Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China


Abstract
:1. Introduction
2. Theoretical Framework
3. Methods
3.1. Procedure and Participants
3.2. Measures
3.2.1. Rural–Urban Residence
3.2.2. Preventive Behaviors
3.2.3. Sociodemographic
3.3. Potential Mediation Variables
3.3.1. Behavioral Intention
3.3.2. Attitude
3.3.3. Subjective Norms
3.3.4. Knowledge about Preventive Behaviors
3.3.5. Variety of Interpersonal Information Source
3.3.6. Variety of Media Information Source
3.3.7. Information Appraisal
4. Data Analysis
4.1. Simple Linear Regressions
4.2. Multiple Linear Regressions
4.3. Path Analysis
5. Results
5.1. Simple Linear Regressions
5.2. Multiple Linear Regressions
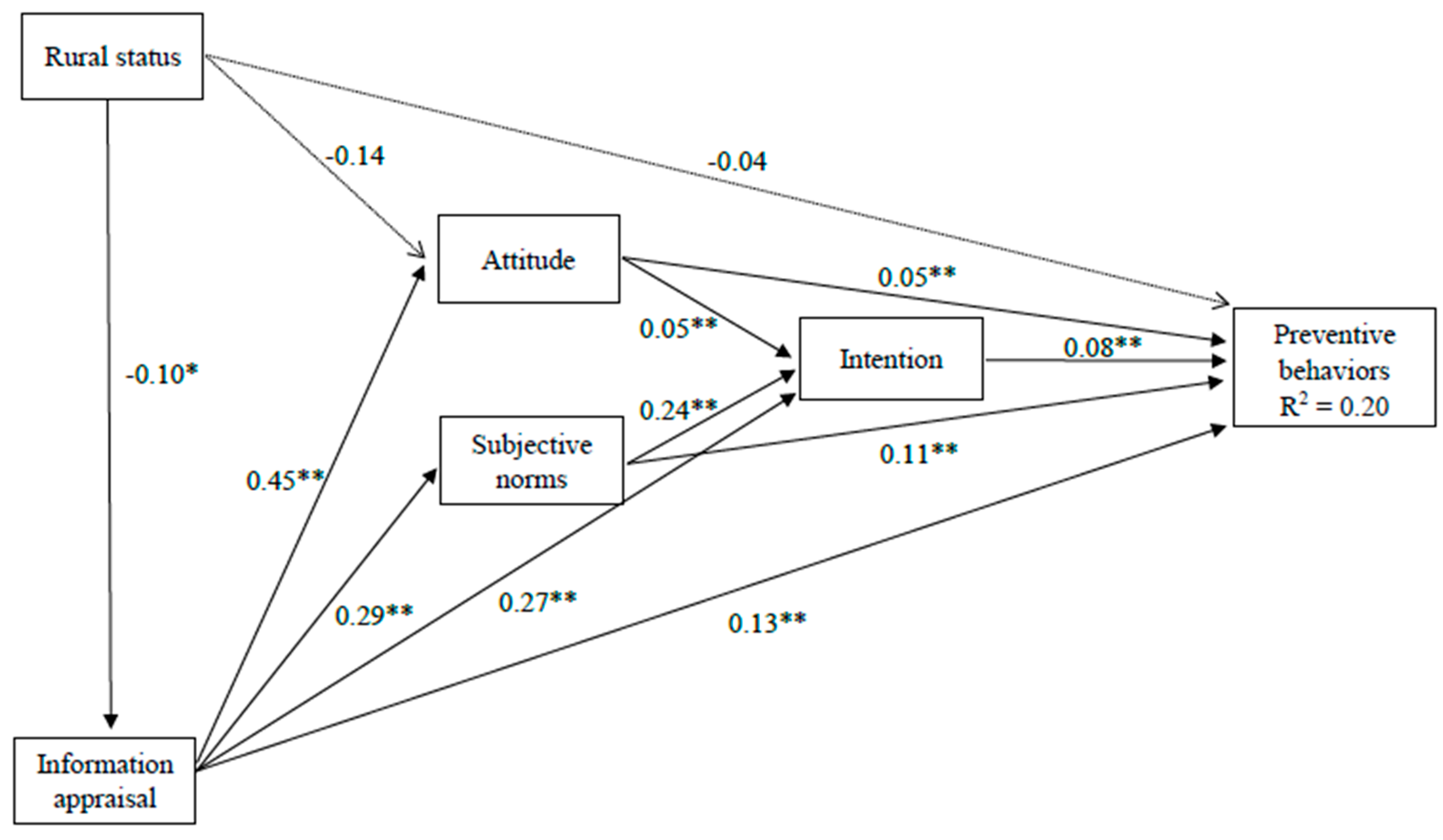
5.3. Path Analysis
5.3.1. Direct Effect
5.3.2. Indirect Effect
5.3.3. Total Effect
6. Discussion
7. Limitations
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sparks, P.J. Rural health disparities. In International Handbook of Rural Demography; Kulcsár, L.J., Curtis, K.J., Eds.; Springer: Amsterdam, The Netherlands, 2012; pp. 255–271. [Google Scholar]
- Thomas, T.L.; DiClemente, R.; Snell, S. Overcoming the triad of rural health disparities: How local culture, lack of economic opportunity, and geographic location instigate health disparities. Health Educ. J. 2014, 73, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Zahnd, W.E.; James, A.S.; Jenkins, W.D.; Izadi, S.R.; Fogleman, A.J.; Steward, D.E.; Colditz, G.A.; Brard, L. Rural-urban differences in cancer incidence and trends in the United States. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1265–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O‘Connor, A.; Wellenius, G. Rural-urban disparities in the prevalence of diabetes and coronary heart disease. Public Health 2012, 126, 813–820. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, K.; Cai, L.-B.; Xu, F.-R.; Wang, P.-G.; Xue, H.-L.; Ye, Y.-L.; Xiong, S.-Z.; Liu, Z.-M.; He, Q.-Q. Urban-rural differences in cardiovascular disease risk factors: A cross-sectional study of schoolchildren in Wuhan, China. PLoS ONE 2015, 10, e0137615. [Google Scholar] [CrossRef]
