The present study demonstrated a high prevalence of the use of added salt, and lower of added sugar and both ingredients in the diets of the Polish and Austrian toddlers. Furthermore, those rates were higher in toddlers aged 25–36 months compared to 12–24 months. It was also observed that the strongest sociodemographic factor associated with the use of added salt, sugar and both salt and sugar was multiparity. Among early feeding factors, current breastfeeding, duration of exclusive breastfeeding and method of introducing complementary foods were the strongest. Moreover, toddlers who consumed meals with added salt and sugar also showed poorer dietary patterns and meal environment. Interestingly, it was also observed that those mothers who used added salt (and sugar to a lesser extent) tended to be more concerned about their children’s feeding practices. The obtained results were specific for the country, as well as diminished with toddlers’ age.
4.1. Prevalence of the Use of Added Salt and Sugar in the Toddlers’ Diets
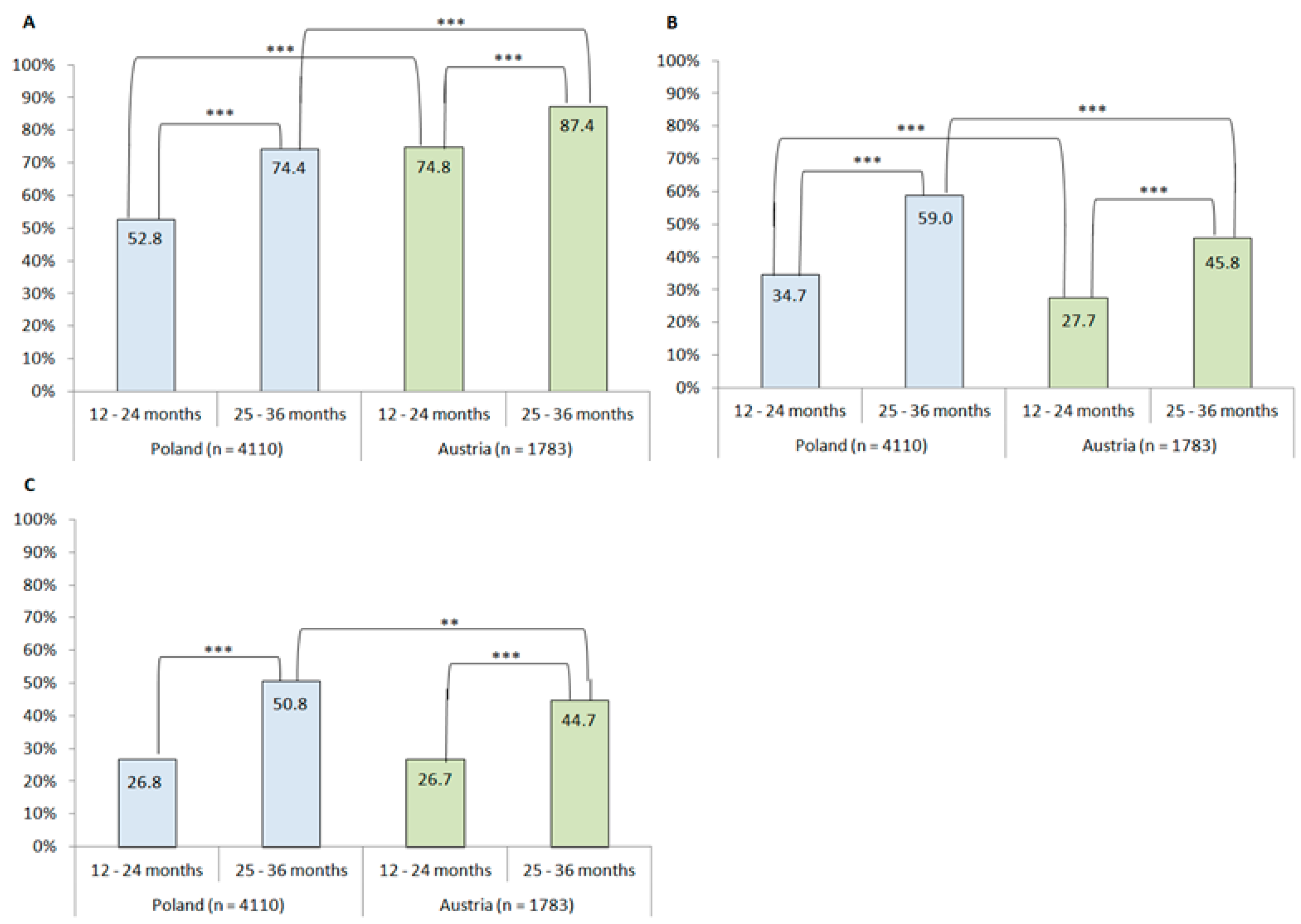
Half of the Polish mothers and three-quarters of the Austrian mothers declared the use of added salt in the diet of their two year old toddlers; for added sugar, these came to one-third for the Polish mothers and one-quarter for the Austrian mothers. Therefore, those rates were higher among older toddlers. Previous studies reported that from 25% (France [
27]) to 50% (USA [
34]) and 60% (Sri Lanka [
35]) of infants received meals with the addition of salt before the end of 12 months of age. A study from Australia showed that around 40% of toddlers aged 2–3 years consumed meals with added salt, and 11% of them added salt at the table [
24]. Sugar was added into the diet of 25% of 10 month infants from France [
27] and 42% of infants from Sri Lanka [
35]. These rates increased with children’s age, which is in accordance with the results of other studies conducted in Europe [
27,
36,
37] and was also confirmed in the present study. The odds of the use of added salt and sugar into toddlers’ diets increased by 18% and 14% (Poland) and 16% and 13% (Austria) per month in the second year of life, respectively. Whereas in the present study, only the use of added salt and sugar as ingredients was assessed, various studies investigated the use of added salt or sugar as well as the intake of salt or sodium and added or free sugars. The use of added salt and sugar intake is inseparably associated with sodium and added/free sugars intake, which also increased with children’s age [
21,
22,
23,
28,
37,
38,
39,
40,
41]. Unfortunately, many infants and toddlers around the world have intakes of sodium [
25,
26,
38,
39,
42,
43] and added/free sugars [
22,
28,
37,
39,
40,
43,
44,
