Allergic Anaphylactic Risk in Farming Activities: A Systematic Review



 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
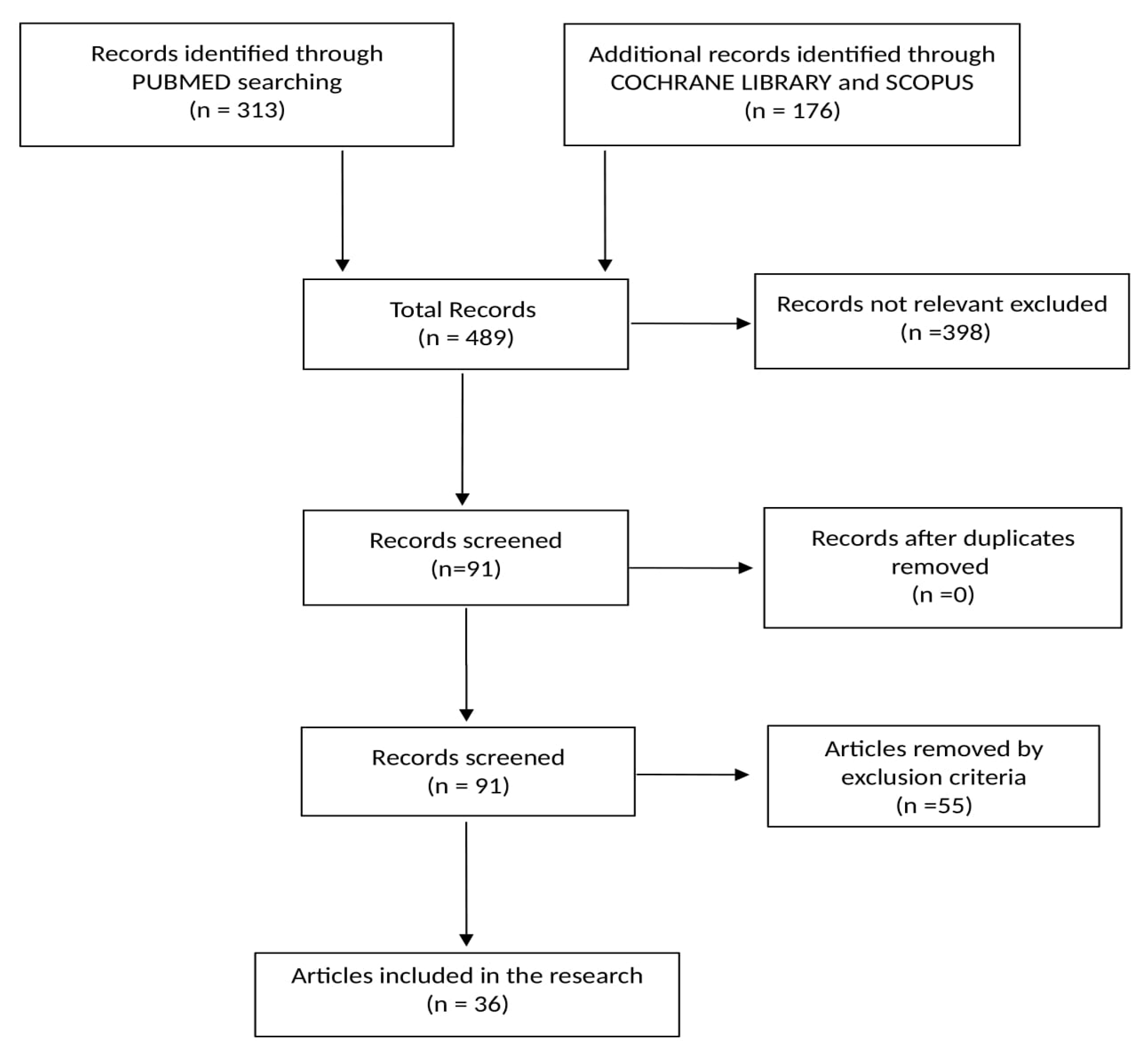
2.1. Literature Research
2.2. Quality Assessment
2.3. Eligibility and Inclusion Criteria
2.4. Exclusion Criteria
3. Results
3.1. Reviews
3.2. Original Articles
3.2.1. Main Diseases
3.2.2. Allergens
3.2.3. Agricultural Sectors and Activities
3.2.4. Demographic Characteristics of Involved Workers
3.3. Case Series and Case Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Simons, F.; Ardusso, L.R.F.; Bilò, M.B.; El-Gamal, Y.M.; Ledford, D.K.; Ring, J.; Sanchez-Borges, M.; Senna, G.E.; Sheikh, A.; Thong, B.Y.; et al. World allergy organization guidelines for the assessment and management of anaphylaxis. World Allergy Organ. J. 2011, 4, 13–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siracusa, A.; Folletti, I.; van Wijk, R.G.; Jeebhay, M.F.; Moscato, G.; Quirce, S.; Raulf, M.; Ruëff, F.; Walusiak-Skorupa, J.; Whitaker, P.; et al. Occupational anaphylaxis: An EAACI task force consensus statement. Allergy 2015, 70, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Reber, L.L.; Hernandez, J.D.; Galli, S.J. The pathophysiology of anaphylaxis. J. Allergy Clin. Immunol. 2017, 140, 335–348. [Google Scholar] [CrossRef] [PubMed]
- De Turk, S.; Reddy, S.; Pellegrino, A.N.; Wilson, J. Anaphylactic Shock. In Clinical Management of Shock—The Science and Art of Physiological Restoration; Stawicki, S.P., Swaroop, M., Eds.; IntechOpen: London, UK, 2019; pp. 1–17. [Google Scholar]
- Antoníl-Amérigo, D.; Alvarez-Perea, A.; Fiandor, A. Anaphylaxis in the workplace. Curr. Treat Options Allergy 2018, 5, 11–28. [Google Scholar] [CrossRef]
- Knight, D.; Jeebhay, M.F. Work-related anaphylaxis. Curr. Allergy Clin. Immunol. 2008, 21, 178–182. [Google Scholar]
- International Labour Office. ILO Code of Practice; International Labour Office: Geneva, Switzerland, 2011; ISBN 978-92-2-124971-9. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. On behalf of the PRISMA Group. Prisma Statement. Evidence 2015, 7, e1000114. [Google Scholar]
- La Torre, G.; Backhaus, I.; Mannocci, A. Rating for narrative reviews: Concept and development of the International Narrative Systematic Assessment tool. Senses Sci. 2015, 2, 31–35. [Google Scholar]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A. A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connel, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 8 May 2020).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; Quay, H.J.M. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Ballal, S.G. Occupational rhinitis revisited: Emphasis on the risk factors in Saudi industry. Saudi J. Med. Sci. 2016, 4, 154–163. [Google Scholar] [CrossRef]
- Quirce, S.; Bernstein, J.A. Old and new causes of occupational asthma. Immunol. Allergy Clin. N. Am. 2011, 31, 677–698. [Google Scholar] [CrossRef]
- Nordgren, T.M.; Bailey, K.L. Pulmonary health effects of agriculture. Curr. Opin. Pulm. Med. 2016, 22, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Green, B.J.; Levetin, E.; Horner, W.E.; Codina, R.; Barnes, C.; Filley, W.V. Landscape plant selection criteria for the allergic patient. J. Allergy Clin. Immunol. Pract. 2018, 6, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Green, B.J. Emerging insights into the occupational mycobiome. Curr. Allergy Asthma Rep. 2018, 18, 62. [Google Scholar] [CrossRef] [PubMed]
