Process Evaluation of a School-Based Program Aimed at Preventing Obesity in Adolescents from Lima and Callao, Peru


Abstract
:1. Introduction
2. Materials and Methods
2.1. Outline of the Overall Research Project—The “Health Promoting Schools” Study Design
2.2. The HPS Obesity Prevention Program, Components, and Planned Delivery
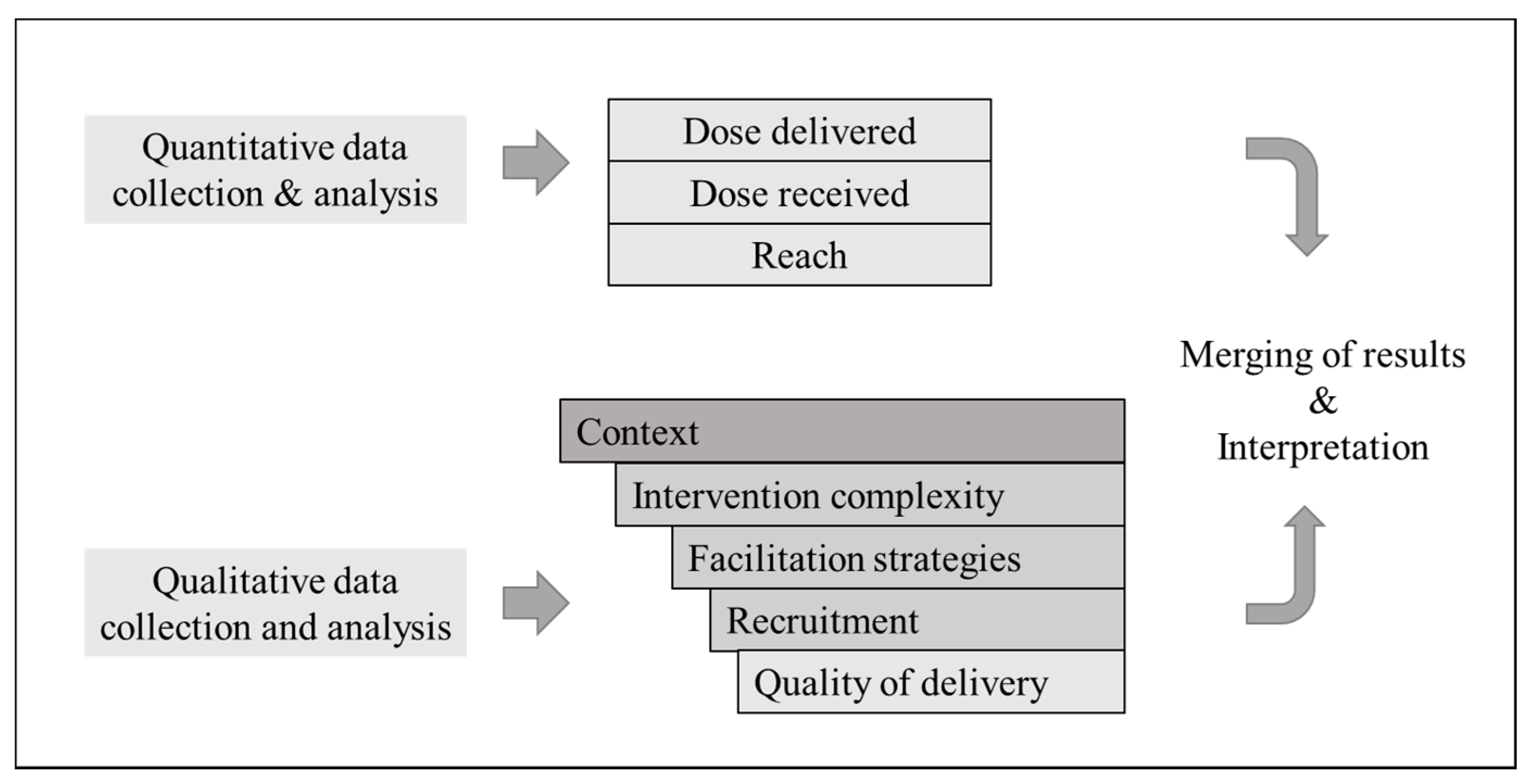
2.3. Description of the Process Evaluation Model
2.4. Data Collection and Measures
2.4.1. Quantitative Data and Measurement of Process Outcomes
2.4.2. Qualitative Data and Measurement of Factors Influencing the Program Implementation
2.5. Data Analyzes
2.5.1. Analysis of Quantitative Data
2.5.2. Analysis of Qualitative Data
2.6. Ethical Approval
3. Results
3.1. Program Delivery: Dose Delivered of Education Sessions for Students and Other Target Groups and the Influence of Intervention Complexity, Facilitation Strategies, and Context
3.2. Program Delivery: Dose Delivered of Other Environmental Activities
3.3. Program Reach: Education and Environmental Activities and the Influence of Recruitment Strategies and Context
3.4. Program Delivery: Dose Received by Satisfaction of Participants with Selected Program Activities
4. Discussion
4.1. The Challenge of Being Part of a Wider ODA Health Promotion Intervention
4.2. The Need to Establish Better Facilitation and Recruitment Strategies
4.3. The Need to Assess and Monitor Contextual Influences before and during Implementation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saunders, R.P.; Evans, M.H.; Joshi, P. Developing a process-evaluation plan for assessing health promotion program implementation: A how-to guide. Health Promot. Pract. 2005, 6, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Steckler, A.B.; Linnan, L.; Israel, B. Process Evaluation for Public Health Interventions and Research; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 1–23. [Google Scholar]
- McGraw, S.A.; Sellers, D.; Stone, E.; Resnicow, K.A.; Kuester, S.; Fridinger, F.; Wechsler, H. Measuring implementation of school programs and policies to promote healthy eating and physical activity among youth. Prev. Med. 2000, 31, S86–S97. [Google Scholar] [CrossRef]
- Bowie, L.; Bronte-Tinkew, J. Process Evaluations: A Guide for Out-of-School Time Practitioners; Child Trends: Washington, DC, USA, 2008; pp. 1–8. [Google Scholar]
- Chinman, M.; Imm, P.; Wandersman, A.; Kaftarian, S.; Neal, J.; Pendleton, K.T.; Ringwalt, C. Using the getting to outcomes (GTO) model in a statewide prevention initiative. Health Promot. Pract. 2001, 2, 302–309. [Google Scholar] [CrossRef]
- Carroll, C.; Patterson, M.; Wood, S.; Booth, A.; Rick, J.; Balain, S. A conceptual framework for implementation fidelity. Implement. Sci. 2007, 2, 40. [Google Scholar] [CrossRef] [Green Version]
- Hasson, H. Systematic evaluation of implementation fidelity of complex interventions in health and social care. Implement. Sci. 2010, 5, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaker, S.; Steckler, A.; Sánchez, V.; Khatapoush, S.; Rose, J.; Hallfors, D.D. Program characteristics and organizational factors affecting the implementation of a school-based indicated prevention program. Health Educat. Res. 2008, 23, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Wierenga, D.; Engbers, L.H.; Van Empelen, P.; Duijts, S.; Hildebrandt, V.H.; Van Mechelen, W. What is actually measured in process evaluations for worksite health promotion programs: A systematic review. BMC Public Health 2013, 13, 1190. [Google Scholar] [CrossRef] [Green Version]
