Effects of Forest Therapy on Health Promotion among Middle-Aged Women: Focusing on Physiological Indicators

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
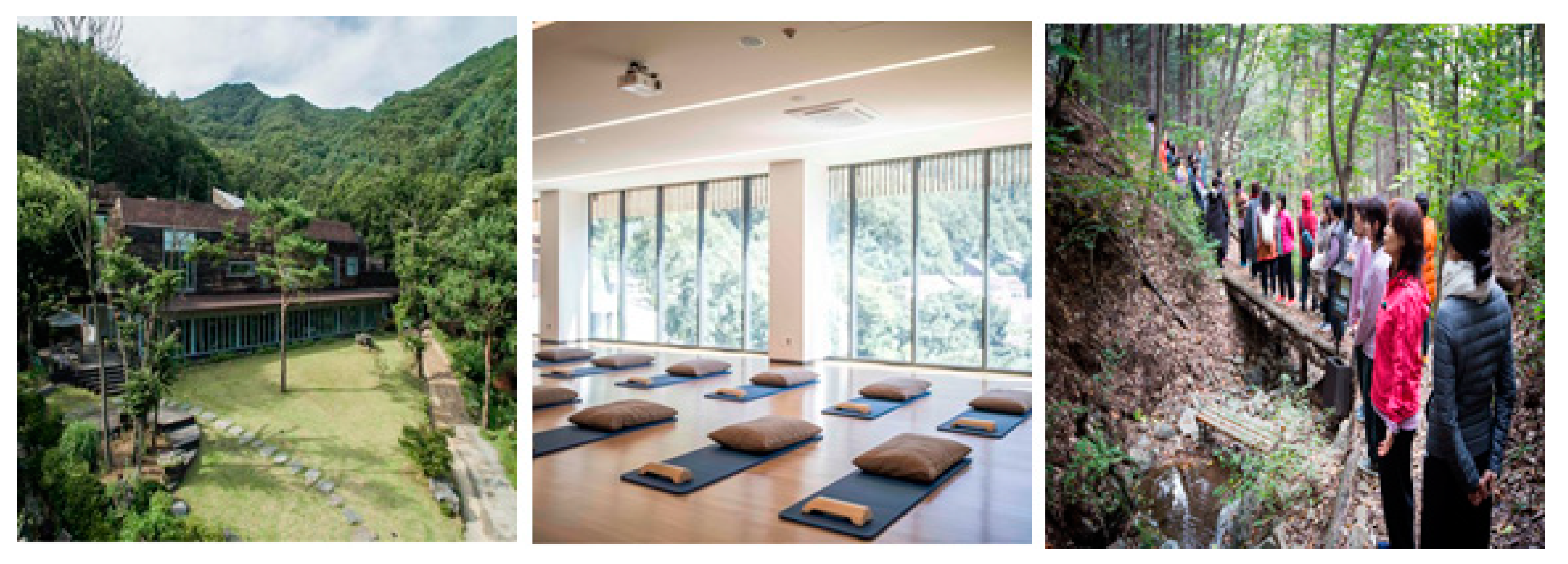
2.2. Study Sites
2.2.1. Forest Site
2.2.2. Urban Site
2.3. Measuring Tools
2.4. Program Setup and Progress
2.5. Data Analysis
3. Empirical Results
3.1. General Characteristics of Subjects
3.2. Physiological Effects of Forest Therapy
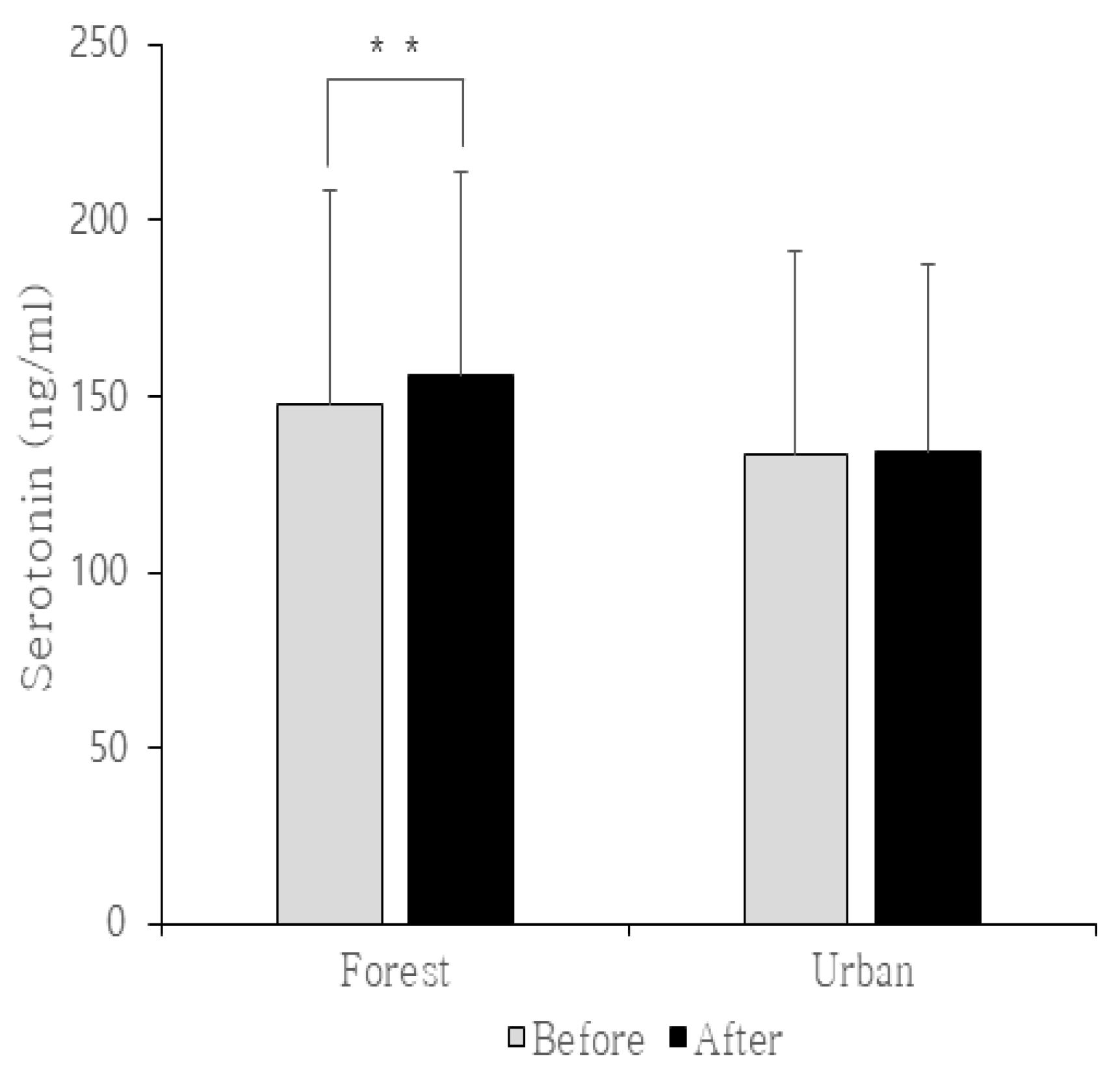
3.2.1. Serotonin
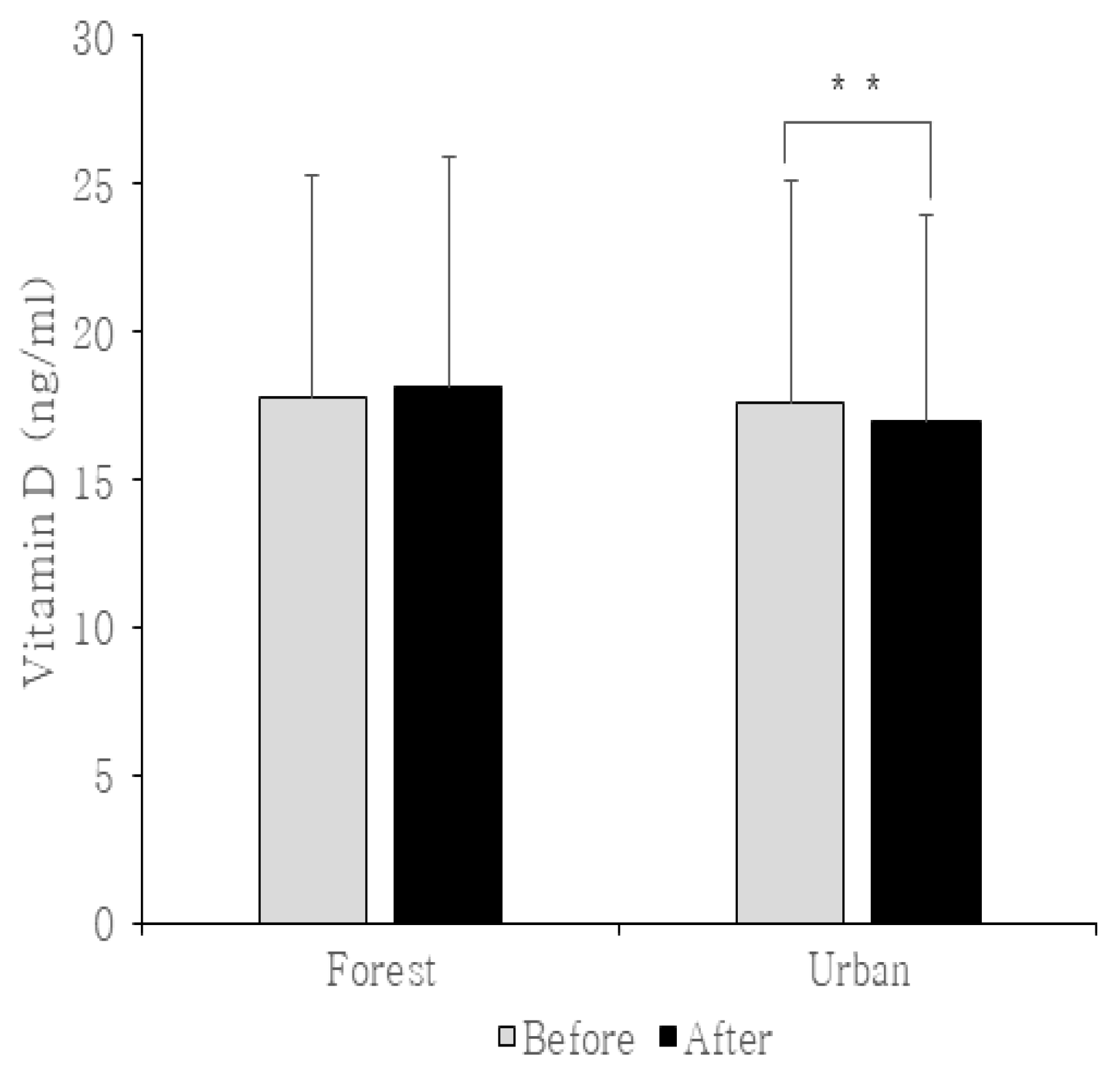
3.2.2. Vitamin D
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Selye, H. The Stress of Life; McGraw-Hill: New York, NY, USA, 1956. [Google Scholar]
- McEwen, S. Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiol. Rev. 2007, 87, 873–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hockey, R. Stress and the cognitive component of skilled performance. In Human Stress and Cognition: An Information Processing Approach; Hamilton, V., Warburton, A., Eds.; John Wiley & Sons: Chichester, UK, 1979; pp. 141–177. [Google Scholar]
- Korte, M.; Koolhaas, M.; Wingfield, C.; McEwen, S. The Darwinian concept of stress: Benefits of allostasis and costs of allostatic load and the trade-offs in health and disease. Neurosci. Biobehav. Rev. 2005, 29, 3–38. [Google Scholar] [CrossRef] [PubMed]
- Bell, M. Stressful life events and coping method in mental illness and illness behavior. Nurs. Res. 1977, 26, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Lee, P.; Lee, Y. Influencing factors on symptoms of stress of middle aged women. J. Korean Acad. Nurs. 2000, 30, 1427–1436. [Google Scholar] [CrossRef]
- Park, J.; Choi, I. The Effect of K-MBSR program on stress, stress coping style, depression, anger and sleep of middle-aged women. J. Korean Acad. Nurs. 2016, 46, 194–206. [Google Scholar] [CrossRef]
- Yeom, J.; Chun, M. The effects of subjective health change on the marital satisfaction change of spouse in middle and old age: Focusing on gender difference. KJGSW 2018, 73, 31–57. [Google Scholar] [CrossRef]
- Trzesniewski, K.; Donnellan, M.; Robins, R. Stability of self-esteem across the life span. J. Personal. Soc. Psychol. 2003, 84, 205–220. [Google Scholar] [CrossRef]
- Park, M.; Kim, K. Effects of yoga exercise program on response of stress, physical fitness and self-esteem in the middle-aged women. KJAN 2014, 26, 22–33. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, R. Aesthetic and affective response to natural environment. In Behavior and the Natural Environment; Springer: Boston, MA, USA, 1983; pp. 85–125. [Google Scholar]