- Harun, N.; Lachapelle, P.; Douglass, J. Thunderstorm-triggered asthma: What we know so far. J. Asthma Allergy 2019, 12, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Nordgren, T.M.; Charavaryamath, C. Agriculture occupational exposures and factors affecting health effects. Curr. Allergy Asthma Rep. 2018, 18, 65. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, E.; AlMass, A.A.M.; Dasgupta, N.; Rahman, S.; Kim, J.; Datta, M. Assessment of occupational health hazards due to particulate matter originated from spices. Int. J. Environ. Res. Public Health 2019, 16, 1519. [Google Scholar] [CrossRef] [Green Version]
- Bilò, M.B.; Antonicelli, L.; Bonifazi, F. Honeybee venom immunotherapy: Certainties and pitfalls. Immunotherapy 2012, 4, 1153–1166. [Google Scholar] [CrossRef]
- Guan, K.; Li, L.S.; Yin, J. Use of sIgE/T-IgE in predicting systemic reactions: Retrospective analysis of 54 honeybee venom allergy cases in North China. Chin. Med. J. 2016, 129, 2091–2095. [Google Scholar] [CrossRef]
- Carballo, I.; Carballada, F.; Nuñez-Orjales, R.; Martín-Lázaro, J.; Vidal, C.; Gonzalez-Quintela, A. total and honeybee venom–Specific serum IgG4 and IgE in beekeepers. J. Investig. Allergol. Clin. Immunol. 2017, 27, 146–148. [Google Scholar] [CrossRef] [Green Version]
- Celıksoy, M.H.; Sancak, R.; Sogut, A.; Guner, S.N.; Korkmaz, A. Characteristics of venom allergic reactions in Turkish beekeepers and alternative treatment modalities. Int. Forum Allergy Rhinol. 2014, 4, 555–558. [Google Scholar] [CrossRef]
- Richter, A.G.; Nightingale, P.; Huissoon, A.P.; Krishna, M.T. Risk factors for systemic reactions to bee venom in British beekeepers. Ann. Allergy Asthma Immunol. 2011, 106, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Münstedt, K.; Wrobel, D.; Kalder, M. Efficacy of venom immunotherapy in beekeepers. J. Investig. Allergol. Clin. Immunol. 2010, 20, 58–62. [Google Scholar] [PubMed]
- Perotin, J.M.; Barbe, C.; Nguyen, K.L.; Fontaine, J.F.; Gabignon, Y.; Nardi, J.; Launois, C.; Lebargy, F.; Lavaud, F.; Deslee, G. Work-related respiratory symptoms in Champagne vineyard workers. Eur. Ann. Allergy Clin. Immunol. 2015, 47, 140–144. [Google Scholar] [PubMed]
- Galli, L.; Facchetti, S.; Raffetti, E.; Donato, F.; D’Anna, M. Respiratory diseases and allergic sensitization in swine breeders: A population-based cross-sectional study. Ann. Allergy Asthma Immunol. 2015, 115, 402–407. [Google Scholar] [CrossRef]
- Ndlovu, V.; Dalvie, M.A.; Jeebhay, M.F. Asthma associated with pesticide exposure among women in rural Western Cape of South Africa. Am. J. Ind. Med. 2014, 57, 1331–1343. [Google Scholar] [CrossRef]
- Viegas, S.; Faísca, V.M.; Dias, H.; Clérigo, A.; Carolino, E.; Viegas, C. Occupational exposure to poultry dust and effects on the respiratory system in workers. J. Toxicol. Environ. Health 2013, 76, 230–239. [Google Scholar] [CrossRef]
- Gascon, M.; Kromhout, H.; Heederik, D.; Eduard, W.; de Joode, B.v.W. Respiratory, allergy and eye problems in bagasse-exposed sugar cane workers in Costa Rica. Occup. Environ. Med. 2012, 69, 331–338. [Google Scholar] [CrossRef]
- Patiwael, J.A.; Jong, N.W.; Burdorf, A.; Groot, H.; van Wijk, R.G. Occupational allergy to bell pepper pollen in greenhouses in the Netherlands, an 8-year follow-up study. Allergy 2010, 65, 1423–1429. [Google Scholar] [CrossRef]
- Patiwael, J.A.; Vullings, L.G.J.; de Jong, N.W.; van Toorenenbergen, A.W.; van Wijk, R.G.; de Groot, H. Occupational allergy in strawberry greenhouse workers. Int. Arch. Allergy Immunol. 2010, 152, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Śpiewak, R.; Góra-Florek, A.; Horoch, A.; Jarosz, M.J.; Doryńska, A.; Golec, M.; Dutkiewicz, J. Risk factors for work-related eczema and urticaria among vocational students of agriculture. Ann. Agric. Environ. Med. 2017, 24, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Oosterhaven, J.A.F.; Verbist, J.; Schuttelaar, M.L.A. Hand eczema among Dutch beekeepers—A cross-sectional study. J. Dtsch. Dermatol. Ges. 2019, 17, 158–166. [Google Scholar] [CrossRef]