- Kasl, S.V.; Cobb, S. Health behavior, illness behavior and sick role behavior: I. Health and illness behavior. Arch. Environ. Health Int. J. 1966, 12, 246–266. [Google Scholar] [CrossRef]
- Chen, X.; Cisse-Egbuonye, N.; Spears, E.C.; Mkuu, R.; McKyer, E.L. Children’s healthy eating habits and parents’ socio-demographic characteristics in rural Texas, USA. Health Educ. J. 2018, 77, 444–457. [Google Scholar] [CrossRef]
- Zahnd, W.E.; Goldfarb, J.; Scaife, S.L.; Francis, M.L. Rural-urban differences in behaviors to prevent skin cancer: An analysis of the Health Information National Trends Survey. J. Am. Acad. Dermatol. 2010, 62, 950–956. [Google Scholar] [CrossRef]
- Doescher, M.P.; Jackson, J.E. Trends in cervical and breast cancer screening practices among women in rural and urban areas of the United States. J. Public Health Manag. Pract. 2009, 15, 200–209. [Google Scholar] [CrossRef] [Green Version]
- El Bcheraoui, C.; Mokdad, A.H.; Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Shirude, S.; Naghavi, M.; Murray, C.J. Trends and patterns of differences in infectious disease mortality among US counties, 1980–2014. JAMA 2018, 319, 1248–1260. [Google Scholar] [CrossRef]
- Liu, H.; Li, M.; Jin, M.; Jing, F.; Wang, H.; Chen, K. Public awareness of three major infectious diseases in rural Zhejiang province, China: A cross-sectional study. BMC Infect. Dis. 2013, 13, 192. [Google Scholar] [CrossRef] [Green Version]
- Santibañez, S.; Bellis, K.S.; Bay, A.; Chung, C.L.; Bradley, K.; Gibson, D.; Shultz, A. Strengthening rural states’ capacity to prepare for and respond to emerging infectious diseases, 2013–2015. South. Med. J. 2019, 112, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Xin, G.; Duan, G. A pilot study of health management mode of infectious diseases in rural communities. Chin. Rural Health Serv. Adm. 2014, 34, 1356–1359. [Google Scholar]
- WHO Rolling Updates on Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 21 April 2020).
