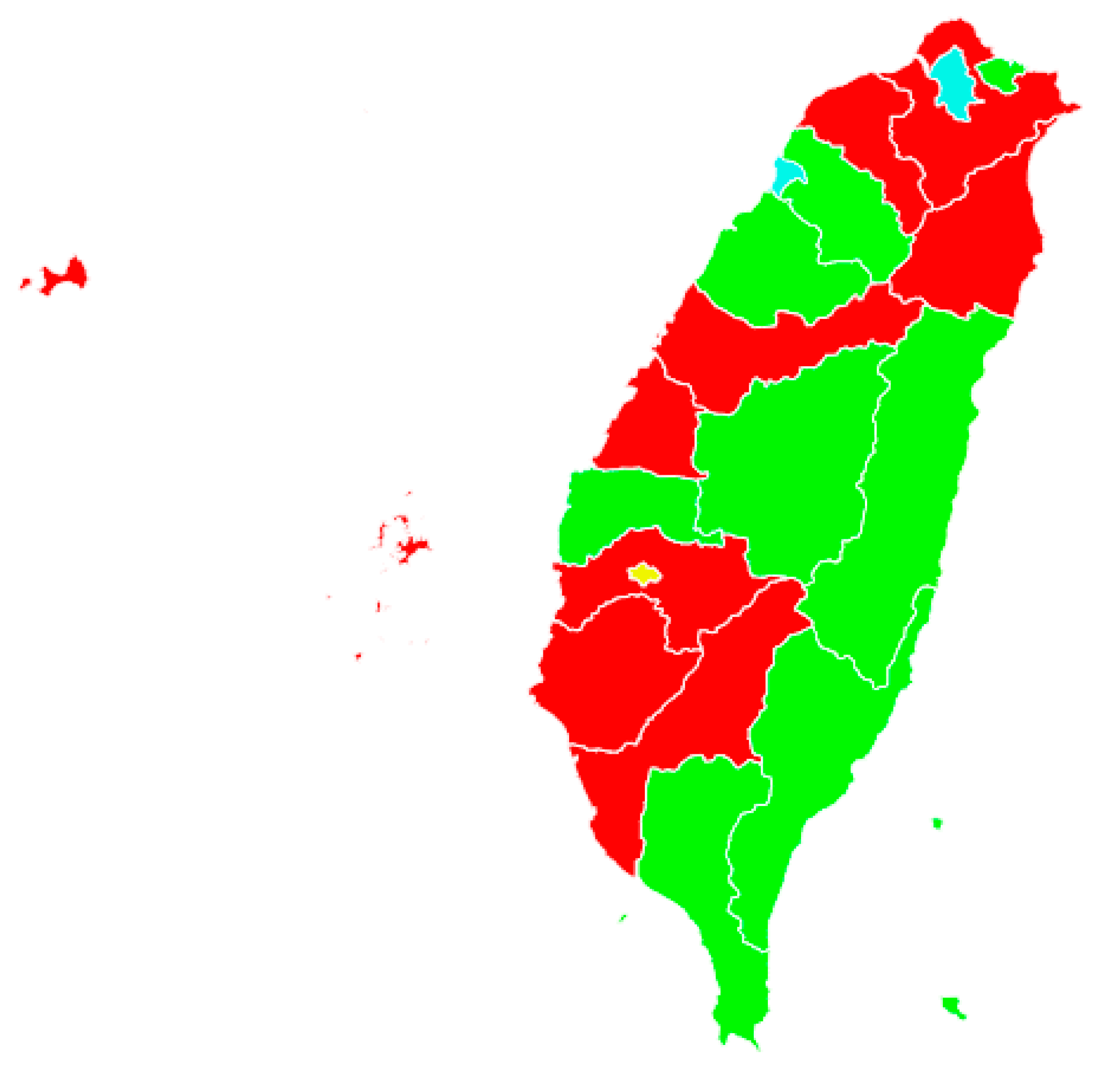
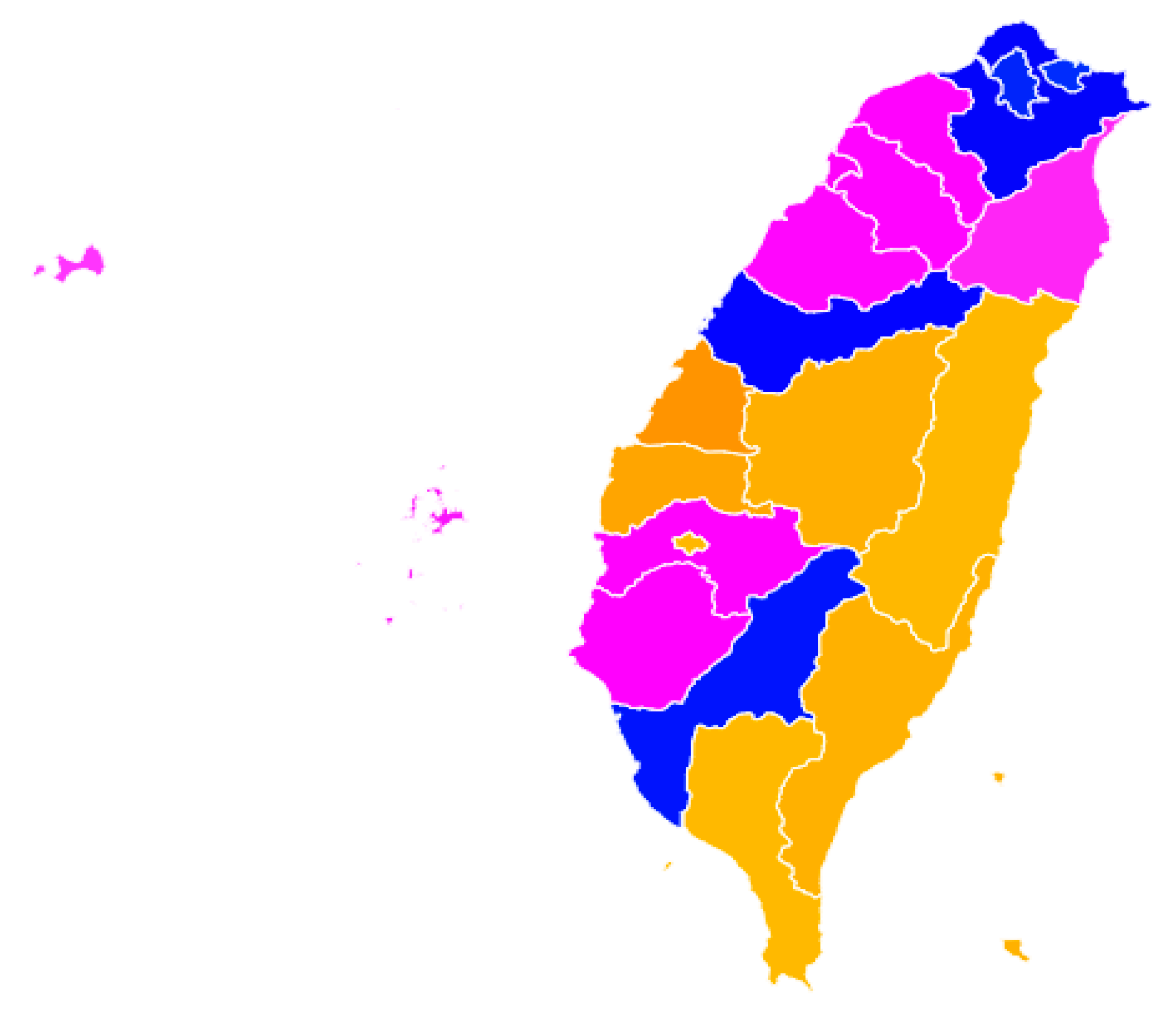
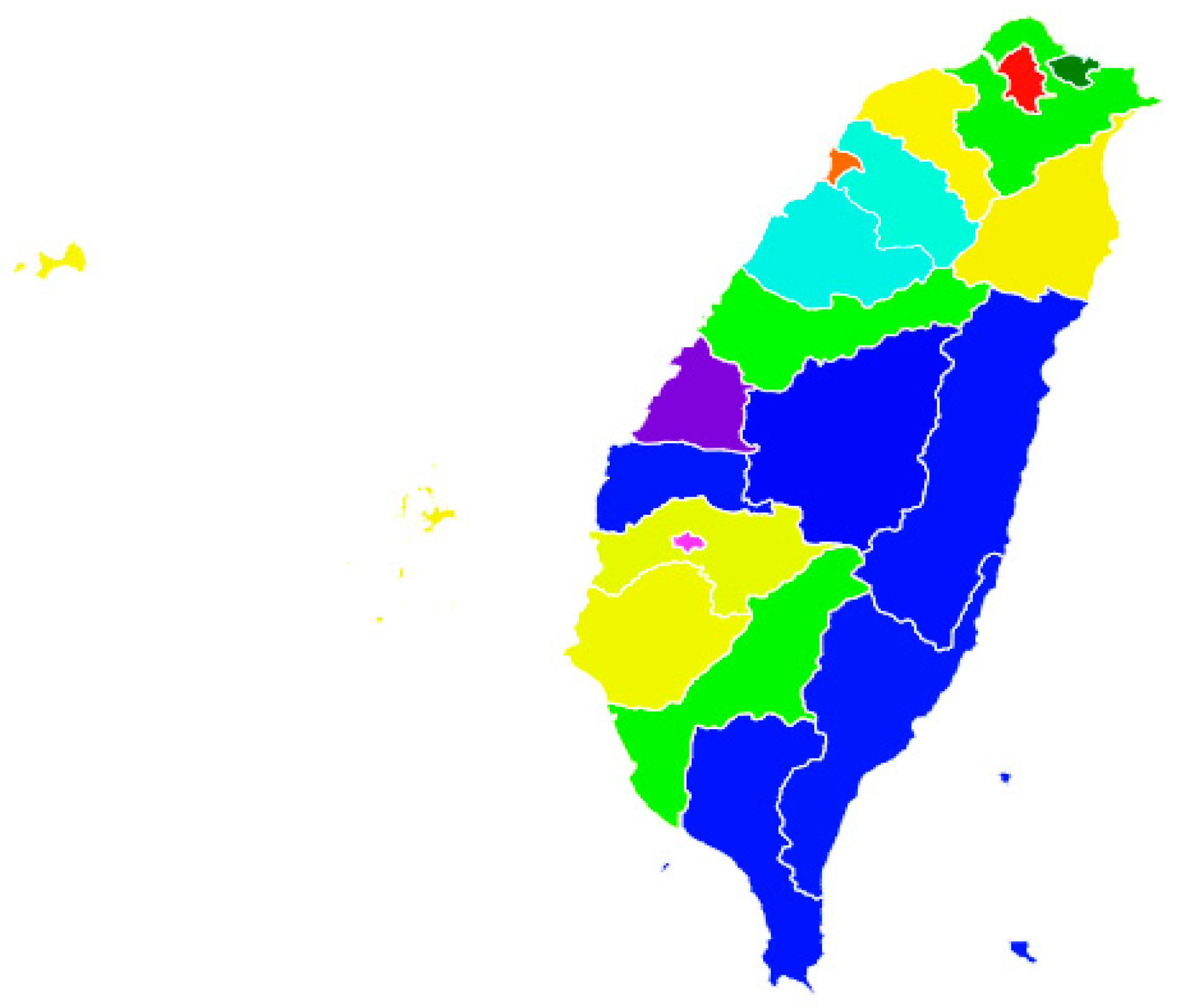
4.1. City Typology and Indicators of Active Aging and Age Friendliness
4.2. City Typology and Well-Being
4.3. Individuals’ Factors Related to Well-Being
4.4. Limitations
5. Conclusions
Supplementary Materials
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Active Aging: A Policy Framework; World Health Organization: Geneva, Switzerland, 2002; p. 12. [Google Scholar]
- Active Aging Group; European Commission (EC) & United Nations Economic Commission for Europe (UNECE). Active Ageing Index (AAI): Concept, Methodology and Final Results; UNECE Grant No: ECE/GC/2012/003; European Centre: Vienna, Austria, 2013. [Google Scholar]
- United Nations Economic Commission for Europe/European Commission. Active Ageing Index 2014: Analytical Report; United Nations Economic Commission for Europe: Geneva, Switzerland, 2015. [Google Scholar]
- Rodríguez-Rodríguez, V.; Rojo-Perez, F.; Fernández-Mayoralas, G.; Morillo-Tomas, R.; Forjaz, J.; Prieto-Flores, M.-E. Active Ageing Index: Application to Spanish Regions. J. Popul. Ageing 2017, 10, 25–40. [Google Scholar] [CrossRef] [Green Version]
- Del Barrio, E.; Rodríguez-Laso, A.; Mayoral, O.; Sancho, M.; Amilibia, L. The Active Ageing Index: A Tool to Develop the Strategy of Active Ageing in the Basque Country (Spain). Build. Evid. Act. Ageing Policies 2018, 139–165. [Google Scholar] [CrossRef]
- Hsu, H.-C.; Liang, J.; Luh, D.-L.; Chen, C.-F.; Lin, L.-J. Constructing Taiwan’s Active Aging Index and Applications for International Comparison. Soc. Indic. Res. 2019, 146, 727–756. [Google Scholar] [CrossRef]
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Havighurst, R.J. Successful Aging. Gerontologist 1961, 1, 8–13. [Google Scholar] [CrossRef]
- Rowe, J.W.; Kahn, R.L. The structure of successful aging. In Successful Aging; Rowe, J.W., Kahn, R.L., Eds.; Dell Publishing: New York, NY, USA, 1997; pp. 36–52. [Google Scholar]