- Rennie, D.C.; Lawson, J.A.; Karunanayake, C.P.; Pahwa, P.; Chen, Y.; Chu, L.; Dosman, J.A. On behalf of the Saskatchewan Rural Health Study Group. Farm exposure and atopy in men and women: The Saskatchewan rural health study. J. Agromed. 2015, 20, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Elholm, G.; Schlünssen, V.; Doekes, G.; Basinas, I.; Omland, Ø.; Grønager, P.M.; Sigsgaard, T. Adult farming exposure does not protect against sensitization to the storage mite Lepidoglyphus destructor. Allergy 2018, 73, 2234–2237. [Google Scholar] [CrossRef]
- Merget, R.; Sander, I.; van Kampen, V.; Raulf, M.; Bruning, T. Triticale allergy in a farmer. Am. J. Ind. Med. 2016, 59, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Perle, R.; Sénéchal, H.; Andrianarisoa, A.; Rakotoarimanana, V.; Godfrin, D.; Peltre, G.; Poncet, P.; Sutra, J.-P. High IgE sensitization to maize and rice pollen in the highlands of Madagascar. Pan Afr. Med. J. 2014, 19, 284. [Google Scholar]
- Bobolea, I.; Barranco, P.; Pastor-Vargas, C.; Iraola, V.; Vivanco, F.; Quirce, S. Arginine kinase from the cellar spider (Holocnemus pluchei): A new asthma-causing allergen. Int. Arch. Allergy Immunol. 2011, 155, 180–186. [Google Scholar] [CrossRef]
- Jain, J.; Banait, S.; Srivastava, A.K.; Lodhe, R. Stroke intracerebral multiple infarcts: Rare neurological presentation of honeybee bite. Ann. Indian Acad. Neurol. 2012, 15, 163–166. [Google Scholar] [CrossRef]
- Perez-Calderon, R.; Gonzalo-Garijo, M.A.; Rodriguez-Velasco, F.J.; Sanchez-Vega, S.; Bartolome-Zavala, B. Occupational respiratory allergy in peach crop workers. Allergy 2017, 72, 1556–1564. [Google Scholar] [CrossRef]
- Reeb-Whitaker, C.K.; Bonauto, D.K. Respiratory disease associated with occupational inhalation to hop (Humulus lupulus) during harvest and processing. Ann. Allergy Asthma Immunol. 2014, 113, 534–538. [Google Scholar] [CrossRef] [Green Version]
- Ring, J.; Grosber, M.; Brockow, K.; Bergmann, K.-C. Anaphylaxis. In History of Allergy; Bergmann, K.-C., Ring, J., Eds.; Karger Publishiers: Basel, Switzerland, 2014; Volume 100, pp. 54–61. [Google Scholar]
- Portier, P.; Richet, C. De l’action anaphylactique de certains venins. C. R. Soc. Biol. 1902, 54, 170–172. [Google Scholar]
- Worm, M.; Babina, M.; Hompes, S. Causes and risk factors for anaphylaxis. J. Dtsch. Dermatol. Ges. 2013, 11, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Barg, W.; Medrala, W.; Wolanczyk-Medrala, A. Exercise-induced anaphylaxis: An update on diagnosis and treatment. Curr. Allergy Asthma Rep. 2011, 11, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, H.L. Diagnosis and treatment of insect sensitivity. J. Asthma Res. 1966, 3, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.F.T.; McKinnon, D.; Chu, K. Emergency department anaphylaxis: A review of 142 patients in a single year. J. Allergy Clin. Immunol. 2001, 108, 861–866. [Google Scholar] [CrossRef]
- Ring, J.; Messmer, K. Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet 1977, 1, 466–469. [Google Scholar] [CrossRef]
- Stark, B.J.; Sullivan, T.J. Biphasic and protracted anaphylaxis. J. Allergy Clin. Immunol. 1986, 78, 76–83. [Google Scholar] [CrossRef]
- Adkinson, N.F.; Bochner, B.S.; Busse, W.W.; Holgate, S.T.; Lemanske, R.; Simons, F.E.R. Middleton’s Allergy Principles and Practice, 7th ed.; Mosby Elsevier: Philadelphia, PA, USA, 2009; pp. 1027–1049. [Google Scholar]