- Orians, G. An ecological and evolutionary approach to landscape aesthetics. In Landscape Meanings and Values; Penning-Rowsell, E.C., Lowenthal, D., Eds.; Allen and Unwin: London, UK, 1986; pp. 3–22. [Google Scholar]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Baur, J.W.; Tynon, J.F. Small-scale urban nature parks: Why should we care? Leis. Sci. 2010, 32, 195–200. [Google Scholar] [CrossRef]
- Heintzman, P. Nature-based recreation and spirituality: A complex relationship. Leis. Sci. 2009, 32, 72–89. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Ikei, H.; Song, C. Forest medicine research in Japan. Nihon Eiseigaku Zasshi 2014, 69, 122–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Kawada, T.; Ohira, T.; et al. Effect of phytoncide from trees on human natural killer function. Int. J. Immunopathol. Pharmacol. 2009, 22, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Kawada, T. Effect of forest therapy on the human psycho-neuro-endocrino-immune network. Nihon Eiseigaku Zasshi 2011, 66, 645–650. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Kobayashi, M.; Inagaki, H.; Hirata, Y.; Li, Y.; Hirata, K.; Kawada, T. A day trip to a forest park increases human natural killer activity and the expression of anti-cancer proteins in male subjects. J. Biol. Regul. Homeost. Agents 2010, 24, 157–165. [Google Scholar] [PubMed]
- Ohira, H.; Takagi, S.; Masui, K.; Oishi, M.; Obata, A. Effect of Shinrinyoku (forest-air bathing and walking): On mental and physical health (in Japanese). Bull. Tokai Women’s Coll. 1999, 9, 217–232. [Google Scholar]
- Park, S.; Woo, J.; Kim, W.; Lee, Y. Sub-populations and disorders that can be applied to forest therapy. J. Korean Inst. For. Recreat. 2012, 16, 35–42. [Google Scholar]
- Yoo, R.; Jeong, S. A Case study on application of the effect using forest on human health improvement and disease prevention. J. Korean Inst. For. Recreat. 2009, 13, 45–51. [Google Scholar]
- Park, H.; Shin, C.; Yeon, P.; Kim, J. A comparative study on the stress recovery effect of forest therapy. J. Korean Inst. For. Recreat. 2014, 18, 13–24. [Google Scholar]
- Song, J.; Cha, J.; Lee, C.; Choi, Y.; Yeon, P. Effects of forest healing program on stress response and spirituality in female nursing college students and their experience. J. Korean Inst. For. Recreat. 2014, 18, 109–125. [Google Scholar] [CrossRef]