- Kafková, M.P. The Ative Aging Index (AAI) and its relation to the quality of life of older adults. In Building Evidence for Active Ageing Policies: Active Ageing Index and Its Potential; Zaidi, A., Harper, S., Howse, K., Lamura, G., Perek-Bialas, J., Eds.; Springer Nature: Singapore, 2018; pp. 55–74. [Google Scholar]
- Hess, M.; Nauman, E.; Steinkopf, L. Population ageing, the intergenerational conflict, and active ageing policies—A multilevel study of 27 European countries. J. Popul. Aging 2017, 10, 11–23. [Google Scholar] [CrossRef]
- King, A.C.; King, D.K.; Banchoff, A.; Solomonov, S.; Ben Natan, O.; Hua, J.; Gardiner, P.; Rosas, L.G.; Espinosa, P.R.; Winter, S.J.; et al. Employing Participatory Citizen Science Methods to Promote Age-Friendly Environments Worldwide. Int. J. Environ. Res. Public Health 2020, 17, 1541. [Google Scholar] [CrossRef] [Green Version]
- Peek, S.T.M.; Kazak, J.K.; Perek-Białas, J.M.; Peek, S.T.M. The Challenges of Urban Ageing: Making Cities Age-Friendly in Europe. Int. J. Environ. Res. Public Health 2018, 15, 2473. [Google Scholar] [CrossRef] [Green Version]
- Joy, M. Problematizing the age friendly cities and communities program in Toronto. J. Aging Stud. 2018, 47, 49–56. [Google Scholar] [CrossRef]
- Lin, L.-J.; Hsu, Y.-C.; Scharlach, A.E.; Kuo, H.-W. Examining Stakeholder Perspectives: Process, Performance and Progress of the Age-Friendly Taiwan Program. Int. J. Environ. Res. Public Health 2019, 16, 608. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.-C.; Kuo, H.-W.; Lin, C.-C. Current Status and Policy Planning for Promoting Age-Friendly Cities in Taitung County: Dialogue Between Older Adults and Service Providers. Int. J. Environ. Res. Public Health 2018, 15, 2314. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.; Chau, P.H.; Cheung, F.; Phillips, D.R.; Woo, J. Comparing the age-friendliness of different neighborhoods using district surveys: An example of Hong Kong. PLoS ONE 2015, 10, e0131526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, A.H.; Rich, T.A. Ecology and Gerontology: An Introduction. Gerontologist 1968, 8, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, UK, 1979; pp. 3–15. [Google Scholar]