- Muraro, A.; Roberts, G.; Worm, M.; Bilò, M.B.; Brockow, K.; Rivas, M.F.; Santos, A.F.; Zolkipli, Z.Q.; Bellou, A.; Beyer, K.; et al. Anaphylaxis: Guidelines from the European Academy of Allergy and Clinical Immunology. Allergy 2014, 69, 1026–1045. [Google Scholar] [CrossRef]
- Vega, J.; Vega, J.M.; Moneo, I.; Armentia, A.; Caballero, M.L.; Miranda, A. Occupational immunologic contact urticaria from pine processionary caterpillar (Thaumetopoea pityocampa): Experience in 30 cases. Contact Dermat. 2004, 50, 60–64. [Google Scholar] [CrossRef]
- De Groot, H.; Veld, C.d.G.; van Wijk, R.G. Allergy to bumblebee venom. I. Occupational anaphylaxis to bumblebee venom: Diagnosis and treatment. Allergy 1995, 50, 581–584. [Google Scholar] [CrossRef]
- Groenewoud, G.C.; Veld, C.d.G.; Nes, A.J.v.O.; de Jong, N.W.; Vermeulen, A.M.; van Toorenenbergen, A.W.; Burdorf, A.; de Groot, H.; van Wijk, R.G. Prevalence of sensitization to the predatory mite Amblyseius cucumeris as a new occupational allergen in horticulture. Allergy 2002, 57, 614–619. [Google Scholar] [PubMed] [Green Version]
- Finegold, I. Issues in stinging insect allergy immunotherapy: A review. Curr. Opin. Allergy Clin. Immunol. 2008, 8, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Ruëff, F.; Przybilla, B.; Biló, M.B.; Müller, U.; Scheipl, F.; Aberer, W.; Birnbaum, J.; Bodzenta-Lukaszyk, A.; Bonifazi, F.; Bucher, C.; et al. Predictors of severe systemic anaphylactic reactions in Hymenoptera venom allergy: Importance of baseline serum tryptase—A study of the European Academy of Allergology and Clinical Immunology Interest Group on Insect Venom Hypersensitivity. J. Allergy Clin. Immunol. 2009, 124, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Severino, M.; Bonadonna, P.; Passalacqua, G. Large local reactions from stinging insects: From epidemiology to management. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 334–337. [Google Scholar] [CrossRef]
- Sun, B.; Zheng, P.; Wang, Y.; Wei, N.; Chen, D.; Zhong, N. Analysis and measurement of sixteen common allergens in children with respiratory disorders in Guangzhou. Clin. J. Biomed. Eng. 2009, 15, 45–48. [Google Scholar]
- Hemmer, W.; Focke, M.; Kolarich, D.; Dalik, I.; Götz, M.; Jarisch, R. Identification by immunoblot of venom glycoproteins displaying immunoglobulin E-binding N-glycans as cross-reactive allergens in honeybee and yellow jacket venom. Clin. Exp. Allergy 2004, 34, 460–469. [Google Scholar] [CrossRef]
- Sturm, G.J.; Kranzelbinder, B.; Schuster, C.; Sturm, E.M.; Bokanovic, D.; Vollmann, J.; Crailsheim, K.; Hemmer, W.; Aberer, W. Sensitization to Hymenoptera venoms is common, but systemic sting reactions are rare. J. Allergy Clin. Immunol. 2014, 133, 1635–1643. [Google Scholar] [CrossRef]
- Nakagawa, T.; Miyamoto, T. The role of IgG4 as blocking antibodies in asthmatics and in beekeepers. Int. Arch. Allergy Appl. Immunol. 1985, 77, 204–205. [Google Scholar] [CrossRef]
- Hayashi, Y.; Hirata, H.; Watanabe, M.; Yoshida, N.; Yokoyama, T.; Kakuta, T.; Murayama, Y.; Sugiyama, K.; Arima, M.; Fukushima, Y.; et al. Usefulness of specific-IgG4 to Hymenoptera venom in the natural history of hymenoptera stings. J. Investig. Allergol. Clin. Immunol. 2014, 24, 192–194. [Google Scholar]
- Varga, E.M.; Kausar, F.; Aberer, W.; Zach, M.; Eber, E.; Durham, S.R.; Shamji, M.H. Tolerant beekeepers display venom-specific functional IgG4 antibodies in the absence of specific IgE. J. Allergy Clin. Immunol. 2013, 131, 1419–1441. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Menardo, J.M.; Aznar, R.; Robinet-Levy, M.; Michel, F.B. Clinical and immunologic survey in beekeepers in relation to their sensitization. J. Allergy Clin. Immunol. 1984, 73, 332–340. [Google Scholar] [CrossRef]
