1. Introduction
Achilles tendon ruptures (ATR) are common injuries among adults and have compounding long-term effects. Over the past 30 years, the incidence of ATR has been increasing from 2 to 22 per 100,000 people per year, primarily in the athletic population [
1]. ATR is more common in males than in females with the ratio being quoted at 5:1 [
2]. Tendons are not contractile tissues, and as such cannot provide the necessary positive work to drive human motion. Evidence has been reported that ATR will cause persistent tendon elongation and is associated with biomechanical deficits such as decreased plantar flexor muscle strength/volume, decreased ankle joint proprioception and reduced AT stiffness [
3,
4].
These functional deficits are reported regardless of the medical efforts and treatment modality for both short-term and long-term outcomes [
5,
6]. The elongated tendon combined with decreased muscle force and tendon stiffness has been shown to have a substantially decreased running and jumping performance, and also has implications for daily functional activities such as normal gait and walking on stairs [
7]. The alterations in calf muscle anatomical, mechanical and neuromuscular properties after ATR may increase plantar flexor muscle activity during movement, leading to AT weakness in a plantarflexed position and reduce plantar flexor endurance [
8].
The rupture injury mechanism of ATR can be attributed to sudden unexpected powerful dorsiflexion of the ankle joint or forced dorsiflexion of the plantarflexed ankle joint [
9]. A case study reported that long-term functional deficits after ATR could be explained by permanent reductions in gastrocnemius muscle fascicle length [
10]. The muscle-tendon structure is detrimentally affected following ATR and the calf muscle strength deficits are positively correlated with the fascicle length reduction magnitude [
11]. The atrophy and eccentric strength impairment of calf muscles were still present after 24 months of ATR, which brings adaptive modifications in gait strategy involving ankle motion and coordinated muscular activities [
12]. The landing pattern (rearfoot strike vs. non-rearfoot strike) also has an impact on the Achilles tendon loading and a previous study found that people with a non-rearfoot strike running pattern experienced nearly 11% greater Achilles tendon impulse during each step [
13]. To further improve treatment, rehabilitation, and enhancing the understanding of the long-term outcome, it is important to understand the underlying mechanisms for musculoskeletal deficits.
Biomechanical analysis is always carried out using experimental or computational methods. The traditional biomechanical analysis based on laboratory experiments has two inadequacies: (1) a lot of important information, including muscle forces, is difficult to measure in the laboratory; (2) separate laboratory data proves difficult to build a relationship with complex human dynamic systems. OpenSim is an open-source software package developed for musculoskeletal model building simulation, and analysis without surgically-invasive procedures [
14]. In silico OpenSim models provide a modeling environment for identifying individual variables (kinematics, kinetics, muscle-tendon parameters) and predict muscle force contributions and joint contact loads during walking and running [
15].
Extensive research has developed “generic” lower limb musculoskeletal models using cadaveric data. Medical images (ultrasound, computed tomography, magnetic resonance imaging, etc.,) may help generate a high level of anatomical personalization for creating image-based subject-specific musculoskeletal models [
16]. Several studies using image-based subject-specific models have been created to estimate knee/tibiofemoral articular forces. The comparison of generic and subject-specific models have also been shown to be more accurate in the assessment of knee joint contact force using subject-specific anatomical parameters [
17,
18]. To date, few studies have investigated the rupture-repaired Achilles tendon (AT) subject-specific model for estimating muscle forces and joint articular forces. The identification of muscle-tendon parameters, i.e., tendon slack length lst and optimal fiber length lom should be critical aspects when creating subject-specific musculoskeletal models. This is important due to the sensitivity of muscle estimated forces to the muscle-tendon complex moment arms [
19].
Based on our prior study, gait asymmetry exists among participants of unilateral Achilles tendon rupture after surgical repair [
20]. However, only limited information about how the muscular contribution to walking and running tasks were reported. This study aims to: (a) Build dynamic subject-specific rupture-repaired AT lower limb musculoskeletal models based on ultrasound medical imaging and motion capture data; (b) Compare lower extremity joint angles, moments, quadriceps femoris and triceps surae muscle forces and joint reaction forces between inter-limb (involved vs. uninvolved side) of unilateral rupture-repaired AT patients at two years after surgery during normal walking, jogging and running. It was hypothesized that the gastrocnemii and soleus AT lengths of the involved side will be significantly longer than the uninvolved side. It was further anticipated that the additional slack of the tendon will reduce force transmission across the joint, thus the muscle forces will compensate any increases while the joint reaction forces will decrease.