- Brouwer, W.; Kroeze, W.; Crutzen, R.; de Nooijer, J.; de Vries, N.K.; Brug, J.; Oenema, A. Which intervention characteristics are related to more exposure to internet-delivered healthy lifestyle promotion interventions? A systematic review. J. Med. Internet Res. 2011, 13, e2. [Google Scholar] [CrossRef]
- Gentile, D.A.; Welk, G.; Eisenmann, J.C.; Reimer, R.A.; Walsh, D.A.; Russell, D.W.; Fritz, K. Evaluation of a multiple ecological level child obesity prevention program: Switch® what you Do, View, and Chew. BMC Med. 2009, 7, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, T.L.; Pallan, M.J.; Clarke, J.L.; Lancashire, E.R.; Lyon, A.; Parry, J.M.; Adab, P. Process evaluation design in a cluster randomised controlled childhood obesity prevention trial: The WAVES study. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 112. [Google Scholar] [CrossRef] [Green Version]
- Robbins, L.B.; Pfeiffer, K.A.; Wesolek, S.M.; Lo, Y.J. Process evaluation for a school-based physical activity intervention for 6th-and 7th-grade boys: Reach, dose, and fidelity. Eval. Progr. Plan. 2014, 42, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, K.A.; Naughton, G.; Benson, A.C. The GLAMA (Girls! Lead! Achieve! Mentor! Activate!) physical activity and peer leadership intervention pilot project: A process evaluation using the RE-AIM framework. BMC Public Health 2012, 12, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turunen, H.; Sormunen, M.; Jourdan, D.; Von Seelen, J.; Buijs, G. Health promoting schools—A complex approach and a major means to health improvement. Health Promot. Int. 2017, 32, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs—Principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritchie, J.; Spencer, L. Qualitative data analysis for applied policy research. In Analysing Qualitative Data; Bryman, A., Burgess, R.G., Eds.; Routledge: London, UK, 1994; pp. 173–194. [Google Scholar]
- Smith, J.; Firth, J. Qualitative data analysis: The framework approach. Nurse Res. 2011, 18, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [Green Version]
- Hahn, E.J.; Noland, M.P.; Rayens, M.K.; Christie, D.M. Efficacy of training and fidelity of implementation of the life skills training program. J. Sch. Health 2002, 72, 282–287. [Google Scholar] [CrossRef] [PubMed]
- De Meij, J.S.; Chinapaw, M.J.; Kremers, S.P.; Jurg, M.E.; Van Mechelen, W. Promoting physical activity in children: The stepwise development of the primary school-based JUMP-In intervention applying the RE-AIM evaluation framework. Br. J. Sportsmed. 2010, 44, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Baird, J. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solberg, L.I.; Brekke, M.L.; Fazio, C.J.; Fowles, J.; Jacobsen, D.N.; Kottke, T.E.; Rolnick, S.J. Lessons from experienced guideline implementers: Attend to many factors and use multiple strategies. Joint Com. J. Qual. Improv. 2000, 26, 171–188. [Google Scholar] [CrossRef]
- Elinder, L.S.; Heinemans, N.; Hagberg, J.; Quetel, A.K.; Hagströmer, M. A participatory and capacity-building approach to healthy eating and physical activity–SCIP-school: A 2-year controlled trial. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cargo, M.; Salsberg, J.; Delormier, T.; Desrosiers, S.; Macaulay, A.C. Understanding the social context of school health promotion program implementation. Health Educ. 2006, 106, 85–97. [Google Scholar] [CrossRef]
- MacDonald, M.A.; Green, L.W. Reconciling concept and context: The dilemma of implementation in school-based health promotion. Health Educ. Behav. 2001, 28, 749–768. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inputs | Materials | Immediate Impacts | Short-Term Impacts | Behavioral Impacts | Health Outcomes |