- Thanakwang, K.; Isaramalai, S.-A.; Hatthakit, U. Development and psychometric testing of the active aging scale for Thai adults. Clin. Interv. Aging 2014, 9, 1211–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rantanen, T.; Portegijs, E.; Kokko, K.; Rantakokko, M.; Törmäkangas, T.; Saajanaho, M. Developing an Assessment Method of Active Aging: University of Jyvaskyla Active Aging Scale. J. Aging Health 2018, 31, 1002–1024. [Google Scholar] [CrossRef] [Green Version]
- Sirgy, M.J. Elderly and quality of life. In The Psychology of Quality of Life: Hedonic Well-Being, Life Satisfaction, and Eudaimonia, 2nd ed.; Springer: New York, NY, USA, 2012; pp. 469–486. [Google Scholar]
- Boggatz, T. Quality of life in old age—A concept analysis. Int. J. Older People Nurs. 2015, 11, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.-C. Trajectories and covariates of life satisfaction among older adults in Taiwan. Arch. Gerontol. Geriatr. 2012, 55, 210–216. [Google Scholar] [CrossRef]
- Chen, Y.; Hicks, A.; E While, A. Quality of life of older people in China: A systematic review. Rev. Clin. Gerontol. 2012, 23, 88–100. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2014, 385, 640–648. [Google Scholar] [CrossRef] [Green Version]
- Read, S.; Grundy, E.; Foverskov, E. Socio-economic position and subjective health and well-being among older people in Europe: A systematic narrative review. Aging Ment. Health 2015, 20, 529–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiraphat, S.; Peltzer, K.; Thamma-Aphiphol, K.; Suthisukon, K. The Role of Age-Friendly Environments on Quality of Life among Thai Older Adults. Int. J. Environ. Res. Public Health 2017, 14, 282. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, S. Heterogeneous Age-Friendly Environments among Age-Cohort Groups. Sustainability 2018, 10, 1269. [Google Scholar] [CrossRef] [Green Version]