4. Discussion
This study integrates an in vivo gait analysis, ultrasound imaging based subject-specific AT repaired lower limb musculoskeletal model to investigate if geometry modification of the AT was present after 2 years operative treatment of the unilateral ATR. The study also investigated if as a consequence, lower limb kinematics, kinetics, and muscular contributions were different between the involved and uninvolved legs. In the current study, the mean ATRS value (83.7) of these patients reported fairly normal physical activity and function and recovered well after two years ATR [
21]. As hypothesized, a discrepancy was found between the patient-reported outcomes and the tests, which showed large impairment and significant functional deficits with an elongated AT persisting on the injured side in patients with a surgically repaired Achilles tendon at two years. The previous findings showed higher AT length 2–6 years after surgical repair on the previously injured leg, which supports our first hypothesis [
34].
Gait analysis has been used to identify intrinsic gait-related risk factors, which revealed altered ankle joint sagittal plane kinematics and plantarflexion moments compared to the uninjured side [
35]. Increased ankle dorsiflexion was accompanied by decreased plantarflexion and was observed almost during the whole stance phase of walking, jogging and running movements. This has also been found in previous studies [
4,
36]. It has been suggested that increased ankle dorsiflexion may reveal a sustained eccentric dynamic control deficit even 4.5 years after an ATR [
37]. An association between increased ankle dorsiflexion and consistent ankle plantar flexor eccentric contraction deficits two years after an ATR was also reported [
38]. The plantarflexion moment of the involved limb was lower during the mid-stance phase of jogging and running. The intra-patient AT length and stiffness asymmetries were found related to deficits in plantarflexion moments during gait in a previous study [
34]. While this study failed to find any difference between the involved and uninvolved sides during normal walking. This discrepancy in such results could be attributed to the physical activity level and follow-up time in this study.
Willy et al., suggested that the side to side deficits and discrepancies were larger in ATR patients with high-demand and higher angular velocity activities, i.e., jogging and hopping compared with walking [
39]. The decreased plantarflexion angle during the push-off phase in jogging and running movements of the injured leg suggested decreased triceps surae contribution in the center of mass displacement during locomotion [
40]. The ankle joint kinematic and kinetic data obtained in this study suggest that the ankle plantar flexor function is more impaired during higher-demand movements and higher end-range ankle joint plantarflexion after an ATR. A previous study showed the plantar flexor muscles suffered from a functional deficit in patients with an ATR even more than two years after surgery [
9]. It was speculated that the increased ankle dorsiflexion degree accompanied by a decreased plantar flexion moment may be a compensatory mechanism of insufficient ankle dorsal flexor function and the anomalous co-contraction of tibialis anterior and calf muscles, which has been confirmed in previous gait analysis with 41 ATR patients one year after surgery [
41].
As hypothesized, the joint reaction forces will decrease, while the results of this study do not support this hypothesis. While this study found that increased knee joint loading associated with decreased ankle joint function was present in patients two years after an ATR. It was reported that if the AT length of the involved side increased, the muscle fascicle length will decrease by an equal amount [
8]. The AT is not a contractile tissue compared to muscle and can’t provide positive work to produce human motion. Thus the shorter triceps surae fascicles in the involved limb may promote a deficit in plantar flexor power generation [
42]. The compromised plantar flexor function of the injured leg following an ATR may compensate by increased work done by the ipsilateral knee joint [
43]. In this study, increased knee extension angles and elevated knee joint moments were found in the involved limb during all activities. Furthermore, increased knee joint contact forces were also present during walking, jogging and running except in the mid-stance phase of running movements. This study showed increased knee extension in the involved limb during initial contact and push-off phases of the jogging and mid-stance phase of running. The increased knee extension during jogging and running maybe a potential regulatory mechanism to ensure sufficient elongated triceps surae complex tension [
44]. A previous study supports the findings of this study, which found a compensation mechanism of the overextension knee joint during running against the AT elongation and deficit of gastro-soleus muscle-tendon complex [
10]. The calf muscle crosses two joints, which play an important role to prevent knee overextension and anterior knee laxity as a stabilizer. Thus the deficit and weakness of the calf muscle in the involved limb may place the knee in an overextension position and at risk for further injury [
45]. It was found that the hip joint was more flexed during the push-off phase of jogging and running, which may be a compensation mechanism following overextension of the knee joint to prevent injury risk during high-demand tasks.
