Incorporating an Increase in Plant-Based Food Choices into a Model of Culturally Responsive Care for Hispanic/Latino Children and Adults Who Are Overweight/Obese

 , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
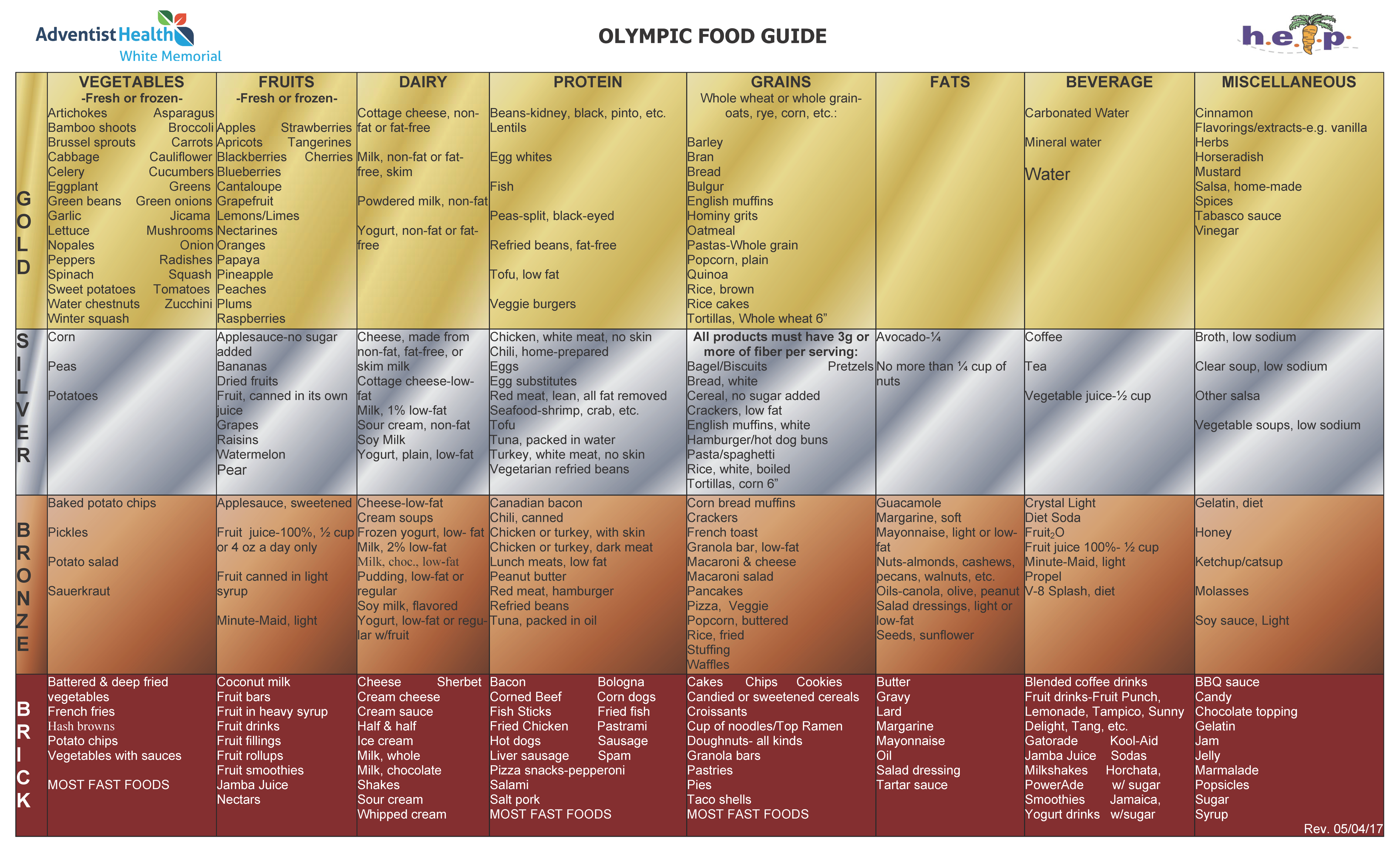
2.1. Healthy Eating Lifestyle Program (HELP) Program
2.1.1. HELP Implemented in the Context of a Culturally Competent Care Model Developed at White Memorial Medical Center
2.1.2. HELP Study Lifestyle Intervention
2.2. Qualitative Measures and Analysis
2.3. Quantitative Evaluation of the HELP Study
3. Results
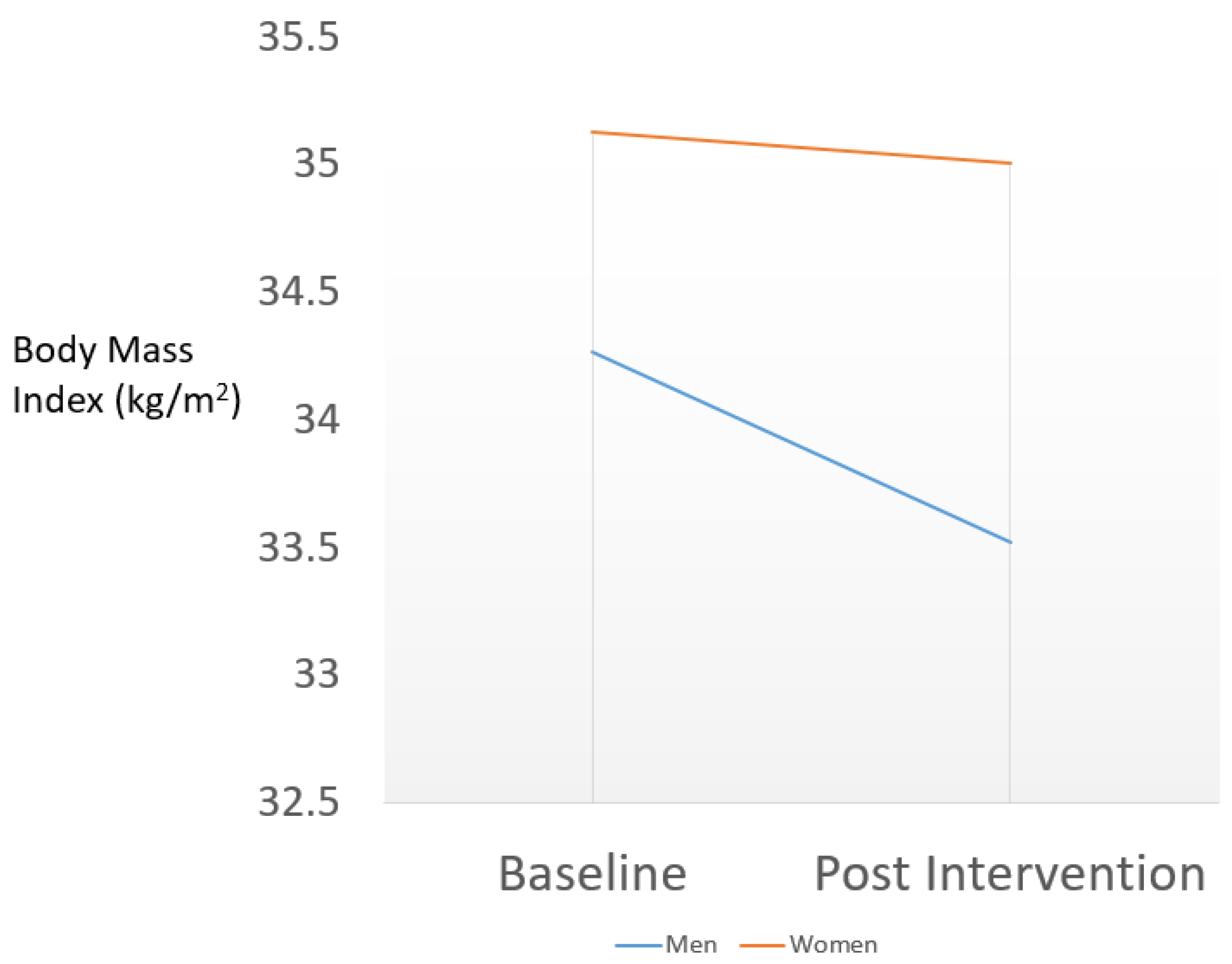
3.1. Quantitative Study of Adiposity Outcomes in HELP Participants
3.2. Qualitative Study of HELP Study Providers
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in Obesity and Severe Obesity Prevalence in US Youth and Adults by Sex and Age, 2007–2008 to 2015–2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef] [Green Version]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. Available online: https://www.cdc.gov/nchs/products/databriefs/db288.htm (accessed on 3 July 2020).
- Harris, S. Adult and Teen Obesity Rates Hit All-Time High, Cdc Reports: American Heart Association Calls for Transformative Change to Reverse Trends. Available online: https://newsroom.heart.org/news/adult-and-teen-obesity-rates-hit-all-time-high-cdc-reports 2017 (accessed on 23 September 2019).