45] already close to the upper limit or even above recommendations. Interestingly, many studies conducted on infants and children have shown that boys compared to girls had a higher intake of sodium [
21,
23,
26,
46]. Concerning sugar intake, the results are inconclusive. Some studies demonstrated higher intake among girls than boys [
40], whereas in the study conducted by Yuan et al. [
47], boys were more prone to consume added sugar, however, it was only observed at 8 months of age. Nonetheless, in our study, we did not observe any gender differences in the prevalence of use of added salt, sugar and both salt and sugar (results not presented).
4.2. Sociodemographic Factors Associated with the Use of Added Salt and Sugar in the Toddlers’ Diets
Multiparity was associated with the use of added salt and sugar in the toddlers’ diets, whereas maternal age, education, and the economic situation showed limited influence. Multiparity was the strongest factor that increased the odds of use of added salt, sugar and both ingredients by 32–85% in the diets of the Polish toddlers aged 12–36 months and the Austrian toddlers aged 12–24 months. Previously, it was reported that Japanese 3 year old toddlers with older siblings exhibited a higher urinary sodium excretion, as well as daily consumption of snacks compared to firstborn children [
48]. Results concerning the use of added sugar and parity are ambiguous, as in the study of Marinho et al. [
40], no association between having siblings and use of added sugar was found, but Yuan et al. [
47] demonstrated that consumption of added sugar was associated with having a multiparous mother. Our results are consistent with previous results from France [
27] and observations from a focus study conducted in five European countries, in which some parents declared following the nutritional guidelines for the firstborn child, but for the second one they “did not follow them as closely” and in consequence, dietary practices were poorer [
49,
50]. Maternal education remained not significant after adjustment for covariates. Whereas poorer early feeding practices were associated with maternal lower education level [
31,
51,
52], no associations regarding salt use or sodium intake in infants and toddlers [
25,
26,
34] were observed, in contrast to free sugars intake in children [
40]. Moreover, a limited inverse association between economic situation and use of added salt and both ingredients in the diet of the Polish toddlers aged 12–24 months, as well as salt in the diet of the Austrian toddlers in this age was noticed. Although a lower economic situation was previously linked to poorer feeding practices during the first years of life [
53], it was not observed in relation to sodium [
46] or added sugars intake [
37], nor sugar and salt use [
27], as well as the timing of introducing solids analyzed in our previous study [
31].