- Lee, J.; Yeon, P.; Park, S.; Kang, J. Effects of forest therapy programs on the stress and emotional change of emotional labor workers. J. Korean Inst. For. Recreat. 2018, 22, 15–22. [Google Scholar]
- Park, S.; Yeon, P.; Hong, C.; Yeo, E.; Han, S.; Lee, H.; Kim, Y. A Study on the effect of the forest healing programs on teachers’ stress and PANAS. Korean J. Environ. Ecol. 2017, 31, 606–614. [Google Scholar] [CrossRef]
- Shin, C.; Yeon, P.; Kim, Y.; Um, J.; Im, Y.; Youn, S.; Lee, S. The influence of a forest healing program on public servants in charge of social welfare and mental health care worker’s job stress and the profile of mood states (POMS). J. Korean For. Soc. 2015, 104, 294–299. [Google Scholar] [CrossRef]
- Lee, J. The Influence of forest scenes on psychophysiological responses. J. Korean For. Soc. 2009, 98, 88–93. [Google Scholar]
- Kellert, R.; Wilson, O. The Biophilia Hypothesis; Island Press: Washington, DC, USA, 1993. [Google Scholar]
- Beery, T.; Jönsson, I.; Elmberg, J. From environmental connectedness to sustainable futures: Topophilia and human affiliation with nature. Sustainability 2015, 7, 8837–8854. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Kim, D.; Yeon, P.; Choi, B. The Analysis of Interests and needs for the development of forest therapy program in adults. J. Korean Inst. For. Recreat. 2014, 18, 45–59. [Google Scholar]
- Park, C.; Kim, D.; Park, K.; Shin, C.; Kim, Y. Effects of forest healing programs on resilience and happiness of employees. Korean J. Environ. Ecol. 2018, 32, 667–675. [Google Scholar] [CrossRef]
- Chae, Y.; Kim, J.; Kang, H. Literature review of forest healing therapy on Korean adults. J. Korean Biol. Nurs. Sci. 2018, 20, 122–131. [Google Scholar] [CrossRef]
- Lee, E.; Park, S.; Yoo, R.; Hong, S. Analysis on the activity contents of forest healing programs in Korea. J. Korean Inst. For. Recreat. 2011, 15, 101–109. [Google Scholar]
- Kim, K. The effects of forest walking meditation using mindfulness paradigm on mental health in middle-age women. Korean J. Medit. 2010, 1, 75–97. [Google Scholar]
- Ahn, H.; Lee, K. Towards a working model for an mbsr-informed forest healing program: Focusing on patients with hypertension. J. Korean Inst. For. Recreat. 2013, 17, 1–11. [Google Scholar]
- Shin, W.; Oh, H. The influence of the forest program on depression level. J. Korean Inst. For. Recreat. 1996, 85, 586–595. [Google Scholar]