- Xie, L. Age-Friendly Communities and Life Satisfaction among the Elderly in Urban China. Res. Aging 2018, 40, 883–905. [Google Scholar] [CrossRef] [PubMed]
- Gibney, S.; Zhang, M.; Brennan, C. Age-friendly environments and psychosocial wellbeing: A study of older urban residents in Ireland. Aging Ment. Health 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, S.; Silarova, B.; Martyr, A.; Collins, R.; Ballard, C.; Anstey, K.J.; Kim, S.R.; Clare, L. Associations of Awareness of Age-Related Change With Emotional and Physical Well-being: A Systematic Review and Meta-analysis. Gerontologist 2019, 101. [Google Scholar] [CrossRef] [Green Version]
- Cramm, J.; Nieboer, A.P. Neighborhood attributes security and solidarity promote the well-being of community-dwelling older people in the Netherlands. Geriatr. Gerontol. Int. 2013, 14, 681–688. [Google Scholar] [CrossRef]
- Cramm, J.M.; van Dijk, H.M.; Nieboer, A.P. The importance of neighbourhood social cohesion and social capital for the well being of older adults in the community. Gerontologist 2013, 53, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Zhai, Y.; Xiao, Y.; Newman, G.; Wang, D. Subtypes of park use and self-reported psychological benefits among older adults: A multilevel latent class analysis approach. Landsc. Urban Plan. 2019, 190, 103605. [Google Scholar] [CrossRef]
- Menec, V.H.; Nowicki, S. Examining the relationship between communities age-friendliness’ and life satisfaction and self-perceived health in rural Manitoba, Canada. Rural. Remote Health 2014, 14, 2594. [Google Scholar]
- Lai, M.L.; Lein, S.-Y.; Lau, S.-H.; Lai, M.L. Modeling Age-Friendly Environment, Active Aging, and Social Connectedness in an Emerging Asian Economy. J. Aging Res. 2016, 2016, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Lee, S. Age-friendly environments and life satisfaction among South Korean elders: Person–environment fit perspective. Aging Ment. Health 2016, 21, 693–702. [Google Scholar] [CrossRef]