- Johns Jopkins University Coronavirus Resource Center. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 12 May 2020).
- Centers for Disease Control and Prevention People Who Are at Higher Risk For Severe Illness. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-at-higher-risk.html (accessed on 12 May 2020).
- Curley, C. Rural America Could Be the Region Hardest Hit by the COVID-19 Outbreak. Available online: https://www.healthline.com/health-news/rural-america-hardest-hit-by-covid-19-outbreak (accessed on 21 April 2020).
- Williams, M.A.; Gelaye, B.; Leib, E.M.B. The COVID-19 Crisis Is Going to Get Much Worse When It Hits Rural Areas. Available online: https://www.washingtonpost.com/opinions/2020/04/06/covid-19-crisis-is-going-get-much-worse-when-it-hits-rural-areas/ (accessed on 21 April 2020).
- Prusaczyk, B. Strategies for disseminating and implementing COVID-19 public health prevention practices in rural areas. J. Rural Health 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henning-Smith, C.; Tuttle, M.; Kozhimannil, K.B. Unequal distribution of COVID-19 risk among rural residents by race and ethnicity. J.Rural Health 2020. [Google Scholar] [CrossRef]
- American Heart Association News Far From Immune, Rural Areas Face Unique COVID-19 Challenges. Available online: https://www.heart.org/en/news/2020/04/30/far-from-immune-rural-areas-face-unique-covid-19-challenges (accessed on 11 May 2020).
- Liu, X.; Zhang, D.; Sun, T.; Li, X.; Zhang, H. Containing COVID-19 in rural and remote areas: Experiences from China. J. Travel Med. 2020. [Google Scholar] [CrossRef]
- Van den Broucke, S. Why health promotion matters to the COVID-19 pandemic, and vice versa. Health Promot. Int. 2020, 35, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Van Bavel, J.J.; Boggio, P.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.; Crum, A.; Douglas, K.; Druckman, J.; Drury, J.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Ajzen, H.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley Publishing Company: Reading, MA, USA, 1977. [Google Scholar]
- Ajzen, I.; Albarracin, D.; Hornik, R. Prediction and Change of Health Behavior: Applying the Reasoned Action Approach; Psychology Press: London, UK, 2007. [Google Scholar]
- Chen, X.; Orom, H.; Hay, J.L.; Waters, E.A.; Schofield, E.; Li, Y.; Kiviniemi, M.T. Differences in rural and urban health information access and use. J. Rural Health 2019, 35, 405–417. [Google Scholar] [CrossRef]
- Abel, T.; McQueen, D. Critical health literacy and the COVID-19 crisis. Health Promot. Int. 2020. [Google Scholar] [CrossRef]
- Chinn, D. Critical health literacy: A review and critical analysis. Soc. Sci. Med. 2011, 73, 60–67. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, H.; Takeuchi, T.; Yano, E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care 2008, 31, 874–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubinelli, S.; Schulz, P.J.; Nakamoto, K. Health literacy beyond knowledge and behaviour: Letting the patient be a patient. Int. J. Public Health 2009, 54, 307–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diviani, N. On the centrality of information appraisal in health literacy research. HLRP Health Lit. Res. Pract. 2019, 3, e21–e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldoory, L. The status of health literacy research in health communication and opportunities for future scholarship. Health Commun. 2017, 32, 211–218. [Google Scholar] [CrossRef]