- Cho, Y.; Shin, W.; Yeon, P. The influence of forest experience program length on sociality and psychology stability of children from low income families. J. Korean Inst. For. Recreat. 2011, 15, 97–103. [Google Scholar]
- Lee, J.; Hong, J.; Tae, Y. Analysis of change of emotion and self-esteem of at-risk children through forest activities. J. Korean Inst. For. Recreat. 2017, 21, 1–9. [Google Scholar] [CrossRef]
- Kim, J.; Shin, C.; Yeon, P.; Lee, J.; Kim, M.; Kim, J.; Yoo, Y. Forest healing program impact on the mental health recovery of elementary school students. J. Korean Inst. For. Recreat. 2013, 17, 69–81. [Google Scholar] [CrossRef]
- Oh, K.; Kim, D.; Kim, J.; Kim, Y. The effects of forest-healing program on developing youth activity competence. Korean J. Youth Stud. 2016, 23, 1–24. [Google Scholar] [CrossRef]
- Eom, P.; Whang, M. Effects of Viewing Environments of Valley, forest road, and city on emotional state based on autonomic nervous system. J. Korean Inst. For. Recreat. 2015, 19, 1–12. [Google Scholar]
- Kim, D.; Lee, S. Effects of forest therapy program in school forest on employment stress and anxiety of university students. PPE 2014, 17, 107–115. [Google Scholar]
- Kim, D.; Kang, H.; Seo, H. Qualitative analysis of emotional labor by forest healing. J. KOEN 2019, 13, 47–56. [Google Scholar]
- Shin, W.; Yeon, P.; Lee, J. The impact that a forest experience influences on a human mental state stability. J. Korean Inst. For. Recreat. 2007, 11, 37–43. [Google Scholar]
- Choi, K.; Shin, W.; Yeon, P.; Cho, Y. The influence of forest walking exercise on human, stress and fatigue. J. Korean Inst. For. Recreat. 2011, 15, 61–66. [Google Scholar]
- Song, J.; Shin, W.; Yeon, P.; Choi, M. The influence of forest therapeutic program on unmarried mothers’ depression and self-esteem. J. Korean For. Soc. 2009, 98, 82–87. [Google Scholar]
- Kim, H.; Lee, Y.; Koo, C.; Yeon, P. The effect of emotional freedom technique (EFT) as forest therapy program on the menopause symptoms and the quality of life of the middle-aged women. J. Korean Inst. For. Recreat. 2016, 20, 83–95. [Google Scholar]
- Lee, Y.; Shin, C. Effects of forest walking meditation on mood states and self-awareness in middle-aged women. J. Korean Inst. For. Recreat. 2015, 19, 19–25. [Google Scholar]
- Shin, C.; Yeon, P.; Cho, M.; Kim, J. Effects of forest healing activity on women’s menopausal symptoms and mental health recovery. PPE 2015, 18, 319–325. [Google Scholar] [CrossRef]