- Lak, A.; Rashidghalam, P.; Myint, P.K.; Baradaran, H. Comprehensive 5P framework for active aging using the ecological approach: An iterative systematic review. BMC Public Health 2020, 20, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Jeste, D.V.; Blazer, D.G.; Buckwalter, K.C.; Cassidy, K.-L.K.; Fishman, L.; Gwyther, L.P.; Levin, S.M.; Phillipson, C.; Rao, R.R.; Schmeding, E.; et al. Age-Friendly Communities Initiative: Public Health Approach to Promoting Successful Aging. Am. J. Geriatr. Psychiatry 2016, 24, 1158–1170. [Google Scholar] [CrossRef] [PubMed]
- Buils, R.F.; Caballer, A.; Alarcón, A. Evaluation of an Age-Friendly City and Its Effect on Life Satisfaction: A Two-Stage Study. Int. J. Environ. Res. Public Health 2019, 16, 5073. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Z.; Yang, L. (Lydia) Neighborhood Environment, Lifestyle, and Health of Older Adults: Comparison of Age Groups Based on Ecological Model of Aging. Sustainability 2019, 11, 2077. [Google Scholar] [CrossRef] [Green Version]
- Au, A.; Chan, S.; Yip, H.M.; Kwok, J.Y.C.; Lai, K.Y.; Leung, K.M.; Lee, A.L.F.; Lai, D.W.L.; Tsien, T.; Lai, S.M.K. Age-Friendliness and Life Satisfaction of Young-Old and Old-Old in Hong Kong. Curr. Gerontol. Geriatr. Res. 2017, 2017, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, A.; Lai, D.W.L.; Yip, H.-M.; Chan, S.; Lai, S.; Chaudhury, H.; Scharlach, A.; Leeson, G. Sense of Community Mediating Between Age-Friendly Characteristics and Life Satisfaction of Community-Dwelling Older Adults. Front. Psychol. 2020, 11, 86. [Google Scholar] [CrossRef] [Green Version]
- Ko, P.-C.; Yeung, W.-J.J. An Ecological Framework for Active Aging in China. J. Aging Health 2018, 30, 1642–1676. [Google Scholar] [CrossRef]
- Kim, J.; Lee, H.; Cho, E.; Lee, K.H.; Park, C.G.; Cho, B.-H. Multilevel Effects of Community Capacity on Active Aging in Community-Dwelling Older Adults in South Korea. Asian Nurs. Res. 2020, 14, 36–43. [Google Scholar] [CrossRef]
- Ministry of Interior. The Yearly Statistics of Ministry of Interior. Retrieved; 2019. Available online: https://www.moi.gov.tw/files/site_stuff/321/2/year/year.html (accessed on 29 January 2020).