4.3. Early Feeding Factors Associated with the Use of Added Salt and Sugar in the Toddlers’ Diet
A lack of current breastfeeding increased the odds of use of added salt, sugar, and both of them in the younger group from Austria, as well as the odds of the use of added salt in the older group from Poland. Additionally, a lack or lower duration of exclusive breastfeeding increased the odds of use of added sugar and both salt and sugar in the younger group, and use of added salt in the older group from Poland, as well as the use of added sugar and both ingredients in the older group from Austria. These results are in agreement with previous studies that linked breastfeeding with better dietary habits during infancy and subsequent life [
23,
42,
54] and lower sodium intake in breastfed children [
25,
26,
42]. Nevertheless, in the study of Yuan et al. [
47], intake of added sugars was not significantly associated with breastfeeding duration. Breastfeeding is also associated with higher intake of unprocessed foods and lower intake of processed foods, which are main sources of salt/sodium and added sugars in the diet [
23,
24,
54,
55]. Breastmilk is an important source of chemosensory information and plays a pivotal role in developing children’s food preferences [
2,
8]. Moreover, breastfeeding mothers tend to be older and better educated than those who are not breastfeeding their children [
42,
54]. This fact may lead to better compliance with nutritional guidelines and in consequence, healthier dietary and lifestyle habits in family and children [
2,
4,
26,
51,
56,
57]. In contrary to previous results, a study from France found that any breastfeeding duration was positively associated with use of added salt and sugar in infants’ diet [
27]. The authors hypothesized that it may be caused by a choice of introducing homemade complementary foods rather than commercial ones, which was higher in breastfeeding mothers and was confirmed in other studies [
27,
54]. Unfortunately, several studies reported that homemade or family foods were often prepared with salt or sugar addition against nutritional recommendations and consequently, contributed into sodium or added sugars intake [
8,
10,
25,
26].
In the present study, we did not observe a significant association between the use of added salt or sugar and types of complementary foods. Interestingly, the use of commercial complementary foods tends to be a risk factor of the use of added salt in the younger Polish and older Austrian toddlers. Despite a lack of association in the present study, a previous longitudinal investigation reported that higher consumption of commercial baby foods increased the intake of added sugars in later childhood [
22]. Analysis of commercial baby foods from four cities in the European region revealed that many of them contained more than the recommended amount of sodium and sugars, possibly due to the addition of salty or sweet ingredients, such as ham, cheese, or concentrated fruit juices [
10]. These results are consistent with previous studies from the USA, which showed that 58% and 45% [
58] or 84% and 70% [
59] of commercial toddler foods had high sodium or added sugar levels, respectively. The authors emphasized that many commercial infant and toddler foods did not fulfill the criteria of healthy foods in accordance with age, despite parents’ perception [
49,
58].
Timing and method of introducing complementary foods into an infant’s diet are other aspects that might determine subsequent dietary habits and food preferences [
2,
8]. In a few previous studies, it was observed that too early starting of complementary feeding (before 4 months) was related to salt/sodium intake [
25,
26,
27] and use of added sugar [
27]. However, our study did not replicate these findings, as the association between the use of added salt, sugar, and age of introducing complementary foods did not remain significant after adjustment to maternal sociodemographic and early feeding factors. Moreover, early introducing of solids seems to be a plausible risk factor of the use of added salt in toddlers’ diet. Parents who introduced solids earlier had more time to introduce salt and sugar [
27], and those children were characterized by poorer dietary patterns or feeding difficulties [
56,
60]. This may be partially explained by poorer following of nutritional recommendations [
57] and maternal characteristics [
31,
51,
53], similar to breastfeeding.