|---|---|---|---|---|---|
| Providing education sessions and carrying out environmental activities targeting students and other members of school community | Year action plans, nutrition and PA curriculum, exhibition stands, nutrition traffic lights, leaflets, banners, minigym, sports equipment, program souvenirs | Participants increased awareness of the importance of a healthy diet and the practice of PA | Development of students’ skills for consuming healthy food, abstaining from unhealthy food options and engage in more PA, parent, teacher and peer support of healthy diet and PA behaviors, food availability at school kiosk | Increased/reduced intake of healthy/unhealthy food and increased participation in PA | Prevent the development of obesity, and thus, improve the physical health status of students |
| Component | Years | Details | Dose |
|---|---|---|---|
| 1. Education program for students | 2015 | Sessions on two modules–Nutrition (5 subjects) and PA (1 subject) to be delivered by implementer nurse in each intervention school throughout the school year. | 1 weekly 50 min to 1.5 h session (6-week period) |
| 2016–2017 | Reinforcement sessions on two modules–Nutrition (3 subjects) and PA (1 subject) delivered by the nurse. | 1 weekly 50 min to 1.5 h session (4-week period) | |
| 2. Environmental component | |||
| 2.1 Parents’ education | 2015–2016 | Sessions on nutrition (2 subjects) and PA (1 subject) per school year delivered by the nurse using open discussion and teamwork. | 1 monthly 45 min to 1 h sessions (3-month period) |
| 2.2 Teachers’ education | 2015 | Introductory session on program, nutrition and PA subjects. Objective was to create awareness of program, specific activities in each school, and encourage support in activities and normal class hours. | 1 time 2 h session |
| 2016–2017 | Capacity-building training on health promotion, including nutrition and PA subjects designed to be delivered each year. Training was scheduled to be carried out by a local University. | 1 weekly 6-h session (4-month period) | |
| 2.3 Junior Health Promoters (JHP) | 2015–2017 | Selection of three students per classroom per school and provision of education sessions by nurse on nutrition (3 subjects) and PA (1 subject). Aim was to support healthy behaviors and motivate the participation and interest of students in program activities. | 45 min sessions |
| 2.4 Healthy Food Kiosk Initiative (Education sessions) | 2015 | Sessions on 7 nutrition subjects to be delivered by implementer nurse to the staff throughout the school year | 30 min sessions |
| 2016–2017 | Sessions on 4 nutrition subjects to be delivered by health center nurse. | 30 min sessions | |
| 2.5 Healthy Food Kiosk Initiative (Physical Improvement & Evaluation) | 2015–2017 | Physical improvement to consist of installation of 1 fruit exhibition stand and 3 nutrition traffic lights per school kiosk during program implementation span. | 4 units in total |
| 2015–2017 | 2-year evaluations of kiosks to verify the availability of healthy food options, sanitation, healthy practices, infrastructure, etc. Specific formats to be used were not established. | 2 times per school year | |
| 2.6 Improve school physical environment | 2015 | Installation of leaflets wall board units per school to exhibit leaflets including those of nutrition and PA subjects; installation of a mini gym unit per school (set of parallel bars, pull-ups bars, and abdominal benches) to promote the practice of PA during and after class hours. | 2 wall board units 1 minigym unit |