The resultant pattern of greater knee extension moment and knee joint contact forces in the involved limb may result in an overloaded knee extensor mechanism. The increased knee joint loading may be attributed to weakened ankle plantar flexor function and elongation of the AT during higher demand tasks like jogging, running and even basic locomotion like walking. The findings of this study were inconsistent with earlier works that showed significantly greater patellofemoral joint loading in the injured leg only during high-demand activities but not during walking in patients after surgical ATR repair [
41,
43]. The reason for the inconsistency may be due to the different physical activity levels and follow-up time of the subjects. The average ATRS value of the previous study is 87.0 compared with 83.7 in this study, and the follow-up time of the previous study was 6.2 years on average compared to two years in our study. Probably, the AT of the patients in this study were still in the remodeling stage and the symptoms and functions will reach a plateau two years after ATR [
46]. The greater knee/patellofemoral joint loading was reported positively correlated with patellofemoral pain and even knee osteoarthritis in previous studies [
47,
48]. Further study should assess the knee symptoms in patients recovering from an ATR.
In the frontal plane, the subtalar joint angle and moment patterns were also changed between the involved and uninvolved sides. During jogging and running, the ankle joint was found more everted combined with greater subtalar eversion moment during almost the whole stance phase. The ankle joint over-eversion was observed associated with several running-related injuries, including medial tibial stress syndrome and more knee injuries [
49]. The deficit of plantar flexor muscle operation in the sagittal plane may be substituted by increased loading in the frontal plane of the lower limb joints [
50]. Consistently, Jandacka et al. reported that a weakened and elongated AT may be the main reason causing altered sagittal plane knee and ankle joint kinematics and increasing lower extremity frontal-plane loading as a consequence [
43].
To the extent of our knowledge, this is the first study to investigate the side-to-side muscular contribution during normal activities via subject-specific OpenSim musculoskeletal modeling after a unilateral ATR. The knee extension femur muscle strength was found conversely increased during jogging and running. While during walking, only the rectus femoris force was found higher in the involved side during the push-off phase, the vas_med, vas_lat and vas_inter forces were still showed deficits in the involved side. In accordance with the present results, which have demonstrated that significantly greater knee joint power was observed in the involved side as compensation for reduced plantar flexor function during high-demand activities only but was not observed during walking [
51]. The greater knee extension muscular forces in the involved side in this study were also following a higher knee extension degree and moments during jogging and running.