Finally, the method of introducing complementary foods may be an important factor that contributes to shaping dietary habits and food preferences [
61]. We observed that following the BLW method decreased odds of use of added salt in the diet of the Polish toddlers, whereas traditional spoon-feeding increased them in the younger group. Moreover, BLW decreased odds of use of added sugar and both ingredients in the older toddlers. Previous studies have shown equivocal results of sodium intake according to the method of introducing solids. Morison et al. [
62] reported no difference in intake of sodium or sugars according to the method of introducing solids, whereas in a study of Erickson et al. [
38], infants who were introduced to solids using a modified BLW method (BLISS) had a higher intake of sodium at 7 months, but not at 24 months, with no difference in added sugars intake. Those differences may be caused by higher consumption of family foods than commercial complementary foods during feeding by the BLW method [
63]. Our results may be explained in two ways. First, infants who were introduced to solids by the BLW method tend to be breastfed longer, introduced to complementary foods later, and their mothers had better characteristics which lead to healthier feeding practices [
31,
62,
63,
64,
65,
66]. Second, the BLW method is associated with more responsive parental feeding practices [
64] and was linked to lower fussiness in later childhood [
65].
4.4. The Use of Added Salt and Sugar and Toddlers’ Dietary Habits and Maternal Concerns About Eating
Interestingly, in the present study, toddlers’ dietary patterns varied under consideration of the consumption of meals with or without added salt or sugar. The Polish and Austrian toddlers who consumed added salt and sugar more often followed a Western-like pattern and less often pro-health pattern, characterized by more frequent consumption of low-processed foods, such as vegetables and fruits, grains, or water. Those results are consistent with previous studies that linked salt intake with consumption of sugar-sweetened beverages [
67] or consumption of savory snacks with sugar-sweetened beverages and sweets [
56]. Toddlers who a followed Western-like dietary pattern may be a risk group of higher sodium/salt [
24,
26,
39,
68,
69] or sugars [
37,
39,
40,
45] intake from processed foods which are characteristic of this pattern. Moreover, higher consumption of salty and sweet foods may blunt the appetite and decrease the intake of nutrient-dense food [
35]. Furthermore, early exposure to unhealthy foods is associated with enhanced preference and increased intake of these foods in later childhood [
23,
70]. In the present study, around one-quarter of the younger and half of the older toddlers from both age groups consumed meals with added both salt and sugar. The results are in accordance with previous studies which reported that the introduction of those ingredients into infants’ or toddlers’ diets is highly associated with each other [
23,
27,
34,
35,
71]. This may be explained in several ways. Firstly, salty and sweet preferences in children are correlated with each other and are related to dietary intake of salty, but not sweet foods [
72]. Secondly, a lot of commercial complementary foods contain not only too much salt/sodium, but also sugar [
58,
59]. Thirdly, mothers who do not follow strictly nutritional guidelines about salt may be more likely to also add sugar during the complementary feeding period [
57]. Furthermore, Polish toddlers, who consumed meals with added salt and sugar, were more often eating meals during watching TV, which may be one of the predictors of poorer dietary habits [
56].
Regarding the results considering the mothers’ concerns about their toddlers’ eating behaviors, it could be noticed that, the Polish mothers who prepared meals without the addition of salt and sugar were less concerned about their toddlers’ eating, whereas in other groups, concerns about “eating too little” (only salt and both ingredients), “not eating vegetables” or “not eating novel foods” were reported more often. Therefore, we hypothesized that those mothers may use added salt and sugar as an encouraging strategy to increase the intake of those foods, as mothers who are more concerned about children’s eating are prone to have less responsive feeding practices [
4]. Furthermore, the addition of salt, but not sugar, has a dose-dependent influence on the toddlers’ vegetable intake [
73]. However, in a previous study from France, the authors did not observe any association between maternal concerns about the child’s health and salt or sugar use during infancy [
27].