| 2.7 PA events | 2015–2017 | Yearly walking event following a prior coordinated route carrying banners promoting healthy nutrition and PA in the community. The event was scheduled to have the participation of the entire school community (students, parents, teachers, school administration staff) in addition to program staff and guests. | 1 time 2-h event |
| 2015–2017 | Sports Olympics to be carried out at each school during the last quarter of school year, designed to include sports competitions (volleyball, football, athletics and/or basketball or other) encouraging the wide participation of all students in each school. | 1 time full-school day event | |
| 2.8 Dissemination of nutrition and PA-related information | 2015–2017 | Disseminate a specific number of leaflets and posters on nutrition and PA subjects developed by the implementation team per year. | 600–1000 leaflets per school (2015) 500 leaflets per school (2016–2017) 50 posters per school (2015–2017) |
| Dimension | Component | Data Collection Instruments | Data Sources | Total Number Collected | Frequency of Measurement |
|---|---|---|---|---|---|
| Dose delivered | Education program | Self-administered form | Implementation Team | 304 | Weekly |
| Environmental activities | Self-administered form | Implementation Team | 228 | Weekly | |
| Kiosk evaluation reports | Implementation Team | 12 | At each kiosk evaluation | ||
| Dose received | Education program | Satisfaction scales | Students | - | End of school year follow-up |
| Individual interviews | Students | 8 | Post-intervention | ||
| Environmental activities | Satisfaction scales | Teachers | - | After training completed | |
| Individual interviews | Parents, teachers | 16 | Post-intervention | ||
| Reach | Education program | Self-administered form | Implementation Team | 304 | Weekly |
| Environmental activities | Self-administered form | Implementation Team | 16 | Weekly | |
| Context | Both | Logbooks | Implementation team | 105 | Weekly |
| E-mails | Design, monitoring & implementation team, school directors, teachers | 248 | During program implementation | ||
| Meeting minutes | Design team, implementation team | 30 | At each meeting | ||
| Individual interviews | Parents, teachers, implementation team, Peru official | 23 | Post-intervention | ||
| Intervention complexity | Both | Year action plans | Design team | 12 | Before start of school year |
| Individual interviews | Teachers, implementers | 14 | Post-intervention | ||
| Facilitation strategies | Both | Year action plans | Design team | 12 | Before start of school year |
| Logbooks | Implementation team | 105 | Weekly | ||
| E-mails | Design, monitoring & implementation team | 124 | During program implementation | ||
| Individual interviews | Implementers | 6 | Post-intervention | ||
| Recruitment | Both | Year action plans | Design team | 12 | Before start of school year |
| Logbooks | Implementation team | 105 | Weekly | ||
| E-mails | Design, monitoring & implementation team, school directors, teachers | 124 | During program implementation | ||
| Individual interviews | Parents, teachers, implementers | 22 | Post- intervention | ||
| Quality of delivery | Both | Individual interviews | Students, parents, teachers | 24 | Post- intervention |
| Results | ||||
|---|---|---|---|---|
| Program Component | School 1 | School 2 | School 3 | School 4 |
| Classrooms | 19 | 18 | 17 | 10 |
| Total students T1–T3 (n) | 825–918 | 554–603 | 417–495 | 352–381 |
| Education program | ||||