- Pleasant, A.; McKinney, J.; Rikard, R. Health literacy measurement: A proposed research agenda. J. Health Commun. 2011, 16, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Aharon, A.A.; Nehama, H.; Rishpon, S.; Baron-Epel, O. Parents with high levels of communicative and critical health literacy are less likely to vaccinate their children. Patient Educ. Couns. 2017, 100, 768–775. [Google Scholar] [CrossRef]
- Graham, S.P.; Prapavessis, H.; Cameron, L.D. Colon cancer information as a source of exercise motivation. Psychol. Health 2006, 21, 739–755. [Google Scholar] [CrossRef]
- Dumitrescu, A.L.; Wagle, M.; Dogaru, B.C.; Manolescu, B. Modeling the theory of planned behavior for intention to improve oral health behaviors: The impact of attitudes, knowledge, and current behavior. J. Oral Sci. 2011, 53, 369–377. [Google Scholar] [CrossRef] [Green Version]
- Bian, J.; Guo, Y.; He, Z.; Hu, X. Social Web and Health Research: Benefits, Limitations, and Best Practices; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Rossi, P. Marketing at the Confluence Between Entertainment and Analytics: Proceedings of the 2016 Academy of Marketing Science (AMS) World Marketing Congress; Springer: Lille, France, 2017. [Google Scholar]
- Matthieu, D. Online Panels China: QQ Survey, So Jump and Diaochapai. Available online: https://daxueconsulting.com/online-panels-china/ (accessed on 17 April 2020).
- Kamal-Chaoui, L.; Leeman, E.; Rufei, Z. Urban Trends and Policy in China. Available online: http://www.oecd.org/governance/regional-policy/42607972.pdf (accessed on 8 April 2020).
- Krechetova, V. Economic and cultural complexes of China. Cybergeo Eur. J. Geogr. 2011. [Google Scholar] [CrossRef]
- Fang, L.; Wang, Y. Multi-disciplinary determination of the rural/urban boundary: A case study in Xi’an, China. Sustainability 2018, 10, 2632. [Google Scholar] [CrossRef] [Green Version]
- WHO Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 8 April 2020).
- China CDC COVID-19 Preventive and Control. Available online: www.chinacdc.cn/en/COVID19/202002/P020200310326809462942.pdf (accessed on 8 April 2020).
- Criss, S.; Baidal, J.A.W.; Goldman, R.E.; Perkins, M.; Cunningham, C.; Taveras, E.M. The role of health information sources in decision-making among Hispanic mothers during their children’s first 1000 days of life. Matern. Child Health J. 2015, 19, 2536–2543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.J.; Rickard, L.N.; Harrison, T.M.; Seo, M. Applying the risk information seeking and processing model to examine support for climate change mitigation policy. Sci. Commun. 2014, 36, 296–324. [Google Scholar] [CrossRef]
- Kahlor, L.A. An augmented risk information seeking model: The case of global warming. Media Psychol. 2007, 10, 414–435. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Zimmerman, R.K.; Santibanez, T.A.; Janosky, J.E.; Fine, M.J.; Raymund, M.; Wilson, S.A.; Bardella, I.J.; Medsger, A.R.; Nowalk, M.P. What affects influenza vaccination rates among older patients? An analysis from inner-city, suburban, rural, and Veterans Affairs practices. Am. J. Med. 2003, 114, 31–38. [Google Scholar] [CrossRef]