- Yeon, P. The relationships between forest experience and depression. J. Korean Inst. For. Recreat. 2007, 11, 1–6. [Google Scholar]
- Cha, J.; Kim, S.; Cheon, D. Experiences of forest healing program among adult children of alcoholics. J. Korean Inst. For. Recreat. 2016, 20, 99–111. [Google Scholar]
- Choi, J. Effects of forest exercise on the daily activity-related physical function and balance in the elderly. Korean J. Health Phys. Educ. 2011, 50, 465–473. [Google Scholar]
- Kim, J.; Shin, C.; Lee, J. The Effects of forest healing program on mental health and melatonin of the elderly in the urban forest. PPE 2017, 20, 95–106. [Google Scholar] [CrossRef]
- Sin, B.; Lee, K. The effects of forest bathing on social psychological and job stress. J. Naturop. 2018, 7, 51–62. [Google Scholar]
- Lee, B.; Lee, H. Effects of occupational and social stresses after forest therapy. J. Naturop. 2013, 2, 108–114. [Google Scholar]
- Lee, J.; Park, B.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Olafsdottir, G.; Cloke, P.; Vögele, C. Place, green exercise and stress: An exploration of lived experience and restorative effects. Health Place 2017, 46, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Gidlow, C.; Jones, M.; Hurst, G.; Masterson, D.; Clark-Carter, D.; Tarvainen, M.; Nieuwenhuijsen, M. Where to put your best foot forward: Psycho-physiological responses to walking in natural and urban environments. J. Environ. Psychol. 2016, 45, 22–29. [Google Scholar] [CrossRef]
- Stigsdotter, U.; Corazon, S.; Sidenius, U.; Kristiansen, J.; Grahn, P. It is not all bad for the grey city–A crossover study on physiological and psychological restoration in a forest and an urban environment. Health Place 2017, 46, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Mao, G.; Lan, X.; Cao, Y.; Chen, Z.; He, Z.; Lv, Y.; Wang, Y.; Hu, X.; Wang, G.; Jing, Y. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar] [PubMed]
- Kjellgren, A.; Buhrkall, H. A comparison of the restorative effect of a natural environment with that of a simulated natural environment. J. Environ. Psychol. 2010, 30, 464–472. [Google Scholar] [CrossRef]
- Levinson, D. A conception of adult development. Am. Psychol. 1986, 41, 3–13. [Google Scholar] [CrossRef]
- Buhler, C.; Massarik, F.; Bugental, J. The Course of Human Life; Springer: New York, NY, USA, 1968. [Google Scholar]
- McLeod, S.A.; Erikson, E. Psychosocial Stages Simply Psychology. 2008. Available online: http://www.simplypsychology.org/Erik-Erikson.html (accessed on 17 June 2020).