4.5. Sources of Knowledge About Children’s Feeding
Presented results showed that mothers of the Polish toddlers who used added salt and sugar in children’s meals more often declared family or friends and TV as sources of knowledge about children’s feeding, whereas nutritionists or dieticians were reported less often. Similar results were observed previously by Bournez et al. [
27] in regard to sugar, but not salt use. However, in both studies, the Internet was the main source of knowledge about nutrition. Previously, relatively high parental consciousness about health risks and the necessity of reduction in salt and sugar in children’s feeding were reported [
48,
71]. Morinaga et al. [
48] did not find any associations with salt intake in children, whereas Khokhar et al. [
71] reported that those parents more often declared behaviors aimed to reduce salt intake in children. Interestingly, some studies suggest that children of parents who restricted sugar intake have increased sweetness preference [
5]. Those results emphasize the necessity of educational interventions to improve parental practices from the beginning of the introduction of solids into the infant’s diet.
Most of the results observed in the present study were significant only in the Polish sample, especially the younger group. A potential explanation for this difference between results obtained in both evaluated countries is the higher prevalence of salt addition in Austrian toddlers. Nearly 90% of older Austrian toddlers received meals with added salt, and this fact could lead to diminishing gaps in toddlers’ characteristics within both subgroups. Moreover, the strength of the factors associated with the use of added salt may also reduce because of the use of added salt increases with toddlers’ age. In our previous paper, which was a part of the present study, we also observed that the Austrian mothers were following the WHO recommendations about the age of introduction of complementary feeding less often than the Polish mothers [
31].
4.6. Strengths and Limitations
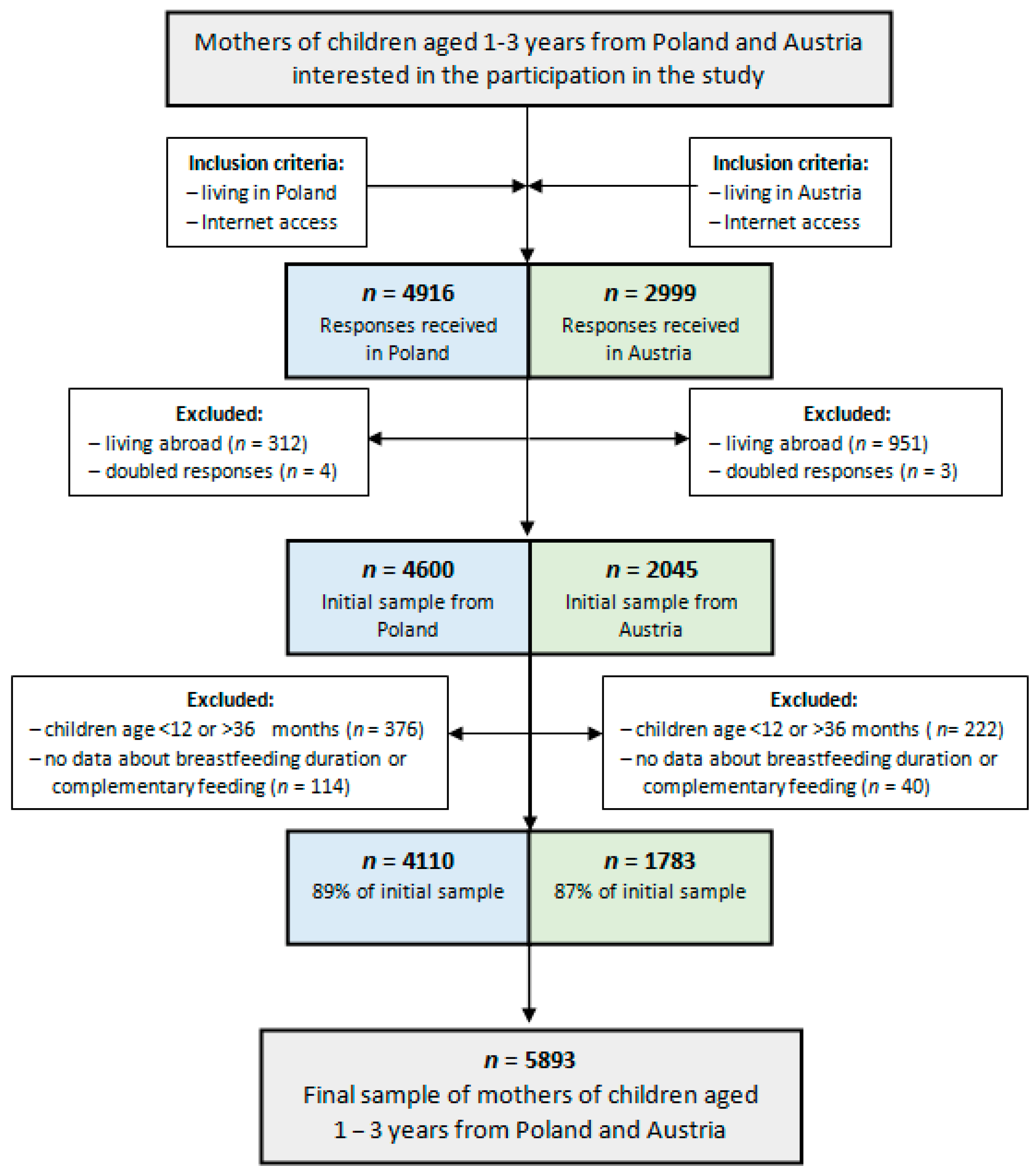
An important strength of this study was the large sample size (
n = 5893) from two European countries. Due to the study design and administration of the questionnaire via the Internet, it was possible to reach out to mothers from diverse parts of Poland and Austria and provide equal access for participation over geographical and financial barriers. Moreover, we assessed the prevalence of the use of added salt, sugar, and both of them in two age categories, which is important because of the fact that children younger than 2 years should not be given added salt nor sugar [