- Sherman, A. Determinants of mammography use in rural and urban regions of Canada. Can. J. Rural Med. 2010, 15, 52–60. [Google Scholar]
- Bryant, H.; Mah, Z. Breast cancer screening attitudes and behaviors of rural and urban women. Prev. Med. 1992, 21, 405–418. [Google Scholar] [CrossRef]
- Yang, Z.J.; Ho, S.S.; Lwin, M.O. Promoting preventive behaviors against influenza: Comparison between developing and developed countries. Asian J. Commun. 2014, 24, 567–588. [Google Scholar] [CrossRef]
- Rimer, B.K.; Kreuter, M.W. Advancing tailored health communication: A persuasion and message effects perspective. J. Commun. 2006, 56, S184–S201. [Google Scholar] [CrossRef]
- Cutter, S.L.; Ash, K.D.; Emrich, C.T. Urban-rural differences in disaster resilience. Ann. Am. Assoc. Geogr. 2016, 106, 1236–1252. [Google Scholar] [CrossRef]
- Anton, C.E.; Lawrence, C. Home is where the heart is: The effect of place of residence on place attachment and community participation. J. Environ. Psychol. 2014, 40, 451–461. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Luo, D.; Sun, W.; Yan, T.; Hu, D.; Pan, W.; Luo, A. Health information literacy and barriers of online health information seeking among digital immigrants in rural China: A preliminary survey. SAGE Open 2019, 9. [Google Scholar] [CrossRef]
- Everett, C.M.; Schumacher, J.R.; Wright, A.; Smith, M.A. Physician assistants and nurse practitioners as a usual source of care. J. Rural Health 2009, 25, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Federal Emergency Management Agency Coronavirus Rumor Control. Available online: https://www.fema.gov/coronavirus/rumor-control (accessed on 29 April 2020).
- Southwell, B.G.; Niederdeppe, J.; Cappella, J.N.; Gaysynsky, A.; Kelley, D.E.; Oh, A.; Peterson, E.B.; Chou, W.-Y.S. Misinformation as a misunderstood challenge to public health. Am. J. Prev. Med. 2019, 57, 282–285. [Google Scholar] [CrossRef]
- Chen, X.; Hay, J.L.; Waters, E.A.; Kiviniemi, M.T.; Biddle, C.; Schofield, E.; Li, Y.; Kaphingst, K.; Orom, H. Health literacy and use and trust in health information. J. Health Commun. 2018, 23, 724–734. [Google Scholar] [CrossRef]
- Paige, S.R.; Krieger, J.L.; Stellefson, M.L. The influence of eHealth literacy on perceived trust in online health communication channels and sources. J. Health Commun. 2017, 22, 53–65. [Google Scholar] [CrossRef] [Green Version]
- McGarrity, L.A.; Huebner, D.M. Behavioral intentions to HIV test and subsequent testing: The moderating role of sociodemographic characteristics. Health Psychol. 2014, 33, 396–400. [Google Scholar] [CrossRef]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic disparities in health behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Li, X.; Xue, J. Education inequality between rural and urban areas of the People’s Republic of China, migrants’ children education, and some implications. Asian Dev. Rev. 2015, 32, 196–224. [Google Scholar] [CrossRef]


{kind=link}
| Rural Status | Age | Sex | Education | Income | |
|---|---|---|---|---|---|
| Preventive behaviors | −0.07 * | 0.01 ** | 0.03 | 0.02 | 0.01 * |
| Behavioral intention | −0.10 | 0.01 ** | 0.01 | 0.03 | 0.02 |
| Attitude | −0.18 * | 0.01 ** | 0.02 | −0.03 | 0.03 * |
| Subjective norms | −0.02 | −0.00 | 0.04 | 0.02 | 0.01 |
| Knowledge | −0.06 | −0.00 | 0.00 | 0.07 ** | 0.04 ** |