- Directorate-General of Budget, Accounting and Statistics, Executive Yuan, Taiwan, Economic Development Statistics. Available online: https://www.dgbas.gov.tw/point.asp?index=1 (accessed on 29 January 2020).
- Lin, C.C.; Li, T.C.; Liu, C.S.; Lin, H.C.; Lin, W.Y.; Lin, C.H. Report of The Age-Friendly Environment Monitor Study; MOHW104-HPA-H-114-114102; Chinese Medical University: Taichung, Taiwan, 2018. (In Chinese) [Google Scholar]
- Hsu, H.-C.; Liang, J.; Luh, D.-L.; Chen, C.-F.; Wang, Y.-W. Social Determinants and Disparities in Active Aging among Older Taiwanese. Int. J. Environ. Res. Public Health 2019, 16, 3005. [Google Scholar] [CrossRef] [Green Version]
- Arpino, B.; Bordone, V. Active ageing typologies: A latent class analysis of the older Europeans. In Building Evidence for Active Ageing Policies: Active Ageing Index and Its Potential; Zaidi, A., Harper, S., Howse, K., Lamura, G., Perek-Bialas, J., Eds.; Springer Nature: Singapore, 2018; pp. 295–311. [Google Scholar]
- Ware, J.E.; Kosinski, M.; Keller, S.D. SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales, 2nd ed.; The Health Institute, New England Medical Center: Boston, MA, USA, 1995. [Google Scholar]
- Kano, M.; Rosenberg, P.E.; Dalton, S.D. A Global Pilot Study of Age-Friendly City Indicators. Soc. Indic. Res. 2017, 138, 1205–1227. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.-W.; Zebrack, B.J. Caring for family members with chronic physical illness: A critical review of caregiver literature. Health Qual. Life Outcomes 2004, 2, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, H.C. Does social participation by the elderly reduce mortality and cognitive impairment? Aging Ment. Health 2007, 11, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Fu, K.-W. Internet use and Protest Politics in South Korea and Taiwan. J. East Asian Stud. 2018, 19, 89–109. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Unweighted (n = 6920) Mean (SD) or % | Weighted (n = 6,578,754) Mean (SD) or % |
|---|---|---|
| Age | 69.25 (9.93) | 66.43 (9.19) |
| Age 55–59 | 18.6% | 27.2% |
| Age 60–64 | 19.1% | 23.9% |
| Age 65–69 | 19.0% | 18.2% |
| Age 70–74 | 12.4% | 10.3% |
| Age 75–79 | 12.7% | 8.9% |
| Age 80+ | 18.2% | 11.5% |
| Sex: Female | 52.7% | 52.6% |
| Male | 47.3% | 47.4% |
| Residence: Community-based | 90.1% | 98.8% |
| Institution-based | 9.9% | 1.2% |
| Marital status: No spouse | 33.2% | 26.1% |
| Having spouse | 66.8% | 73.9% |
| Education (ordinal, 1–22) | 5.57 (5.27) | 6.06 (5.40) |
| Self-rated health (1–5) | 3.53 (0.94) | 3.60 (0.92) |
| HRQoL (0–600) | 468.20 (127.76) | 480.12 (120.92) |
| HRQoL—physical (0–300) | 222.08 (73.87) | 230.21 (67.57) |
| HRQoL—mental (0–300) | 254.64 (62.64) | 260.18 (59.03) |
| Life satisfaction (1–5) | 3.80 (0.82) | 3.80 (0.81) |
| Work | 24.8% | 31.8% |
| Volunteering | 10.4% | 11.5% |
| Politics | 1.6% | 1.8% |
| Other social groups | 14.0% | 13.9% |
| Family caregiving (children or elderly) | 6.9% | 7.8% |
| Physical independent | 93.6% | 97.0% |
| Not depressed | 72.8% | 75.4% |
| Happy | 84.5% | 85.6% |
| Living alone (or with spouse only) | 8.0% | 7.3% |
| Owning house | 84.9% | 92.8% |
| Non-poverty | 84.9% | 26.0% |
| Social connected | 64.0% | 68.8% |
| Use of Internet | 35.0% | 43.5% |
| Lifelong learning | 5.4% | 5.8% |
| Public transportation: Inconvenient | 3.7% | 4.0% |
| Convenient | 50.4% | 53.4% |
| Non-users | 45.9% | 42.7% |
| Public transportation: Unsafe | 1.4% | 1.4% |
| Safe | 52.7% | 53.4% |
| Non-users | 45.9% | 42.7% |