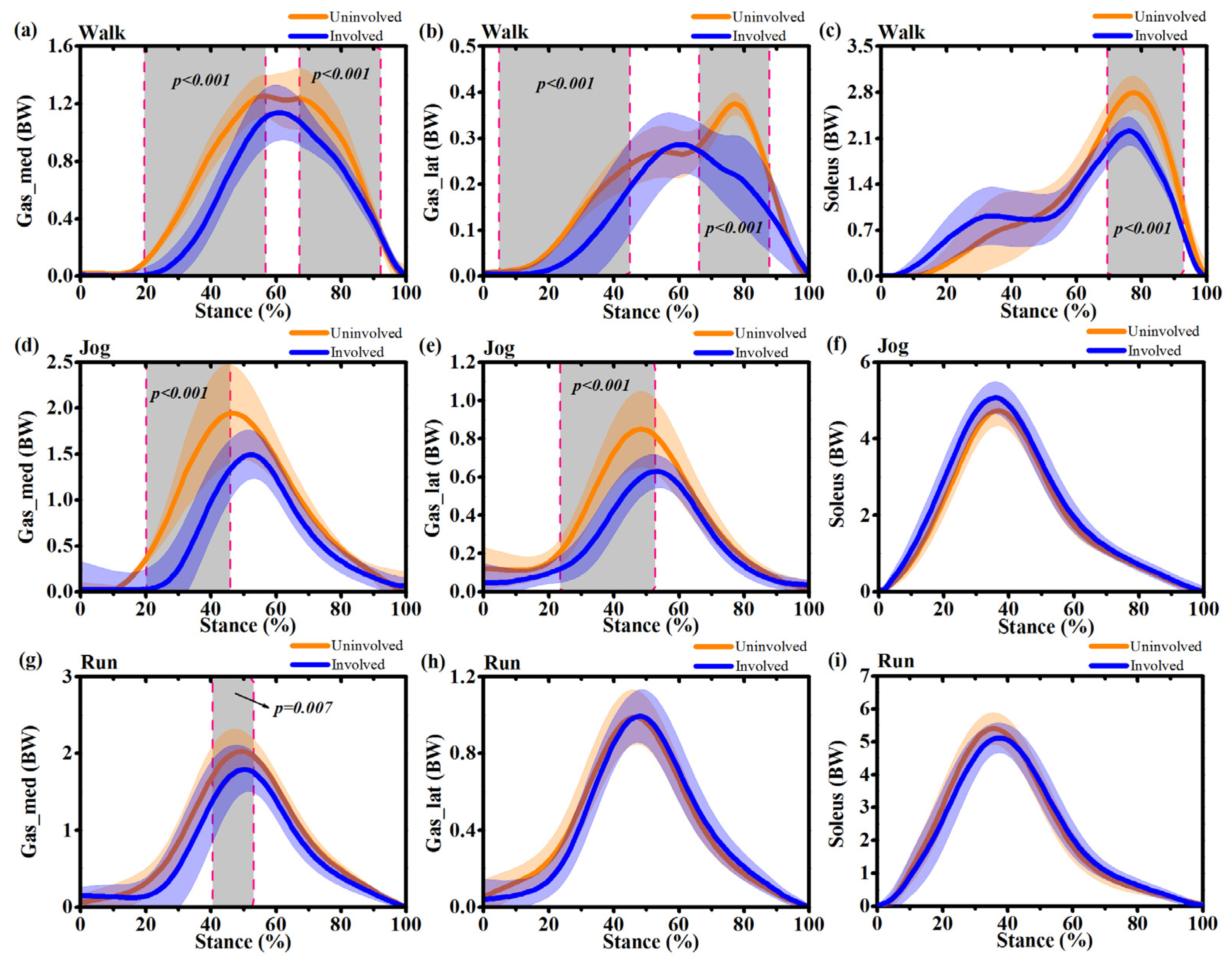
In the present study, it was found that significant lower limb muscle strength deficits during normal movements persist on the injured side two years after an acute ATR. The gastrocnemius and soleus muscle forces were found significantly decreased in the involved side during the stance phase of walking, jogging and running. Thus, the results do not support the hypothesis of the triceps surae muscle forces will increase to compensate for the additional slack length and decreased force transmission capacity of the AT.
There are several possible explanations for this result. The first interpretation was that with the elongated AT in the involved side, the shank muscles are atrophied, the AT properties may tend to more compliant and hysteresis, which may hurt the stretch-shortening cycle and muscle-tendon interaction during the stance phase of the involved limb [
52,
53,
54]. The second interpretation was when the ankle joint in plantar flexion position during the push-off phase, the triceps surae muscle was in a shortened posture and below the optimal angle for force generatio. These findings are in accordance with a study that reported the additional slack of the AT may lead to decreased plantarflexion strength [
5]. The weakened plantar flexor muscles on the involved side and asymmetry may overload the muscle-tendon complex in the uninvolved side. Furthermore, the plantar flexor muscle deficit may affect the mediolateral acceleration of the center of mass based on a previous study and thus disturb the frontal plane ankle stability of the injured side. This may be an additional explanation for the increased ankle joint eversion in the involved side in this study. The increased AT length and decreased triceps surae strength to stretch the AT indicate that the functional deficit in the involved side may be primarily caused by anatomical alterations of the tendon. Thus, the calf muscle asthenia may be due to inefficacies in force transmission capacity across the joint.
Several limitations should not be ignored in the current study. The first limitation relates to the small sample size in this study. However, we have still observed significant musculoskeletal abnormalities between the involved and uninvolved sides in patients recovering from an ATR. The second limitation was the lack of a healthy control group and to assess inter-limb differences, while an inter-limb gait function test may be a conservative assessment after an ATR. The third limitation of this study was that the movement speed (about 3.5 m/s during running) during testing in the laboratory was relatively slow compared to the real outdoor activities. The ATR mostly occurred during a rapid plantar flexor eccentric loading phase. Thus, further studies should investigate lower limb musculoskeletal functional differences during high-intensity movements like cutting and landing in both ATR patients and uninjured subjects.


 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}