| Interpersonal source variety | 0.05 | 0.01 * | 0.03 | 0.13 ** | 0.03 |
| Media source variety | −0.03 | −0.00 | 0.10 | −0.01 | −0.04 |
| Information appraisal | −0.10 * | 0.00 | 0.04 | 0.05 ** | 0.02 * |
| Independent Variable | b | SE | 95% CI | p | |
|---|---|---|---|---|---|
| Direct Effect | |||||
| Preventive behaviors | Rural status | −0.04 | 0.03 | −0.10, 0.02 | 0.178 |
| Attitude | 0.05 | 0.01 | 0.03, 0.07 | <0.001 ** | |
| Intention | 0.08 | 0.02 | 0.05, 0.11 | <0.001 ** | |
| Subjective norms | 0.11 | 0.02 | 0.08, 0.14 | <0.001 ** | |
| Information appraisal | 0.13 | 0.02 | 0.10, 0.17 | <0.001 ** | |
| Intention | Attitude | 0.05 | 0.01 | 0.02, 0.08 | <0.001 ** |
| Subjective norms | 0.24 | 0.02 | 0.19, 0.28 | <0.001 ** | |
| Information appraisal | 0.27 | 0.03 | 0.22, 0.32 | <0.001 ** | |
| Attitude | Rural status | −0.14 | 0.08 | −0.29, 0.02 | 0.083 |
| Information appraisal | 0.45 | 0.04 | 0.36, 0.53 | <0.001 ** | |
| Subject norms | Information appraisal | 0.29 | 0.03 | 0.23, 0.34 | <0.001 ** |
| Information appraisal | Rural status | −0.10 | 0.05 | −0.19, −0.01 | 0.028 * |
| Indirect Effect | |||||
| Preventive behaviors | Rural status | −0.03 | 0.01 | −0.05, −0.01 | 0.008 ** |
| Information appraisal | 0.08 | 0.01 | 0.07, 0.10 | <.001 ** | |
| Attitude | 0.004 | 0.001 | 0.001, 0.007 | 0.004 ** | |
| Subjective norms | 0.02 | 0.004 | 0.01, 0.03 | <.001 ** | |
| Intention | Rural status | −0.04 | 0.02 | −0.08, −0.01 | 0.012 * |
| Information appraisal | 0.09 | 0.01 | 0.07, 0.11 | <0.001 ** | |
| Attitude | Rural status | −0.04 | 0.02 | −0.09, −0.00 | 0.032 * |
| Subjective norms | Rural status | −0.03 | 0.01 | −0.05, −0.00 | 0.031 * |
| Total Effect | |||||
| Preventive behaviors | Rural status | −0.07 | 0.03 | −0.13, −0.01 | 0.029 * |
| Attitude | 0.06 | 0.01 | 0.04, 0.08 | <0.001 ** | |
| Intention | 0.08 | 0.02 | 0.05, 0.11 | <0.001 ** | |
| Subjective norms | 0.13 | 0.02 | 0.10, 0.16 | <0.001 ** | |
| Information appraisal | 0.22 | 0.02 | 0.18, 0.25 | <0.001 ** | |
| Intention | Rural status | −0.04 | 0.02 | −0.08, −0.01 | 0.012 * |
| Information appraisal | 0.36 | 0.03 | 0.31, 0.41 | <0.001 ** | |
| Attitude | 0.05 | 0.01 | 0.02, 0.08 | <0.001 ** | |
| Subjective norms | 0.24 | 0.02 | 0.19, 0.28 | <0.001 ** | |
| Attitude | Rural status | −0.18 | 0.08 | −0.34, −0.02 | 0.026 * |
| Information appraisal | 0.45 | 0.04 | 0.36, 0.53 | <0.001 ** | |
| Subjective norms | Rural status | −0.03 | 0.01 | −0.05, −0.00 | 0.031 * |
| Information appraisal | 0.29 | 0.03 | 0.23, 0.34 | <0.001 ** | |
| Information appraisal | Rural status | −0.10 | 0.05 | −0.19, −0.01 | 0.028 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Chen, H. Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. Int. J. Environ. Res. Public Health 2020, 17, 4437. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124437
Chen X, Chen H. Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. International Journal of Environmental Research and Public Health. 2020; 17(12):4437. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124437
Chicago/Turabian StyleChen, Xuewei, and Hongliang Chen. 2020. "Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China" International Journal of Environmental Research and Public Health 17, no. 12: 4437. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124437