- Golden, D.B.; Marsh, D.G.; Kagey-Sobotka, A.; Freidhoff, L.; Szklo, M.; Valentine, M.D.; Lichtenstein, L.M. Epidemiology of insect venom sensitivity. JAMA 1989, 262, 240–244. [Google Scholar] [CrossRef]
- Christensen, L.H.; Holm, J.; Lund, G.; Riise, E.; Lund, K. Several distinct properties of the IgE repertoire determine effector cell degranulation in response to allergen challenge. J. Allergy Clin. Immunol. 2008, 122, 298–304. [Google Scholar] [CrossRef]
- Przybilla, B.; Ruëff, F. Hymenoptera venom allergy. J. Dtsch. Dermatol. Ges. 2010, 8, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Susitaival, P. Epidemiological Study of Hand Dermatoses and Other Skin Diseases in a Cohort of Finnish Farmers. Ph.D. Thesis, Kuopio University, Kuopio, Finland, 1996. [Google Scholar]
- Ercilla-Montserrat, M.; Izquierdo, R.; Belmonte, J.; Montero, J.I.; Munoz, P.; De Linares, C.; Rieradevall, J. Building-integrated agriculture: A first assessment of aerobiological air quality in rooftop greenhouses (i-RTGs). Sci. Total Environ. 2017, 598, 109–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, M.; Maibach, H.I. The clinical significance of immunological contact urticaria to processed grains. Indian J. Dermatol. Venereol. Leprol. 2012, 78, 591–594. [Google Scholar] [CrossRef]
- Spiewak, R.; Gora, A.; Dutkiewicz, J. Work-related skin symptoms and type I allergy among eastern-Polish farmers growing hops and other crops. Ann. Agric. Environ. Med. 2001, 8, 51–56. [Google Scholar]
- Green, B.J.; Couch, J.R.; Lemons, A.R.; Burton, N.C.; Victory, K.R.; Nayak, A.P.; Beezhold, D.H. Microbial hazards during harvesting and processing at an outdoor United States cannabis farm. J. Occup. Environ. Hyg. 2018, 15, 430–440. [Google Scholar] [CrossRef]
- Pesonen, M.; Koskela, K.; Aalto-Korte, K. Contact urticaria and protein contact dermatitis in the Finnish Register of Occupational Diseases in a period of 12 years. Contact Dermat. 2020, 83, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Monso, E. Occupational Asthma in greenhouses workers. Curr. Opin. Pulm. Med. 2004, 10, 147–150. [Google Scholar] [CrossRef]
- Chatzi, L.; Prokopakis, E.; Tzanakis, N.; Alegakis, A.; Bizakis, I.; Siafakas, N.; Lionis, C. Allergic rhinitis, asthma, and atopy among grape farmers in a rural population in Crete, Greece. Chest 2005, 127, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Radon, K.; Monso, E.; Weber, C.; Danuser, B.; Iversen, M.; Opravil, U.; Donham, K.; Hartung, J.; Pedersen, S.; Garz, S.; et al. Prevalence and risk factors for airway diseases in farmers—Summary of results of the European farmers’ project. Ann. Agric. Environ. Med. 2002, 9, 207–213. [Google Scholar] [PubMed]
- Filipiak, B.; Heinrich, J.; Schäfer, T.; Ring, J.; Wichmann, H.E. Farming, rural lifestyle and atopy in adults from southern Germanydresults from the MONICA/KORA study Augsburg. Clin. Exp. Allergy 2001, 31, 1829–1838. [Google Scholar] [CrossRef]
- Portengen, L.; Sigsgaard, T.; Omland, Ø.; Hjort, C.; Heederik, D.; Doekes, G. Low prevalence of atopy in young Danish farmers and farming students born and raised on a farm. Clin. Exp. Allergy 2002, 32, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Ernst, P.; Cormier, Y. Relative scarcity of asthma and atopy among rural adolescents raised on a farm. Am. J. Respir. Crit. Care Med. 2000, 161, 1563–1566. [Google Scholar] [CrossRef]
- Hoppin, J.A.; Umbach, D.M.; London, S.; Henneberger, P.K.; Kullman, G.J.; Alavanja, M.C.; Sandler, D.P. Pesticides and atopic and non-atopic asthma among farm women in the Agricultural Health Study. Am. J. Respir. Crit. Care Med. 2008, 177, 11–18. [Google Scholar] [CrossRef]