- Tsunetsugu, Y.; Park, B.J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in an old-growth broadleaf forest in Yamagata prefecture. Jpn. J. Physiol. Anthropol. 2007, 26, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across. Jpn. Environ. Health Prev. Med. 2010, 15, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, C.; Joung, D.; Ikei, H.; Igarashi, M.; Aga, M.; Park, B.; Miyazaki, Y. Physiological and psychological effects of walking on young males in urban parks in winter. J. Physiol. Anthropol. 2013, 32, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Sari, Y.; Zhang, J.; Goodlett, C.; Li, T. Prenatal alcohol exposure retards the migration and development of serotonin neurons in fetal C57BL mice. Dev. Brain Res. 2001, 126, 147–155. [Google Scholar] [CrossRef]
- Svenningsson, P.; Chergui, K.; Rachleff, I.; Flajolet, M.; Zhang, X.; El Yacoubi, M.; Vaugeois, J.; Nomikos, G.; Greengard, P. Alterations in 5-HT1B receptor function by p11 in depression-like states. Science 2006, 311, 77–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M. Resurrection of vitamin D deficiency and rickets. J. Clin. Investig. 2006, 116, 2062–2072. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.; Ajani, U.; McGuire, L.; Liu, S. Concentrations of serum vitamin D and the metabolic syndrome among U.S. adults. Diabetes Care 2005, 28, 1228–1230. [Google Scholar] [CrossRef] [Green Version]
- Mitri, J.; Muraru, M.; Pittas, A. Vitamin D and type 2 diabetes: A systematic review. Eur. J. Clin. Nutr. 2011, 65, 1005–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Q.; Shi, L.; Rimm, E.; Giovannucci, E.; Hu, F.; Manson, J.; Rexrode, K. Vitamin D intake and risk of cardiovascular disease in US men and women. Am. J. Clin. Nutr. 2011, 94, 534–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovannucci, E. Vitamin D and cancer incidence in the Harvard cohorts. Ann. Epidemiol. 2019, 19, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Ganji, V.; Milone, C.; Cody, M.; McCarty, F.; Wang, Y. Serum vitamin D concentrations are related to depression in young adult US population: The Third National Health and Nutrition Examination Survey. Int. Arch. Med. 2010, 3, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milaneschi, Y.; Shardell, M.; Corsi, A.; Vazzana, R.; Bandinelli, S.; Guralnik, J.; Ferrucci, L. Serum 25-hydroxyvitamin D and depressive symptoms in older women and men. J. Clin. Endocrinol. Metab. 2010, 95, 3225–3233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, R.; Hirani, V. Relationship between vitamin D levels and depressive symptoms in older residents from a national survey population. Psychosom. Med. 2010, 72, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Mindfulness for Beginners: Reclaiming the Present Moment and Your Life; Sounds True: Boulder, CO, USA, 2012. [Google Scholar]
- Bondy, B.; Erfurth, A.; Jonge, S.; Kruger, M.; Meyer, H. Possible association of the short allele of the serotonin transporter promoter gene polymorphism(5-HTTLPR) with violent suicided. Mol. Psychiatry 2000, 5, 193–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, S.; Kim, H.; Park, S. An influence of iong entraining of Taekwondo of middle-aged women on her dopamine, serotonin and stress hormone. Exerc. Sci. 2009, 18, 247–256. [Google Scholar] [CrossRef]
- Cho, E. The Effect of Dance Sport Exercise on Neurotransmitter and Concentration in Youth. Master’s Thesis, Myongji University, Seoul, Korea, 2011. [Google Scholar]
- Soares, J.; Naffah-Mazzacoratti, M.; Canalheiro, E. Increased serotonin levels in physically traind men. Braz. J. Med. Biol. Res. 1994, 27, 1635–1638. [Google Scholar] [PubMed]
- Barchas, J.D.; Freedman, D. Brainamines. Biochem. Pharmacol. 1963, 12, 1232–1235. [Google Scholar] [CrossRef]
- Romanowski, W.; Grabiec, S. The role of serotonin in the mechanism of central fatigue. Acta Physiol. Pol. 1974, 25, 127–134. [Google Scholar]
- Hong, S.; Lee, D.; Lee, G. The effects of low intensity muscle strengthening on norepinephrine and epinephrine serotonin level in stroke patients with depression or emotional incontinence. KSIM 2018, 6, 69–76. [Google Scholar]