| Elderly respected | 69.5% | 68.0% |
| Active Aging Indicators (%) | Content (9 Cities) | Developed (2 Cities) | Participatory (8 Cities) | Pioneer (1 City) |
|---|---|---|---|---|
| Work | 0.306 | 0.274 | 0.385 | 0.369 |
| Volunteer | 0.115 | 0.107 | 0.132 | 0.086 |
| Social group participation | 0.129 | 0.178 | 0.152 | 0.184 |
| Politics | 0.016 | 0.023 | 0.027 | 0.011 |
| Family caregiving | 0.077 | 0.084 | 0.086 | 0.085 |
| Physically independent | 0.074 | 0.060 | 0.088 | 0.108 |
| Living alone | 0.074 | 0.060 | 0.088 | 0.108 |
| Non-depressed | 0.773 | 0.698 | 0.730 | 0.632 |
| Owning house | 0.932 | 0.898 | 0.940 | 0.835 |
| Non-poverty | 0.232 | 0.274 | 0.316 | 0.558 |
| Social connected | 0.666 | 0.670 | 0.792 | 0.528 |
| Internet use | 0.416 | 0.537 | 0.398 | 0.499 |
| Lifelong learning | 0.063 | 0.043 | 0.054 | 0.078 |
| Public transportation convenience | 0.958 | 0.992 | 0.949 | 0.992 |
| Transportation safety | 0.988 | 0.978 | 0.982 | 1.000 |
| Elderly respect | 0.669 | 0.761 | 0.669 | 0.736 |
| Higher educated | 0.326 | 0.592 | 0.313 | 0.360 |
| Age Friendly City Indicators (Ranking) 2016 | Insecure | Infrastructural | Tranquil |
|---|---|---|---|
| Work | 16.429 | 6.800 | 7.625 |
| Volunteer | 12.286 | 8.000 | 10.500 |
| Social groups | 13.286 | 12.600 | 6.750 |
| Caregiving | 13.000 | 8.600 | 9.500 |
| Social connected | 13.143 | 10.800 | 8.000 |
| Internet use | 10.000 | 14.400 | 8.500 |
| Lifelong learning | 12.286 | 8.800 | 10.000 |
| Elderly respect | 9.286 | 9.200 | 12.375 |
| Sidewalk for people | 5.286 | 12.500 | 13.813 |
| Medical professionals /population | 10.857 | 13.400 | 8.375 |
| Barrier-free bus accessibility | 14.857 | 9.200 | 7.500 |
| Bus stop accessibility | 8.429 | 14.600 | 9.750 |
| Hospital beds /population | 11.143 | 13.000 | 8.375 |
| Crime rate | 13.286 | 9.600 | 8.625 |
| Low income rate | 13.286 | 14.100 | 5.813 |
| Neighborhood safety | 6.000 | 14.800 | 11.750 |
| Public library numbers | 8.929 | 15.600 | 8.688 |
| Barrier-free public buildings | 13.000 | 8.400 | 9.625 |
| Barrier-free Passage house outside | 15.571 | 8.000 | 7.625 |
| Housing affordability | 13.857 | 3.600 | 11.875 |
| Elderly abuse rate | 11.857 | 11.400 | 8.750 |
| Variables | M1. City Clusters |
|---|---|
| Fixed effects | |
| Constant | 1.720 (0.146) *** |
| Age | 0.051 (0.007) *** |
| Sex (male) | −0.073 (0.021) ** |
| Marry (having spouse) | 0.018 (0.026) |
| Education | 0.010 (0.002) *** |
| Self-rated health | 0.188 (0.012) *** |
| AAC Cluster: Content | 0.267 (0.104) * |
| AAC Cluster: Developed | 0.162 (0.117) |
| AAC Cluster: Participatory | 0.250 (0.099) * |
| AFC Cluster: Infrastructural | −0.017 (0.053) |
| AFC Cluster: Tranquil | 0.010 (0.049) |
| Work | −0.001 (0.024) |
| Volunteering | 0.030 (0.032) |
| Social groups | −0.028 (0.029) |
| Politics | −0.016 (0.074) |
| Caregiving | −0.177 (0.035) *** |
| Physically independent | 0.232 (0.098) * |
| Not depressed | 0.284 (0.023) *** |
| Living alone | −0.179 (0.039) *** |
| Owning house | 0.243 (0.043) *** |
| Non-poverty | 0.055 (0.024) * |
| Socially connected | 0.118 (0.022) *** |
| Internet | 0.061 (0.024) * |
| Lifelong learning | 0.089 (0.044) * |
| Public transportation: convenient | −0.073 (0.086) |
| Public transportation: inconvenient | −0.022 (0.087) |
| Public Transportation: safe | 0.131 (0.084) |
| Elderly respected | 0.253 (0.022) *** |
| Random effects covariance of cities | |
| Residual | 0.549 (0.010) *** |
| AAC clusters | 2.805 × 10−5 (0.002) |
| AFC clusters | 0.003 (0.000) |