- Enholm, G.; Schlunssen, V.; Doekes, G.; Basinas, I.; Bibby, B.M.; Hjort, C.; Grønager, P.M.; Omland, Ø.; Sigsgaard, T. Become a farmer and avoid new allergic sensitization: Adult farming exposures protect against new-onset atopic sensitization. J. Allergy Clin. Immunol. 2013, 132, 1239–1241. [Google Scholar]


{kind=link}
| First Author | Year | Study | Key Messages |
|---|---|---|---|
| Al-Maneea | 2013 | cross-sectional | Exposure to animal products (dust, pigeon, dog, cat, turkey) exacerbates allergic asthma |
| Ballal | 2016 | narrative review | Storage mites and cow’s dander are the commonest causes of occupational rhinitis in this occupational group |
| Bilò | 2012 | narrative review | Allergic beekeepers represent unique populations for epidemiological, venom allergy immunopathogenesis and mechanism studies |
| Bobolea | 2011 | case control | Spiders represent an important but as yet unexplored source of indoor allergens, especially in agricultural environments |
| Carballo | 2017 | case-control | High concentrations of HBV-sIgG4 associated with less severe sting reactions in beekeepers. HBV-sIgE tended to be higher in beekeepers with more severe reactions, while total serum IgE was lower in beekeepers than in controls. |
| Çelıksoy | 2014 | cross-sectional | The risk of a severe reaction to bee stings increases with the degree of exposure and beekeepers are at the highest risk |
| Elholm | 2018 | cohort Studies | Storage mites can be typical occupational allergen for which new sensitization might occur in the first years of a farmer’s work life. |
| Ercilla-Montserrat | 2017 | experimental study | It is possible to recirculate the air of the i-RTG to the building, thus to converting the system into an Bi-RTG without posing health risks due to allergies for the building users if the biological air quality is monitored and the corresponding preventive measures are taken, even with the installation of air filters. |
| Galli | 2015 | case-control | The prevalence of allergic diseases is lower in people who reside in the countryside and therefore are exposed to bacterial, parasitic, and viral infections during childhood |
| Gascon | 2012 | cohort study | During the harvesting season, the prevalence of wheeze and eye problems almost doubled in workers exposed to bagasse and other types of dust |
| Green | 2018 | narrative Review | Health and safety precautions used in the landscape industry can be used by gardeners, landscapers and arborists to reduce or eliminate exposure to biological hazards |
| Green | 2018 | narrative Review | Occupational fungal exposures include a much broader diversity of fungi than once thought |
| Green | 2018 | pilot study | Potential exposure to microbiological hazards, such as Actinobacteria and cannabis fungal, in workers that harvest, bud strip or hand trim organically produced cannabis. |
| Guan | 2016 | case-control | The use of sIgE/T-IgE results is a useful diagnostic parameter in determining honeybee venom allergy |
| Harun | 2019 | narrative review | Wheat harvesting has implicated in respiratory symptoms, with fungal spores as the predominant aeroallergen |
| Jain | 2012 | case report | Venom bee stings can cause neurological complications (stroke, seizure, aphasia, dysarthria, apraxia, ataxia and coma) |
| Merget | 2016 | case control | Triticale allergy may occur as a distinct allergy in farmers |
| Munstedt | 2010 | cross-sectional | Desensitization can result in a complete absence of symptoms after re-exposure to bee stings |