- Baek, I.; Kim, B.; Park, K. The effect of circuit class training on the synthesis of central serotonin in people. J. Korean Soc. Phys. Med. 2012, 7, 451–458. [Google Scholar] [CrossRef]
- Im, D.; Baek, I.; Yoon, B.; Park, C. Effect of 8-weeks’ balance training on depression inventory and serotonin in individuals post-stroke. KSW 2012, 7, 155–161. [Google Scholar]
- Yoon, D.; Park, J.; Cho, S.; Park, M.; Kim, S.; Choi, J. Depressive symptomatology and metabolic syndrome in Korean women. J. Obes. Metab. Syndr. 2005, 14, 213–219. [Google Scholar]
- Wipfli, B.; Landers, D.; Nagoshi, C.; Ringenbach, S. An examination of serotonin and psychological variables in the relationship between exercise and mental health. Scand. J. Med. Sci. Sports 2011, 21, 474–481. [Google Scholar] [CrossRef]
- Morgan, W.; Brown, D.; Raglin, J. Psychological monitoring of overtraining and staleness. Br. J. Sports Med. 1987, 21, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youn, T.; Kim, H.; Jung, W.; Lee, M. Effects of 12 weeks of yoga training program on physical fitness and cardiorespiratory function in middle-aged women. Korean J. Health Phys. Educ. 2017, 56, 561–572. [Google Scholar] [CrossRef]
- Kim, H. Effects of 20 Weeks Yoga on Neurotransmitter in Educable Mentally Retarded Teenagers. Master’s Thesis, Sookmyung Women’s University, Seoul, Korea, 2007. [Google Scholar]
- Yoo, J. Effect of yoga exercise on blood pressure, physical fitness, and blood variables in elderly with vascular dementia. KJGD 2010, 18, 217–226. [Google Scholar]
- An, H.; Kim, I.; Kim, Y. Analysis of the effect on geriatric depression by aromatherapy. J. Soc. Occup. Ther. Aged Dement. 2014, 8, 12–26. [Google Scholar]
- Vyssoki, B.; Praschak-Rieder, N.; Sonneck, G.; Bluml, V.; Willeit, M.; Kasper, S.; Kapusta, N. Effects of sunshine on suicide rates. Compr. Psychiatry 2012, 53, 535–539. [Google Scholar] [CrossRef]
- An, J.; Kim, J. A brain-scientific interpretation of the mental and physical healing by the Buddhist meditation. Buddhism Res. 2014, 41, 447–479. [Google Scholar]
- Yang, E.; Seo, S.; Jeong, K.; Yoon, H.; Lee, D.; Hwang, B. The effects of short-term meditation and walking exercise in a forest on blood pressure, heart rate, NK-cell and POMS. J. Kinesiol. 2011, 13, 31–40. [Google Scholar]
- Manocha, R. Why meditation. Aust. Fam. Phys. 2000, 29, 1135–1138. [Google Scholar]
- Jones, M. Changes in cytokine production in healthy subjects practicingGuolin Qigong: A pilot study. BMC Complement. Altern. Med. 2001, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Walton, G.; Pugh, D.; Gelderloos, P.; Macrae, P. Stress reduction and preventing hypertension. J. Altern. Complement. Med. 1995, 1, 263–283. [Google Scholar] [CrossRef]
- Tooley, G.; Armstrong, S.; Norman, T.; Sali, A. Acute increases in night-time plasma melatonin levels following a period of meditation. Biol. Psychol. 2000, 53, 69–78. [Google Scholar] [CrossRef]
- Shin, Y. Differences of Psychophysiological Effects between Meditative and Athletic Walking in a Forest and Gymnasium. Ph.D. Thesis, The Catholic University of Korea, Seoul, Korea, 2012. [Google Scholar]
- May, H.; Bair, T.; Lappe, D.; Anderson, J.; Horne, B.; Carlquist, J.; Muhlestein, A. Association of vitamin D levels with incident depression among a general cardiovascular population. Am. Heart J. 2010, 159, 1037–1043. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Program | Description of Content |
|---|---|
| Lying-down meditation | Meditation for fatigue relief and correct sleep habit building through relaxing meditation with deep rest, which relaxes the whole body while lying down |
| Seon yoga | Yoga consisting of actions to unwind joints that even beginners can easily follow |
| Serotonin walking | Walking that relaxes the body with stretching while appreciating the joy of walking and feeling one’s own breathing, leading to mental relaxation |