10]. Further, our study was able to explore some plausible factors associated with the use of added salt and sugar, both sociodemographic and early feeding, as well as to investigate the association between dietary habits among children with different statuses of use of added salt and sugar. It is worth emphasizing that some of the presented factors may be modifiable. This creates the possibility of interventions aimed to improve early dietary habits and even reduce the risk of non-communicable diseases in further life.
Notwithstanding, the present study has some limitations, which should be considered. First of all, the survey was conducted only among Internet users. However, Internet access is generally available in Poland, as well as in Austria. In Poland, 99% of households with children have Internet access, and in Austria, 88% [
31,
74]. Second, all of the data about early feeding factors were self-reported by mothers of toddlers aged 12–36 months and they could have some difficulties in remembering details. Although, existing data suggest that maternal recall is valid years later, whereas information about introducing solids may be poorer reported [
75,
76,
77,
78]; nonetheless, the recall time in the present study was relatively short (≤3 years), therefore, recall bias was minimized. Third, we collected data only about the current use of added salt and sugar. No information about the intake of salt/sodium, free/added sugars, or products that contain high amounts of salt or sugar, as well as the time when salt and sugar were introduced into children’s diet is available. Fourth, there is a likelihood that the present investigation involved more mothers who were especially interested in children’s nutrition, thereupon they could follow the nutritional recommendations to a higher degree. Nonetheless, the present study demonstrated a low adherence to the recommendation of avoiding salt and sugar during complementary feeding, as we observed a high prevalence of use of added salt (especially in the Austrian toddlers) and moderately high prevalence of use of added sugar. Moreover, we found some interesting influencing factors (e.g., related to early feeding practices or maternal concerns about children eating behaviors), which can be directions to develop intervention strategies and educational programs.


 ,
, 



{kind=link}
{kind=link}