| Ndlovu | 2014 | cross-sectional | Pesticide exposure among women farm workers is associated with increased risk of ocular nasal symptoms and an elevated asthma symptom |
| Nordgren | 2018 | narrative Review | Working and/or living near CAFOs (concentrated animal feeding operations) is a risk factor for development of various respiratory diseases due to various contaminants, like biological dust, pesticides and zoonotic pathogens |
| Nordgren | 2016 | narrative Review | In agricultural industry, occupational exposures to bioaerosols and inorganic aerosols lead to increased risk for lung disease amongst workers |
| Oosterhaven | 2019 | cross-sectional | The prevalence of hand eczema in beekeepers was higher than in the general population, but a small subset of beekeepers suffered it |
| Patiwael | 2010 | cohort study | Pollen from bell pepper plants cultivated in greenhouses cause occupational allergic disease |
| Patiwael | 2010 | cross-sectional | Allergic symptoms attributable to the workplace are present among a proportion of strawberry greenhouse employees |
| Perez-Calderon | 2017 | case-series | Sensitization to no-pollen tree structures, such as peach leaves, may cause occupational respiratory symptoms. |
| Perotin | 2015 | cross-sectional | Work-related respiratory symptoms are frequent and associated with a sensitization to gramineae and with activities performed close to vine in late spring |
| Pesonen | 2020 | cross-sectional | Main causes of CU and PCD in Finnish workers are animal dander, grain, NRL, and plant- and animal derived foods. |
| Quirce | 2011 | narrative review | Asthma rapidly accelerated with the advent of new technologies introducing a spectrum of new agents into the workplace |
| Ramavovololona | 2014 | cohort study | Major allergens β-expansins, profilin and polygalacturonase were characterized both in maize and rice pollen |
| Reeb-Whitaker | 2014 | case series | Occupational exposure to hop dust is associated with respiratory disease, especially in hop workers |
| Rennie | 2015 | cross-sectional | There are associations between atopic sensitization and farm living that appear to vary by sex. Specific allergens appear to be more important for an increase in or protection from allergy that is related to the timing of farming exposures. |
| Richter | 2011 | cross-sectional | Factors that predisposed beekeepers to allergic reactions are female gender, having a family member with bee venom allergy, more than 2 years of beekeeping and premedication with an antihistamine |
| Sabino | 2012 | case control | This study confirmed the presence and distribution of Aspergillus in Portuguese poultry and swine farms |
| Spiewak | 2017 | cross-sectional | Work with hops is the kind of plant production associated with most frequent skin diseases, followed by work with grain, hay and straw. Skin prick tests do not correlate well with referred symptoms. |
| Upadhyay | 2019 | narrative review | People involved in spice agriculture and food industries are at greater risk to long and short-term respiratory issues |
| Viegas | 2013 | cross-sectional | Poultry farm workers are more prone to suffer from respiratory ailments and this may be attributed to higher concentrations of particulate in the dust |
| First Author | Included Subjects | Allergic Disease | Allergens | Category Workers | Scores |
|---|---|---|---|---|---|
| Ballal SG | Rhinitis | various | Farmers, florists, greenhouse, animal, grain handlers | I.5 | |
| Bilò MB | Anaphylaxis | Bee Venom | Beekeepers | I.5 | |
| Green BJ | Respiratory disease | Fungal bioaerosols | Various | I.5 | |
| Green BJ | Respiratory, dermatologic | Pollen, Arthropods, Bioaerosol | Gardeners, Horticulture, Greenhouse | I.5 | |