- Barnard, N.D.; Levin, S.M.; Yokoyama, Y. A systematic review and meta-analysis of changes in body weight in clinical trials of vegetarian diets. J. Acad. Nutr. Diet. 2015, 115, 954–969. [Google Scholar] [CrossRef]
- Toumpanakis, A.; Turnbull, T.; Alba-Barba, I. Effectiveness of plant-based diets in promoting well-being in the management of type 2 diabetes: A systematic review. BMJ Open Diabetes Res. Care 2018, 6, e000534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, P.N.; Jaceldo-Siegl, K.; Shih, W.; Collado, N.; Le, L.T.; Silguero, K.; Estevez, D.; Jordan, M.; Flores, H.; McCarthy, W.J.; et al. Plant-Based Diets Are Associated With Lower Adiposity Levels Among Hispanic/Latino Adults in the Adventist Multi-Ethnic Nutrition (AMEN) Study. Front. Nutr. 2019, 6, 34. [Google Scholar] [CrossRef] [PubMed]
- Jaceldo-Siegl, K.; Estevez, D.; Fraser, G.E.; Hayes-Bautista, D.E.; Flores, H.; Jordan, M.; Singh, P.N. Plant-Based Diets in Hispanic/Latino Adult Adventists in the United States and Their Association With Body Mass Index. Am. J. Health Promot. 2019, 33, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Ramal, E.; Champlin, A.; Bahjri, K. Impact of a Plant-Based Diet and Support on Mitigating Type 2 Diabetes Mellitus in Latinos Living in Medically Underserved Areas. Am. J. Health Promot. 2018, 32, 753–762. [Google Scholar] [CrossRef]
- Ramal, E.; Petersen, A.B.; Ingram, K.M.; Champlin, A.M. Factors that influence diabetes self-management in Hispanics living in low socioeconomic neighborhoods in San Bernardino, California. J. Immigr. Minor. Health 2012, 14, 1090–1096. [Google Scholar] [CrossRef]
- Fraser, G.E. Diet, Life Expectancy, and Chronic Disease: Studies of Seventh-Day Adventists and Other Vegetarians; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Fraser, G.E. Vegetarian diets: What do we know of their effects on common chronic diseases? Am. J. Clin. Nutr. 2009, 89, 1607–1612. [Google Scholar] [CrossRef] [Green Version]
- Vang, A.; Singh, P.N.; Lee, J.W.; Haddad, E.H.; Brinegar, C.H. Meats, processed meats, obesity, weight gain and occurrence of diabetes among adults: Findings from Adventist Health Studies. Ann. Nutr. Metab. 2008, 52, 96–104. [Google Scholar] [CrossRef]
- Singh, P.N.; Clark, R.W.; Herring, P.; Sabaté, J.; Shavlik, D.; Fraser, G.E. Obesity and life expectancy among long-lived Black adults. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.N.; Arthur, K.N.; Orlich, M.J.; James, W.; Purty, A.; Job, J.S.; Rajaram, S.; Sabaté, J. Global epidemiology of obesity, vegetarian dietary patterns, and noncommunicable disease in Asian Indians. Am. J. Clin. Nutr. 2014, 100 (Suppl. 1), 359–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonstad, S.; Butler, T.; Yan, R.; Fraser, G.E. Type of vegetarian diet, body weight, and prevalence of type 2 diabetes. Diabetes Care 2009, 32, 791–796. [Google Scholar] [CrossRef] [Green Version]
- Tonstad, S.; Stewart, K.; Oda, K.; Batech, M.; Herring, R.P.; Fraser, G.E. Vegetarian diets and incidence of diabetes in the Adventist Health Study-2. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 292–299. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.N.; Sabate, J.; Fraser, G.E. Does low meat consumption increase life expectancy in humans? Am. J. Clin. Nutr. 2003, 78 (Suppl. 3), 526–532. [Google Scholar] [CrossRef] [Green Version]
- Orlich, M.J.; Singh, P.N.; Sabaté, J.; Jaceldo-Siegl, K.; Fan, J.; Knutsen, S.; Besson, W.L.; Fraser, G.E. Vegetarian dietary patterns and mortality in Adventist Health Study 2. JAMA Int. Med. 2013, 173, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Stratton, I.M.; Adler, A.I.; Neil, H.A.W.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 2000, 321, 405–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvidrez, J.; Castille, D.; Laude-Sharp, M.; Rosario, A.; Tabor, D. The National Institute on Minority Health and Health Disparities Research Framework. Am. J. Public Health 2019, 109 (Suppl. 1), S16–S20. [Google Scholar] [CrossRef] [PubMed]
- Ring, J.M.; Nyquist, J.G.; Mitchell, S.; Flores, H.; Samaniego, L. Curriculum FOR Culturally Responsive Health Care: The Step-by-Step Guide for Cultural Competence Training; Radcliffe Publishing: Oxford, UK, 2008. [Google Scholar]
- Cousineau, M.R.; Flores, H.; Cheng, S.; Gates, J.D.; Douglas, J.H.; Clute, G.B.; Coan, C.E. Transforming a family medicine center and residency program into a federally qualified health center. Acad. Med. 2013, 88, 657–662. [Google Scholar] [CrossRef] [Green Version]
- Halvorson, M. Healthy Eating Lifestyle Program (HELP). Available online: http://cdc.thehcn.net/promisepractice/index/view?pid=3542 (accessed on 2 July 2020).