| Model fit | −2LL = 13,133.028, BIC = 13,159.015 |
| Variables | M2. HRQoL | M3. HRQoL-Physical | M4. HRQoL-Mental |
|---|---|---|---|
| Fixed effects | |||
| Constant | 129.533 (30,167) *** | 38.029 (14.142) ** | 84.927 (15.083) *** |
| Age | −11.830 (1.712) *** | −7.249 (0.955) *** | −2.922 (0.529) *** |
| Sex (male) | 8.604 (3.888) * | 3.248 (2.169) | 2.221 (1.533) |
| Marital status (have spouse) | 5.941 (4.528) | 3.977 (2.525) | 4.611 (1.871) * |
| Education | 0.005 (0.412) | 0.051 (0.230) | 0.022 (0.158) |
| AAC Cluster: Content | 25.422 (27.938) | 12.460 (11.236) | 14.147 (14.800) |
| AAC Cluster: Developed | −7.507 (32.030) | 1.989 (12.633) | −2.569 (17.046) |
| AAC Cluster: Participatory | 18.193 (26.038) | 10.472 (10.633) | 7.998 (13.696) |
| AFC Cluster: Infrastructural | 22.445 (15.671) | 12.538 (5.788) * | 6.856 (8.577) |
| AFC Cluster: Tranquil | 26.591 (14.160) | 12.802 (5.326) * | 9.758 (7.706) |
| Work | 31.446 (5.277) *** | 18.665 (2.942) *** | 11.626 (1.769) *** |
| Volunteering | 29.198 (6.358) *** | 14.450 (3.544) *** | 11.252 (2.372) *** |
| Social groups | −4.176 (5.202) | 1.873 (2.901) | −7.245 (2.119) ** |
| Politics | −34.220 (13.598) * | −8.756 (7.584) | −16.775 (5.386) ** |
| Caregiving | −8.147 (7.049) | 1.045 (3.932) | −6.477 (2.642)* |
| Physically independent | 258.179 (13.555) *** | 152.858 (7.561) *** | 109.215 (7.100) *** |
| Happy | 33.981 (4.904) *** | 12.573 (2.733) *** | 21.627 (2.048) *** |
| Living alone | −7.684 (6.505) | 1.043 (3.629) | −8.512 (2.859) ** |
| Owning house | 15.986 (8.431) | 8.653 (4.701) | 7.393 (3.119) * |
| Non-poverty | −2.310 (4.807) | −3.013 (2.673) | 3.672 (1.775) * |
| Socially connected | 30.480 (3.875) *** | 14.748 (2.160) *** | 13.797 (1.620) *** |
| Internet use | 23.002 (4.767) *** | 9.644 (2.653) *** | 10.199 (1.787) *** |
| Lifelong learning | 8.379 (8.459) | 1.589 (4.719) | 4.509 (3.193) |
| Public transportation: convenient | 0.556 (15.003) | 12.312 (8.359) | −12.553 (6.297) * |
| Public transportation: inconvenient | −24.949 (15.101) | −6.796 (8.416) | −17.460 (6.380) ** |
| Public Transportation: safe | 39.312 (14.611) ** | 10.705 (8.150) | 25.633 (6.157) *** |
| Respected | 11.381 (3.949) ** | 2.561 (2.201) | 7.182 (1.559) *** |
| Random effects covariance | |||
| Residual | 10,541.207 (257.665) *** | 3283.654 (80.240) *** | 2935.722 (54.675) *** |
| AAC cluster | 29.890 (189.743) | 0.897 (22.487) | 21.767 (54.529) |
| AFC cluster | 353.006 (0.000) | 35.140 (0.000) | 107.141 (0.000) |
| Model fit | −2LL = 40,857.346, BIC = 40,881.706 | −2LL = 36,925.908, BIC = 36,950.268 | −2LL = 62,765.185, BIC = 62,791.171 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, H.-C. Associations of City-Level Active Aging and Age Friendliness with Well-Being among Older Adults Aged 55 and Over in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 4304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124304
Hsu H-C. Associations of City-Level Active Aging and Age Friendliness with Well-Being among Older Adults Aged 55 and Over in Taiwan. International Journal of Environmental Research and Public Health. 2020; 17(12):4304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124304
Chicago/Turabian StyleHsu, Hui-Chuan. 2020. "Associations of City-Level Active Aging and Age Friendliness with Well-Being among Older Adults Aged 55 and Over in Taiwan" International Journal of Environmental Research and Public Health 17, no. 12: 4304. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124304