| Harun DS | Asthma | Pollen | agricultural activities | I.5 | |
| Nordgren M | Respiratory disease | Biological Dust, Bioaerosols | Various | I.5 | |
| Nordgren M | Respiratory disease | Aeroallergens | Farmers | I.5 | |
| Quirce S | Asthma | Various | Various | I.6 | |
| Upadhyay E | Respiratory, dermatologic | Arthropods | Spice agricultural workers | I.5 | |
| Bobolea I | 1 case, 5 controls | Asthma | Arthropods | Cereal workers | N.6 |
| Carballo I | 158 cases, 465 controls | Anaphylaxis | Honeybee Venom | Beekeepers | N.6 |
| Elholm G | not specified | Sensitization | Arthropods | Farmer, Millers, Cattlemen | N.7 |
| Ercilla-Montserrat M | not specified | Respiratory disease | Biological dust | Greenhouses worker | n.a. |
| Galli L | 101 cases, 82 controls | Respiratory disease | Aeroallergens | Swine breeders | N.6 |
| Gascon M | N.74 | Respiratory, ocular disease | Biological dust | Sugarcane workers | N.6 |
| Green BJ | not specified | Respiratory, dermatologic | Microbiological hazard | Farm Cannabis workers | n.a. |
| Guan K | 54 cases | Anaphylaxis | Honeybee Venom | Beekeepers | N.3 |
| Jain J | N.1 | Stroke | Bee Venom | Beekeepers | n.a. |
| Merget R | 1 case, 4 controls | Asthma | Triticale | Farmers | N.6 |
| Patiwael JA | N.322 | Respiratory disease | Pepper Pollen | Greenhouses | N.7 |
| Perez-Calderon | N.37 | Respiratory disease | Peach tree | Peach Crop | n.a. |
| Ramavovololona | N.65 | Respiratory, dermatologic | Pollen | Maize, Rice Crop | N.5 |
| Reeb-Whitaker | N.57 | Respiratory disease | Lupulus | Hop workers | n.a. |
| Sabino R | 47 cases, 28 controls | Respiratory, dermatologic | Aspergillus | Swine, Poultry workers | N.7 |
| First Author | Included Subjects | Allergic Disease | Allergen | Category Workers | Score |
|---|---|---|---|---|---|
| Al-Maneea | N.10 | Respiratory disease | Animals | Not specified | N.5 |
| Çelıksoy MH | N.301 | Anaphylaxis | Bee Venom | Beekeepers | N.5 |
| Munstedt K | N.63 | Anaphylaxis | Bee Venom | Beekeepers | N.5 |
| Ndlovu V | N.211 | Asthma | Pesticide | Not specified | N.6 |
| Oostarhaven | N.833 | Dermatitis | Various (propolis) | Beekeepers | N.7 |
| Patiwael JA | N.75 | Respiratory, dermatologic | Strawberry Pollen | Greenhouses | N.6 |
| Perotin JM | N.307 | Respiratory disease | Aeroallergens | Vineyard workers | N.5 |
| Pesonen M | N.570 | Dermatitis | Cow, grain, flour dust | farmers, livestock workers, gardeners | N.6 |
| Rennie DC | n.11982 | Atopic/allergic reaction | Aeroallergens | Farmers | N.7 |
| Richter AG | N.852 | Anaphylaxis | Bee Venom | Beekeepers | N.6 |
| Spiewak | N.440 | Dermatitis | Biological dust | students of agriculture | N.8 |
| Viegas S | N.46 | Respiratory disease | Poultry dust | Poultry farmworkers | N.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arcangeli, G.; Traversini, V.; Tomasini, E.; Baldassarre, A.; Lecca, L.I.; Galea, R.P.; Mucci, N. Allergic Anaphylactic Risk in Farming Activities: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17144921
Arcangeli G, Traversini V, Tomasini E, Baldassarre A, Lecca LI, Galea RP, Mucci N. Allergic Anaphylactic Risk in Farming Activities: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(14):4921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17144921
Chicago/Turabian StyleArcangeli, Giulio, Veronica Traversini, Emanuela Tomasini, Antonio Baldassarre, Luigi Isaia Lecca, Raymond P. Galea, and Nicola Mucci. 2020. "Allergic Anaphylactic Risk in Farming Activities: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 14: 4921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17144921