| Nutrition sessions a T1–T3 (n) (%) + | 64–48 (67.4–84.2) | 75–49 (83.3–90.7) | 64–45 (75.3–88.2) | 48–27 (96.0–90.0) |
| PA sessions b T1–T3 (n) (%) + | 12–19 (63.2–100.0) | 18–18 (100.0–100.0) | 17–13 (100.0–76.5) | 4–10 (40.0–100.0) |
| Reach students ++ | 586–823 (71.0–89.7) | 458–444 (82.7–73.6) | 314–368 (75.3–74.3) | 319–324 (90.6–85.0) |
| Environmental activities | ||||
| Parental health education | ||||
| Sessions T1–T2 c (n) (%) + | 3–1 (100.0–33.3) | 3–1 (100.0–33.3) | 3–1 (100.0–33.3) | 3–1 (100.0–33.3) |
| Reach parents ++ | 206–220 (25.0–25.4) | 108–127 (19.5–22.9) | 103–129 (24.7–30.9) | 205–210 (58.2–55.1) |
| Teachers’ health education | ||||
| Total teachers T1–T3 (n) | 67–64 | 34–35 | 30–26 | 15–23 |
| Sessions T1–T3 (n) (%) + | 0–16 (0.0–100.0) | 0–16 (0.0–100.0) | 0–16 (0.0–100.0) | 0–16 (0.0–100.0) |
| Reach teachers ++ | 0–23 (0.0–35.9) | 0–10 (0.0–28.6) | 0–14 (0.0–53.9) | 0–11 (0.0–47.8) |
| Junior Health Promoters | ||||
| Total selected T1–T3 (n) | 95–46 | 54–54 | 52–48 | 30–33 |
| Education sessions T1–T3 (n) (%) + | 4–4 (100.0–100.0) | 1–4 (25.0–100.0) | 4–4 (100.0–100.0) | 3–4 (75.0–100.0) |
| Reach Junior Health Promoters ++ | 33–13 (34.7–28.3) | 25–47 (46.3–87.0) | 23–25 (44.2–52.1) | 28–28 (93.3–84.9) |
| Healthy Food Kiosk | ||||
| Food kiosk education (Staff) | 9–9 | 3–4 | 5–2 | 3–4 |
| Sessions T1–T3 d (n) (%) + | 7–4 (100.0–100.0) | 3–4 (42.9–100.0) | 6–4 (85.7–100.0) | 3–4 (42.9–100.0) |
| Reach kiosk staff ++ | 6–4 (66.7–44.4) | 2–2 (66.7–50.0) | 3–1 (60.0–50.0) | 2–2 (66.7–50.0) |
| Food kiosk improvement | ||||
| Total fruits exhibition stands installed (n) (%) | 1 (100.0) | 1 (100.0) | 1 (100.0) | 1 (100.0) |
| Total nutrition traffic lights installed (n) (%) | 3 (100.0) | 3 (100.0) | 3 (100.0) | 3 (100.0) |
| Food kiosk evaluation T1–T3 e (n) (%) + | 1–1 (50.0–50.0) | 1–1 (50.0–50.0) | 1–2 (50.0–100.0) | 1–1 (50.0–50.0) |
| Total leaflets wall board installed (n) (%) | 2 (100.0) | 2 (100.0) | 2 (100.0) | 2 (100.0) |
| Total minigym installed (n) (%) | * 1 (100.0) | 1 (100.0) | * 1 (100.0) | 1 (100.0) |
| Total walking events carried out T1–T3 (n) (%) | 1 (33.3) | 2 (66.7) | 2 (66.7) | 2 (66.7) |
| Reach total participants T1–T3 (n) | 825–0 | 670–? | 370–575 | 390–401 |
| Total sports Olympics carried out T1–T3 (n) (%) | 1 (33.3) | 3 (100.0) | 3 (100.0) | 3 (100.0) |
| Reach students T1–T3 (n) (%) ++ | 384–0 (46.5–0.0) | 216–? (39.0–?) | 310–? (74.3–?) | 120–? (34.1–?) |
| Leaflet distribution T1–T3 (n) (%) + | 1000–500 (100.0–100.0) | 700–500 (100.0–100.0) | 700–500 (100.0–100.0) | 600–500 (100.0–100.0) |
| Poster distribution T1–T3 (n) (%) + | 25–50 (50.0–100.0) | 25–50 (50.0–100.0) | 25–50 (50.0–100.0) | 25–50 (50.0–100.0) |
| Category | School 1 | School 2 | School 3 | School 4 | ||||
|---|---|---|---|---|---|---|---|---|
| 2015 | 2017 | 2015 | 2017 | 2015 | 2017 | 2015 | 2017 | |
| Education Program | ||||||||
| Nutrition Education | 3.66 ± 1.05 | 3.78 ± 1.01 | 3.86 ± 1.04 | 3.73 ± 1.06 | 3.86 ± 1.11 | 3.75 ± 1.06 | 3.51 ± 1.08 | 3.71 ± 0.98 |
| PA education | 3.60 ± 1.06 | 3.61 ± 1.08 | 3.53 ± 1.09 | 3.65 ± 1.01 | 3.69 ± 1.08 | 3.73 ± 1.12 | 3.60 ± 1.13 | 3.60 ± 1.07 |
| Environmental Activities | ||||||||
| Healthy Food Kiosk Initiative | 3.98 ± 1.05 | 3.80 ± 1.12 | 3.48 ± 1.19 | 3.70 ± 1.24 | 3.52 ± 1.12 | 3.44 ± 1.20 | 3.46 ± 1.06 | 3.60 ± 1.23 |
| School PA environment (minigym or equipment) | 3.41 ± 1.18 | 3.42 ± 1.28 | 3.42 ± 1.17 | 3.60 ± 1.13 | 3.84 ± 1.18 | 3.67 ± 1.19 | 3.40 ± 1.23 | 3.59 ± 1.30 |
| PA events | 3.37 ± 1.51 | 1.35 ± 1.23 | 3.96 ± 1.19 | 3.71 ± 1.21 | 4.27 ± 1.06 | 3.92 ± 1.22 | 3.93 ± 1.11 | 3.91 ± 1.21 |