- Dreimane, D.; Safani, D.; MacKenzie, M.; Halvorson, M.; Braun, S.; Conrad, B.; Kaufman, F. Feasibility of a hospital-based, family-centered intervention to reduce weight gain in overweight children and adolescents. Diabetes Res. Clin. Pract 2007, 75, 159–168. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention: Modified Z-Scores in the Cdc Growth Charts. Available online: https://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/biv-cutoffs.pdf CDC (accessed on 4 June 2020).
- Chambers, M.; Tanamas, S.K.; Clark, E.J.; Dunnigan, D.L.; Kapadia, C.R.; Hanson, R.L.; Nelson, R.G.; Knowler, W.C.; Sinha, M. Growth Tracking in Severely Obese or Underweight Children. Pediatrics 2017, 140, 2017–2248. [Google Scholar] [CrossRef] [Green Version]
- Santiago-Torres, M.; Kratz, M.; Lampe, J.W.; Tapsoba, J.D.D.; Breymeyer, K.L.; Levy, L.; Villaseñor, A.; Wang, C.-Y.; Song, X.; Neuhouser, M.L. Metabolic responses to a traditional Mexican diet compared with a commonly consumed US diet in women of Mexican descent: A randomized crossover feeding trial. Am. J. Clin. Nutr. 2016, 103, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Santiago-Torres, M.; Tinker, L.F.; Allison, M.A.; Breymeyer, K.L.; Garcia, L.; Kroenke, C.H.; Lampe, J.W.; Shikany, J.M.; Van Hore, L.; Neuhouser, M.L. Development and Use of a Traditional Mexican Diet Score in Relation to Systemic Inflammation and Insulin Resistance among Women of Mexican Descent. J. Nutr. 2015, 145, 2732–2740. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Cruz, A.; Bacardi-Gascon, M.; Turnbull, W.H.; Rosales-Garay, P.; Severino-Lugo, I. A Flexible, Low–Glycemic Index Mexican-Style Diet in Overweight and Obese Subjects With Type 2 Diabetes Improves Metabolic Parameters During a 6-Week Treatment Period. Diabetes Care 2003, 26, 1967–1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, J.A.; Caramelli, B. Vegetarians from latin america. Am. J. Cardiol. 2010, 105, 902. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.A.; Hanis, C.L. Lessons Learned from 20 Years of Diabetes Self-Management Research With Mexican Americans in Starr County, Texas. Diabetes Educ. 2014, 40, 476–487. [Google Scholar] [CrossRef]
- Hu, J.; Wallace, D.C.; McCoy, T.P.; Amirehsani, K.A. A family-based diabetes intervention for Hispanic adults and their family members. Diabetes Educ. 2014, 40, 48–59. [Google Scholar] [CrossRef]
- McEwen, M.M.; Pasvogel, A.; Murdaugh, C.; Hepworth, J. Effects of a Family-Based Diabetes Intervention on Behavioral and Biological Outcomes for Mexican American Adults. Diabetes Educ. 2017, 43, 272–285. [Google Scholar] [CrossRef]
- McEwen, M.M.; Lin, P.C.; Pasvogel, A. Analysis of behavior risk factor surveillance system data to assess the health of Hispanics with diabetes in US-Mexico border communities. Diabetes Educ. 2013, 39, 742–751. [Google Scholar] [CrossRef] [PubMed]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, P.N.; Steinbach, J.; Nelson, A.; Shih, W.; D’Avila, M.; Castilla, S.; Jordan, M.; McCarthy, W.J.; Hayes-Bautista, D.; Flores, H. Incorporating an Increase in Plant-Based Food Choices into a Model of Culturally Responsive Care for Hispanic/Latino Children and Adults Who Are Overweight/Obese. Int. J. Environ. Res. Public Health 2020, 17, 4849. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134849
Singh PN, Steinbach J, Nelson A, Shih W, D’Avila M, Castilla S, Jordan M, McCarthy WJ, Hayes-Bautista D, Flores H. Incorporating an Increase in Plant-Based Food Choices into a Model of Culturally Responsive Care for Hispanic/Latino Children and Adults Who Are Overweight/Obese. International Journal of Environmental Research and Public Health. 2020; 17(13):4849. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134849
Chicago/Turabian StyleSingh, Pramil N., Jessica Steinbach, Anna Nelson, Wendy Shih, Mary D’Avila, Selene Castilla, Michael Jordan, William J. McCarthy, David Hayes-Bautista, and Hector Flores. 2020. "Incorporating an Increase in Plant-Based Food Choices into a Model of Culturally Responsive Care for Hispanic/Latino Children and Adults Who Are Overweight/Obese" International Journal of Environmental Research and Public Health 17, no. 13: 4849. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134849