| Healing touch | Massage in pairs of participants that relieves muscle tension using props |
| Stress relief meditation | Meditation to relieve stress, understand the internal and external causes of stress, and practice mental habits for the effective prevention and relief of stress |
| Natural meditation | Meditation that facilitates the understanding of the inner and outer self through the five senses, leading to the restoration of the five senses and relaxation |
| Time | Day 1 | Day 2 | Day 3 |
|---|---|---|---|
| 7:00–8:00 a.m. | Serotonin walking on a forest trail | ||
| 8:00–9:00 a.m. | |||
| 9:00–10:00 a.m. | 9:30 Natural meditation | ||
| 10:00–11:00 a.m. | Orientation | ||
| 11:00–12:00 a.m. | 10:30 Questionnaire completion, blood collection | 10:30 Questionnaire completion, blood collection | |
| 12:00–1:00 p.m. | |||
| 1:00–2:00 p.m. | 1:30 p.m. Lying-down meditation | 1:30 p.m. Lying-down meditation | |
| 2:00–3:00 p.m. | |||
| 3:00–4:00 p.m. | Seon yoga | Healing touch | |
| 4:00–5:00 p.m. | |||
| 5:00–6:00 p.m. | |||
| 6:00–7:00 p.m. | |||
| 7:00–8:00 p.m. | |||
| 8:00–9:00 p.m. | Stress relief meditation |
| Time | Day 1 | Day 2 | Day 3 |
|---|---|---|---|
| 7:00–8:00 a.m. | |||
| 8:00–9:00 a.m. | |||
| 9:00–10:00 a.m. | |||
| 10:00–11:00 a.m. | Orientation | Serotonin walking on a tree-lined street | 10:30 Natural meditation |
| 11:00–12:00 a.m. | 10:30 Questionnaire completion, blood collection | Healing touch | 11:30 Questionnaire completion, blood collection |
| 12:00–1:00 p.m. | |||
| 1:00–2:00 p.m. | 1:30 p.m. Lying-down meditation | 1:30 p.m. Lying-down meditation | |
| 2:00–3:00 p.m. | Seon yoga | Stress relief meditation |
| Variables | Items | Number of Persons | % |
|---|---|---|---|
| Age | 40–49 | 15 | 28 |
| 50–59 | 27 | 51 | |
| 60–65 | 11 | 21 | |
| Education level | High-school graduate or lower | 15 | 28 |
| College student | 8 | 15 | |
| College graduate | 22 | 42 | |
| Graduate student or higher | 8 | 15 | |
| Household income (KRW) | Less than 2 million | 6 | 11 |
| 2 million–less than 3 million | 7 | 13 | |
| 3 million–less than 4 million | 10 | 19 | |
| 4 million–less than 5 million | 9 | 17 | |
| 5 million–less than 6 million | 5 | 9 | |
| 6 million or higher | 16 | 30 | |
| Residence area | Seoul | 25 | 47 |
| Capital area | 23 | 43 | |
| Provincial area | 5 | 9 | |
| Occupation | Self-employed | 6 | 11 |
| Office job | 5 | 9 | |
| Specialist | 4 | 8 | |
| Service industry job | 3 | 6 | |
| Full-time homemaker | 28 | 53 | |
| Other | 7 | 13 |
| Variable | Before | After | t | p |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| Forest (n = 53) | 147.62 (61.21) | 156.28 (57.83) | −3.59 ** | 0.001 |
| Urban (n = 53) | 133.52 (57.72) | 134.22 (53.40) | −0.44 | 0.67 |
| Variable | Before | After | t | p |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| Forest (n = 53) | 17.81 (7.45) | 18.11 (7.84) | −1.66 | 0.10 |
| Urban (n = 53) | 17.62 (7.45) | 16.95 (7.02) | 3.70 ** | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, B.-J.; Shin, C.-S.; Shin, W.-S.; Chung, C.-Y.; Lee, S.-H.; Kim, D.-J.; Kim, Y.-H.; Park, C.-E. Effects of Forest Therapy on Health Promotion among Middle-Aged Women: Focusing on Physiological Indicators. Int. J. Environ. Res. Public Health 2020, 17, 4348. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124348
Park B-J, Shin C-S, Shin W-S, Chung C-Y, Lee S-H, Kim D-J, Kim Y-H, Park C-E. Effects of Forest Therapy on Health Promotion among Middle-Aged Women: Focusing on Physiological Indicators. International Journal of Environmental Research and Public Health. 2020; 17(12):4348. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124348
Chicago/Turabian StylePark, Bum-Jin, Chang-Seob Shin, Won-Sop Shin, Chung-Yeub Chung, Si-Hyung Lee, Dong-Jun Kim, Youn-Hee Kim, and Chang-Eun Park. 2020. "Effects of Forest Therapy on Health Promotion among Middle-Aged Women: Focusing on Physiological Indicators" International Journal of Environmental Research and Public Health 17, no. 12: 4348. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124348