| Teacher education a | 3.98 ± 1.07 | 4.42 ± 1.03 | 3.94 ± 1.11 | 3.95 ± 1.07 | 4.06 ± 1.5 | 4.41 ± 1.12 | 4.02 ± 1.07 | 4.34 ± 1.03 |
| Description | Sub-Themes | Themes |
|---|---|---|
| - Increasing mental health-related activities targeting students, parents, and teachers | (1) Greater prioritization of mental health program affects program activities and their implementation | (1) Complexity of the HPS intervention |
| - Nurse staff supported psychologists in new activities | ||
| - Responsibility of some components was transferred directly to local stakeholders | (2) Change of responsibility increases providers and the need for coordination and component description | |
| - Unclear coordination strategies between program design and implementation teams on occasions | (1) Lack of program clarity for new implementers | (2) Limited strategies to facilitate program implementation |
| - Lack of timely coordination and monitoring of components with school and health centers. | ||
| - Lack of guidelines provided to schools for PA events | ||
| - Detail of education sessions was given in plans | (2) Guidelines for education sessions | |
| - Parent sessions and walking events were informed in advance through notices in students’ school diary | (1) Program strategies to adapt to contextual factors | (3) Difficulties to maintain the participation of subjects |
| - Time availability was the main difficulty for parents in attending the sessions | ||
| - It was very difficult to gather JHP from different years, classrooms, and shifts to sessions | ||
| - JHP needed to make an effort themselves to attend sessions | ||
| - Some presents and refreshment sets were given to JHP assisting sessions | ||
| - Could not control street vendor or stores outside the school selling unhealthy foods | (2) Food environment outside school affects willing of kiosk staff to receive sessions | |
| - Kiosk staff were less willing to receive sessions because profit concerns by changes promoted by program | ||
| - Parents and teachers working long hours during the week and even on weekends | (1) Low participation of parents to sessions and low participation of teachers to program training | (4) Context |
| - Commitment of school directors and teachers representatives to adapt students sessions to school plans | (2) Commitment of school stakeholders for complying with education and environmental components | |
| - Environmental activities were not given the same importance by school stakeholders | ||
| - Stakeholders from different levels, complex hierarchical lines, and organizational procedures involved in the program | (3) Multidisciplinary character of the program |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosme Chavez, R.; Nam, E.W. Process Evaluation of a School-Based Program Aimed at Preventing Obesity in Adolescents from Lima and Callao, Peru. Int. J. Environ. Res. Public Health 2020, 17, 4804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134804
Cosme Chavez R, Nam EW. Process Evaluation of a School-Based Program Aimed at Preventing Obesity in Adolescents from Lima and Callao, Peru. International Journal of Environmental Research and Public Health. 2020; 17(13):4804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134804
Chicago/Turabian StyleCosme Chavez, Rosemary, and Eun Woo Nam. 2020. "Process Evaluation of a School-Based Program Aimed at Preventing Obesity in Adolescents from Lima and Callao, Peru" International Journal of Environmental Research and Public Health 17, no. 13: 4804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134804